
Abstract
Background
California issued stay-at-home (SAH) orders to mitigate COVID-19 spread. Previous studies demonstrated a shift in mechanisms of injuries (MOIs) and decreased length of stay (LOS) for the general trauma population after SAH orders. This study aimed to evaluate the effects of SAH orders on geriatric trauma patients (GTPs), hypothesizing decreased motor vehicle collisions (MVCs) and LOS.
Methods
A post-hoc analysis of GTPs (≥65 years old) from 11 level-I/II trauma centers was performed, stratifying patients into 3 groups: before SAH (1/1/2020-3/18/2020) (PRE), after SAH (3/19/2020-6/30/2020) (POST), and a historical control (3/19/2019-6/30/2019) (CONTROL). Bivariate comparisons were performed.
Results
5486 GTPs were included (PRE-1756; POST-1706; CONTROL-2024). POST had a decreased rate of MVCs (7.6% vs 10.6%, P = .001; vs 11.9%, P < .001) and pedestrian struck (3.4% vs 5.8%, P = .001; vs 5.2%, P = .006) compared with PRE and CONTROL. Other mechanisms of injury, LOS, mortality, and operations performed were similar between cohorts. However, POST had a lower rate of discharge to skilled nursing facility (SNF) (20% vs 24.5%, P = .001; and 20% vs 24.4%, P = .001).
Conclusion
This retrospective multicenter study demonstrated lower rates of MVCs and pedestrian struck for GTPs, which may be explained by decreased population movement as a result of SAH orders. Contrary to previous studies on the generalized adult population, no differences in other MOIs and LOS were observed after SAH orders. However, there was a lower rate of discharge to SNF, which may be related to a lack of resources due to the COVID-19 pandemic, and thus potentially negatively impacted recovery of GTPs.
Keywords
Key Takeaways
• COVID-19 stay-at-home orders had effects on geriatric trauma patients which differed from the effects on the generalized adult trauma population. • Geriatric trauma patients had lower rates of motor vehicle collisions and pedestrian struck after stay-at-home orders. • Geriatric trauma patients had a similar LOS and a lower rate of discharge to SNF, which may be related to a lack of resources due to the pandemic.
Introduction
Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) causing coronavirus disease 2019 (COVID-19) has caused a significant public health threat. Over 84 million people in the US have been infected to date, and the number of cases continues to rise in the face of new variants. 1 In an attempt to mitigate the spread of the virus and decrease population movements, various state-issued directives were implemented, such as a statewide stay-at-home (SAH) mandate issued by the California Governor on March 19, 2020. 2 These restrictions negatively impacted society and the country at large with global financial loss, physiologic stress, and social isolation, 3 which may have contributed to an increase in suicidal ideation, drug abuse, domestic violence, and firearm sales in the US.4-6 Additionally, the trauma population has been affected by the SAH mandate. 7
Several single-center studies have characterized the effects of COVID-19 on trauma volume and mechanisms, demonstrating an increase in penetrating trauma, gunshot wounds, domestic violence, and self-harm and a decrease in motor vehicle collisions (MVCs).5,7-9 More recently, multicenter studies have been able to provide more generalizable data, reporting increased rates of firearm violence and illicit drug use as well as disproportionate changes in trauma volume based on socioeconomic surrogates such as insurance status.4,9,10 In addition, there has been a decrease in length of stay (LOS), thought to be due to increased pressure to discharge patients from overwhelmed hospitals. 9
However, compared to the general population, there is limited data on certain subsets of patients such as pediatric and geriatric trauma patients (GTPs). 11 Geriatric trauma patients represent a particularly vulnerable and consistently expanding trauma demographic that merit further research. 12 Geriatric trauma patients have increased MVC fatality risk and are also the group most vulnerable to COVID-19 mortality, attributed to underlying chronic disease and immunodeficiency. 12 Given this significant health threat, it is possible that elderly patients would more strictly adhere to SAH orders and physical distancing recommendations, which in turn would restrict their driving and mobility. Additionally, GTPs may have had shortened hospital stays during the pandemic as providers attempted to protect this vulnerable population from inpatient COVID-19 exposure. Therefore, we hypothesized a decrease in the rate of MVCs and LOS after the March 19, 2020 SAH orders compared with 2019 historical controls (March 19, 2019, to June 30, 2019) and the immediate time frame preceding the SAH orders (January 1, 2020, to March 18, 2020) in Southern California.
