
Abstract
Nipple adenoma is a rare proliferative lesion that originates from the lactiferous ducts of the nipple. Though it is benign, the typical presentation includes suspicious symptoms—a firm nodule, crusting erosion, and/or discharge from the nipple. These findings can raise concern for malignancy and in particular, Paget’s disease. We report two cases of this uncommon entity, highlighting the variable clinical presentation and keys to the diagnostic evaluation and management.
Keywords
Nipple adenoma (NA) is an epithelial proliferation of the lactiferous ducts of the nipple. The lesion commonly presents as a palpable mass within the nipple and may have an overlying erosion or discharge from the associated ducts. Ultimately, tissue sampling proves a benign entity, but initial signs indicate a concern for breast malignancy.
Case 1
A 44-year-old female without medical morbidities presented with 4 months of pruritus and a palpable mass in the right nipple. Her family history was negative for breast cancer. On examination, she had an excoriation and firm 10 mm mass involving more than 50% of the nipple. Mammography and breast ultrasound (BUS) were reported Breast Imaging Reporting and Data System (BIRADS) category 2, with two simple cysts measuring 14 mm and 20 mm in the ipsilateral breast. She underwent an incisional biopsy of the nipple mass, which revealed NA. Nipple excision was performed to achieve complete resection. Final histopathology showed nipple adenoma with sclerosing and papillomatous patterns (Figures 1).
Case 2
A healthy 35-year-old female with no family history of breast cancer presented with left nipple discharge. Breast examination confirmed pathologic non–bloody serous discharge from a left lactiferous duct orifice and noted a 9 mm shiny mass on the nipple surface. Mammography and a focused left BUS demonstrated a subareolar intraductal mass measuring 4 × 4 × 9mm (BIRADS 4). Core biopsy of the intraductal mass showed a papilloma without atypia. Incisional biopsy of the nipple mass demonstrated nipple adenoma. The patient declined further excision, opting instead for short interval follow-up. Examination at six months revealed that the NA was no longer palpable or visible at the prior biopsy site. Six-month BUS demonstrated an increase in the size of the papilloma to 11 mm, prompting excision. Histopathology confirmed the known intraductal papilloma. At 18 months, the NA remained not palpable or visible on exam, and the patient will continue with a clinical exam in another six months (Figures 2).
Case 3
A 49-year-old female with a personal history of endometrial cancer and family history of breast cancer (sister at age 40) presented with more than one year of intermittent nipple discharge from an enlarged left nipple. On examination, the left nipple was excoriated and dry, with a 7 mm firm hypopigmented mass palpable at the superior nipple surface. Nipple discharge was not present at the time of clinical evaluation. Mammography and BUS were non-contributary. Magnetic Resonance Imaging (MRI) was obtained and showed an enlarged left nipple enhancing homogeneously and without a discreet mass. Genetic testing did not reveal any pathogenic mutations. Incisional biopsy showed nipple adenoma. The patient desired excision with preservation of her nipple. Final histology confirmed benign nipple adenoma, and the cosmetic outcome was favorable.
Discussion
Nipple adenoma is a rare benign epithelial tumor of the lactiferous duct, accounting for just .1-1.7% of benign breast lesions.1,2 The average reported age of presentation is between 40 and 50 years. 3 Nipple discharge is the most prevalent symptom, present in up to 58% of the patients. However, nipple distortion with or without crusting, erythema, thickening, itching, inflammation, and ulceration have been described. 2 Therefore, the differential diagnosis is wide and includes concern for Paget’s, squamous cell carcinoma, and benign entities like eczema, psoriasis, and skin infections. 1
The work up for NA starts with diagnostic mammography and BUS to delineate the extent of the nipple abnormality and to rule out a malignancy. While the mammogram is generally normal, BUS typically shows a well-defined hypoechoic mass with internal vascularity located within the nipple. An incisional biopsy is recommended to establish the diagnosis as these are often not amenable to core biopsy unless they are large at presentation. Nipple adenoma with sclerosing and papillomatosis patterns with a focus of necrosis. Intraductal epithelial hyperplasia is present. Cells show a heterogenous appearance, suggesting against a clonal population, as is seen in DCIS. Shiny 9 mm nodule on the left nipple demonstrating nipple adenoma on incisional biopsy.