Methods
This study was approved by the Institutional Review Board of the University of California, Irvine, and considered exempt from the need for informed consent. A post-hoc multicenter retrospective analysis of GTPs (≥65 years old) presenting to 11 American College of Surgeons level-I and level-II trauma centers in Southern California was performed. Patients were divided into 3 groups based on their date of injury: before the SAH order from 1/1/2020 to 3/18/2020 (PRE), after the SAH order from 3/19/2020 to 6/30/2020 (POST), and a historical control from 3/19/2019 to 6/30/2019 (CONTROL).
All patients in each trauma center’s registry were included, comprising both trauma activations and trauma consults. The primary outcome was the rate of MVCs, and secondary outcomes were the rate of pedestrians struck and LOS. Demographic data and clinical history were collected including sex (self-reported), age, race (self-reported), insurance status, body mass index (BMI), and comorbidities, which included diabetes, congestive heart failure, cerebrovascular accident, myocardial infarction (MI), coronary artery disease, cancer, end-stage renal disease, chronic obstructive pulmonary disease, dementia, cirrhosis, and smoking status. Injury characteristics and specific mechanisms of injury were recorded, including ground-level fall (GLF), pedestrian struck, motorcycle collision, MVC, assault, sports injury, gunshot wounds, and stab wounds. Injury profile characteristics such as the injury severity score (ISS) and the abbreviated injury scale (AIS) for each body region were calculated. Also, vital signs and examination findings on arrival were obtained. Additional outcomes included intensive care unit (ICU) LOS, ventilator days, packed red blood cells transfused within 4 hours, and fresh frozen plasma transfused within 4 hours. Additional data were collected, including procedures performed, complications, and discharge disposition (home, skilled nursing facility (SNF), long-term acute care hospital, acute rehabilitation, and hospice).
Descriptive statistics were performed for all variables within each group. Categorical variables were reported as percentages of their respective group and continuous variables were reported as means with standard deviation. The POST group was compared with the PRE and the CONTROL groups in 2 separate analyses to account for both seasonal and annual variations. χ2 test was used to compare categorical variables, and either a two-sample t-test or Mann-Whitney U test was used to compare continuous variables. All P-values were two-sided and considered significant if less than .05. This analysis was performed using IBM SPSS Statistics for Windows (version 24; IBM Corp., Armonk, NY).
Results
A total of 5486 GTPs were identified across the 3 periods: 1756 in the PRE group, 1706 in the POST group, and 2024 in the CONTROL group. A total of 12 patients (.70%) within the POST period were identified as COVID positive on laboratory testing regardless of symptoms. Given their relatively small contribution, further subset analysis was not performed on these patients. However, we identified that all 12 patients sustained blunt trauma with the distribution as follows: 9 ground-level falls, 1 fall from height, and 2 MVCs.
PRE vs POST Demographics, Comorbidities, Vital Signs, and Injury Characteristics
Demographics and Comorbidities of Trauma Patients Greater Than 65 Years Old Compared by Time Period.
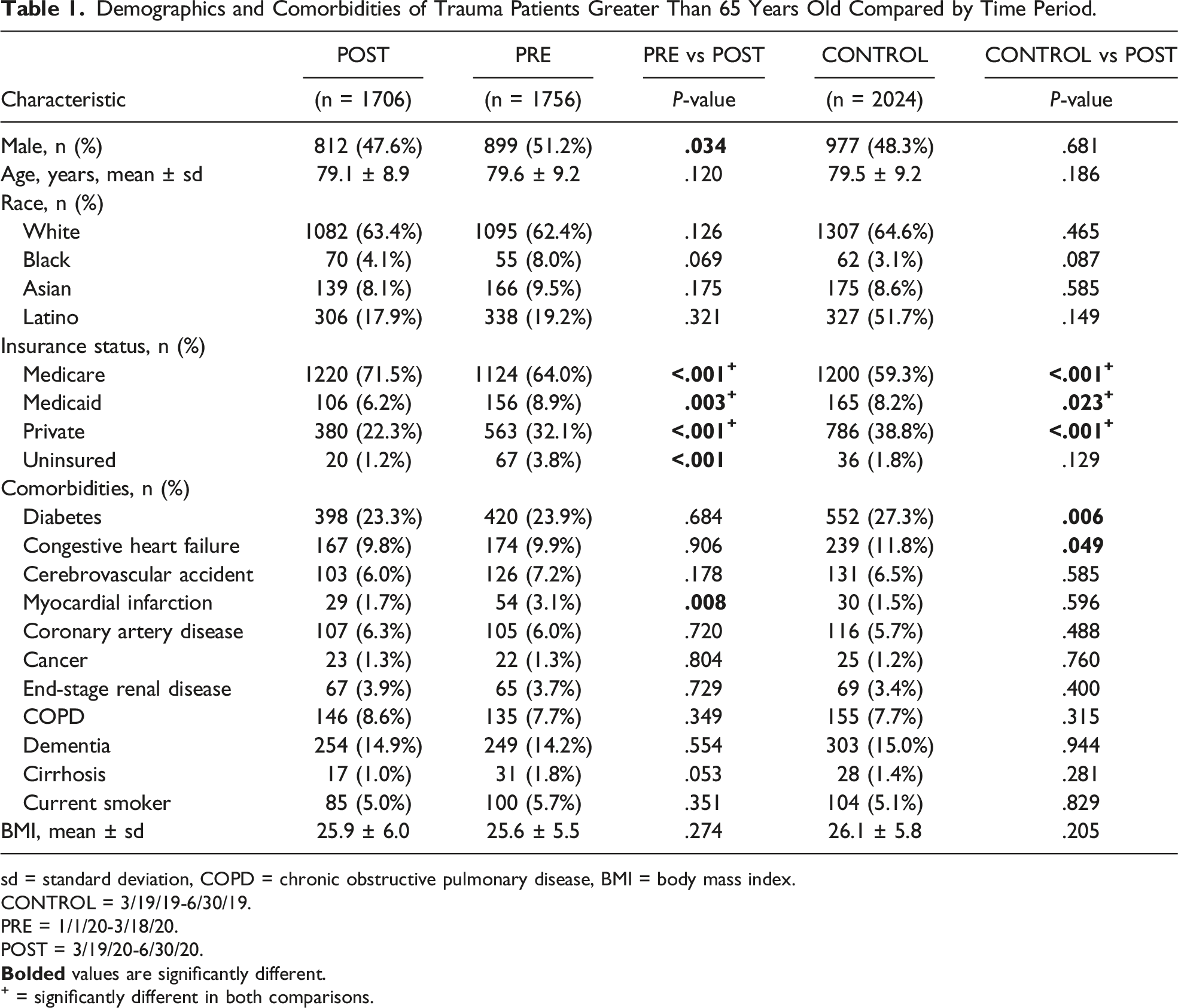
sd = standard deviation, COPD = chronic obstructive pulmonary disease, BMI = body mass index.
CONTROL = 3/19/19-6/30/19.
PRE = 1/1/20-3/18/20.
POST = 3/19/20-6/30/20.
+ = significantly different in both comparisons.
Injury Characteristics and Vital Signs of Trauma Patients Greater Than 65 Years Old Compared by Time Period.
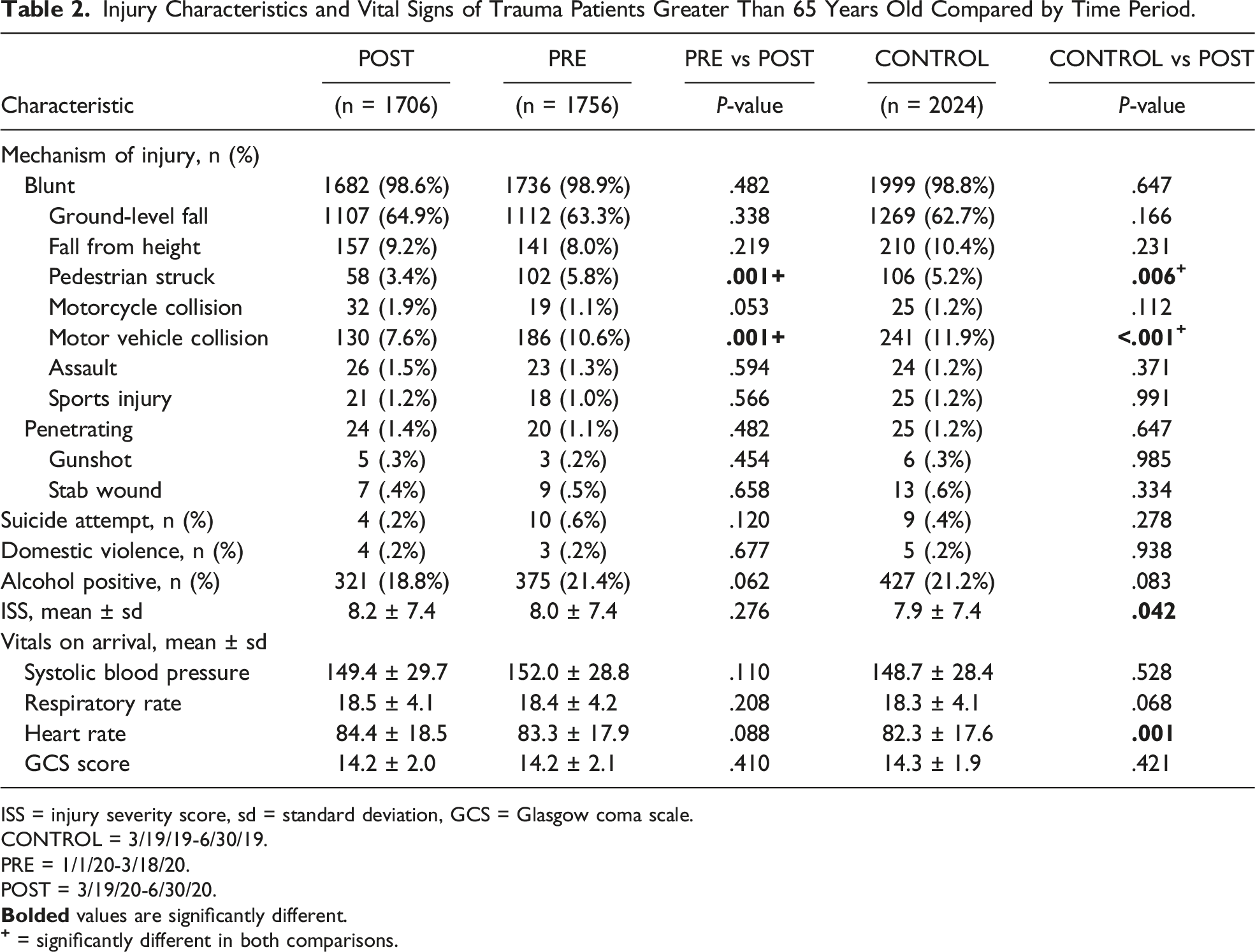
ISS = injury severity score, sd = standard deviation, GCS = Glasgow coma scale.
CONTROL = 3/19/19-6/30/19.
PRE = 1/1/20-3/18/20.
POST = 3/19/20-6/30/20.
CONTROL vs POST Demographics, Comorbidities, Vital Signs, and Injury Characteristics
Compared with the CONTROL group, the POST group had a similar percentage of male patients (47.6 vs 48.3%, P = .68) and similar racial demographics (all P > .05). With regard to insurance status, the POST group had a higher rate of Medicare (71.5% vs 59.3%, P < .001) but a lower rate of Medicaid (6.2 vs 8.2%, P = .023) and private insurance (22.3 vs 38.8%, P < .001). The POST group less commonly had diabetes (23.3 vs 27.3%, P = .006) and congestive heart failure (9.8 vs 11.8%, P = .049). Otherwise, the 2 groups were similar regarding age, BMI, and other comorbidities (all P > .05) (Table 1).
In terms of injury profile, there was a similar rate of blunt (98.6% vs 98.8%, P = .64) and penetrating (1.4 vs 1.2%, P = .64) trauma across cohorts. However, compared with the CONTROL group, the POST group had a lower rate of MVCs (7.6% vs 11.9%, P < .001) and pedestrian struck (3.4 vs 5.2%, P = .006). The POST group also had a statistically lower ISS (8.2 vs 7.8, P = .042) and higher heart rate (84.4 vs 82.3 beats per minute, P = .001) on arrival. Otherwise, the 2 groups were similar in terms of suicide attempts, domestic violence, and vital signs on arrival (all P > .05) (Table 2).
PRE vs POST Outcomes
Outcomes of Trauma Patients Greater Than 65 Years Old Compared by Time Period.
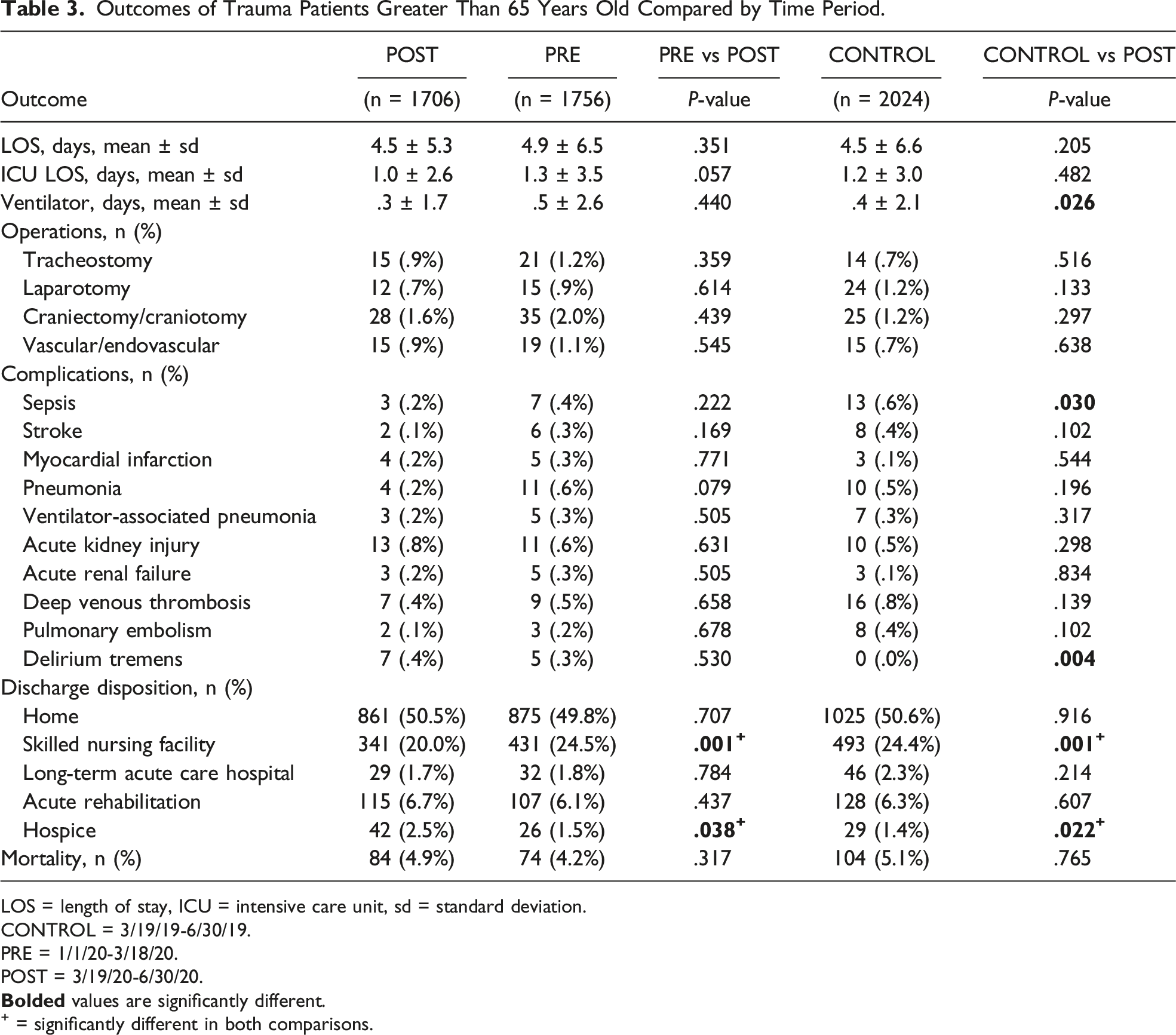
LOS = length of stay, ICU = intensive care unit, sd = standard deviation.
CONTROL = 3/19/19-6/30/19.
PRE = 1/1/20-3/18/20.
POST = 3/19/20-6/30/20.
+ = significantly different in both comparisons.
CONTROL vs POST Outcomes
Compared with the CONTROL group, the POST group had fewer ventilator days (.3 vs .4 days, P = .026), lower rates of sepsis (.2 vs .6%, P = .030), and higher rates of delirium tremens (.4 vs .0%, P = .004). Similar to the PRE group, the POST group had a lower rate of discharge to SNF (20.0 vs 24.4%, P = .001) but a higher rate of hospice (2.5 vs 1.4%, P = .022) when compared to the historical control group. Otherwise, the 2 groups were similar in LOS, ICU LOS, operations performed, and mortality (all P > .05) (Table 3).
Discussion
The COVID-19 pandemic has changed the makeup of the overall trauma population; however, studies focusing on important subsets of trauma patients, including GTPs, which are a growing proportion of trauma patients, are lacking. This multicenter study explored changes in mechanisms and outcomes in GTPs during the start of the Southern California SAH orders. We identified a decrease in MVCs and pedestrian struck and similar rates of penetrating trauma. However, there was a similar LOS across study periods. Interestingly, there was a decreased discharge rate to SNF in the POST cohort compared to both the PRE and CONTROL groups.
Understanding mechanisms of injury is a crucial first step to invest time and resources in the pursuit of injury prevention and quality improvement. 13 We identified a shift in mechanisms of injury for GTPs during the SAH period, namely, a decreased rate of MVCs and pedestrians struck. This finding is corroborated by prior generalized adult single-center studies, public vehicle collision data, and multicenter studies. 9 However, contrary to previous studies on the general trauma population, this study did not find increased rates of penetrating trauma or gunshot wounds for GTPs. 14 Yeates et al 14 identified a notable 21% increase in rates of penetrating trauma and a 24% increase in rates of gunshot wounds among trauma patients of all ages across Southern California. This finding coincides with the general trend of increased firearm violence and firearm-related suicides in the US. Among the elderly, firearm suicides have increased 49% between 2010 and 2018, which is expected to continue as the elderly population grows. 15 The authors stipulated that increased economic and psychological pressure and subsequent rising unemployment may have contributed to the rise in penetrating trauma. Although we lack data to support this conjecture, elderly patients may not have experienced those particular stressors and thus were not as vulnerable to violent penetrating mechanisms of injury.
Geriatric trauma patients present a unique challenge to trauma care providers, including longer hospital stays and greater morbidity and mortality compared to younger patients with a similar ISS. 16 These differences are explained by decreased physiologic reserve, increased comorbid illness, under-triage, and lack of trauma center care. 16 Considering the vulnerability of this population, many trauma centers advocate for early intensive monitoring and early ICU admission for geriatric patients. After adjusting for injury severity, age, gender, and mechanism of injury, one study found a decrease in the overall mortality from 53.8% to 34.2% (P=.003) in the population that received revised protocol care, including early hemodynamic monitoring, trauma team activation, and ICU admission. 17 This highlights the importance of intensive care monitoring in GTPs, a resource that was limited and strained by the COVID-19 pandemic. That said, this study demonstrated similar in-hospital mortality rates across periods, differing from previous studies on the general trauma population.
Length of stay is often multifactorial but may be influenced by comorbidities and age. 17 However, this study on GTPs found a similar LOS across time periods, which is contrary to prior generalized adult studies.14,18 This discrepancy may be due to a push for earlier discharge of healthy adults, related to a lack of resources available due to COVID-19. 14 It is also possible that decreased SNF and post-acute care availability during the pandemic precluded early discharge, which was demonstrated in this current study. Thus, GTPs may have received inadequate post-acute care and/or rehabilitation during the pandemic, which is a crucial factor in the optimal recovery of GTPs.19,20 Future research to evaluate post-acute resource allocation and the long-term impact on the recovery of GTPs affected during this pandemic appears warranted.
There are several limitations to this study. Given the retrospective design and reliance on multiple data collectors, it is possible that key data were entered incorrectly or misclassified. Another limitation is that the period after the California SAH orders, which we defined as March 19, 2020, to June 30, 2020, was diverse over time and across different counties. It contained periods of mandated SAH orders and others with partial reopening, making it possible that we overestimated or underestimated the effects of the SAH order in this study. Also, although we used an earlier 2020 cohort and a historical control from 2019, this study does lack additional historical years to fully account for trends over time. With regard to our analysis, although we attributed most of the changes in the trauma population to COVID-19 and the subsequent SAH orders, it is possible that those changes were in part due to other ongoing societal issues, such as civil unrest related to racial injustice. Additionally, although we attributed decreased discharge to SNF to impaired resources during the pandemic, we did not specifically examine this. It is possible that the observed change in injury pattern, namely, a decreased rate of MVCs and pedestrian struck impacted GTPs’ discharge disposition and SNF placement. However, given that the ISS differences across cohorts were minimal, this seems less likely as injuries typically drive post-discharge disposition rather than mechanisms of injury. Our study is lacking readmission data which may have further elucidated how GTPs’ recovery was impacted by the pandemic and SAH orders. We hope to explore this topic specifically in future work. Finally, this post-hoc analysis only captures the beginning period of the pandemic and thus cannot determine if these effects changed over time. Despite these and other limitations, this is the largest study to the authors’ knowledge to evaluate changes in the geriatric trauma population during the COVID-19 pandemic.
Conclusion
This multicenter retrospective study of 11 American College of Surgeons level-I and II trauma centers in Southern California demonstrated lower rates of MVCs and pedestrian struck for GTPs. Interestingly, we did not identify a shorter LOS, as previously demonstrated in other age groups, possibly due to a lower rate of discharge to SNF. This data suggests the need for additional post-acute resources for GTPs during this and any future pandemic. Further studies with long-term data are warranted to identify the impact of the COVID-19 pandemic on the recovery of injured GTPs.
Footnotes
Author Contributions
All authors contributed to the study conception and design. Material preparation, data collection, and analysis were performed by Eric O Yeates, Areg Grigorian, Natthida Owattanapanich, Galinos Barmparas, Kent Garber, Liz Penaloza-Villalobos, Ann Lin, Ryan Arthur Figueras, Terry Curry, Kathryn B Schaffer, Graal Diaz, Arianne Johnson, Justine Chinn, Ariana Naaseh, Amanda Leung, and Christina Grabar. The manuscript was written by Morgan Manasa. All authors read and approved the final manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.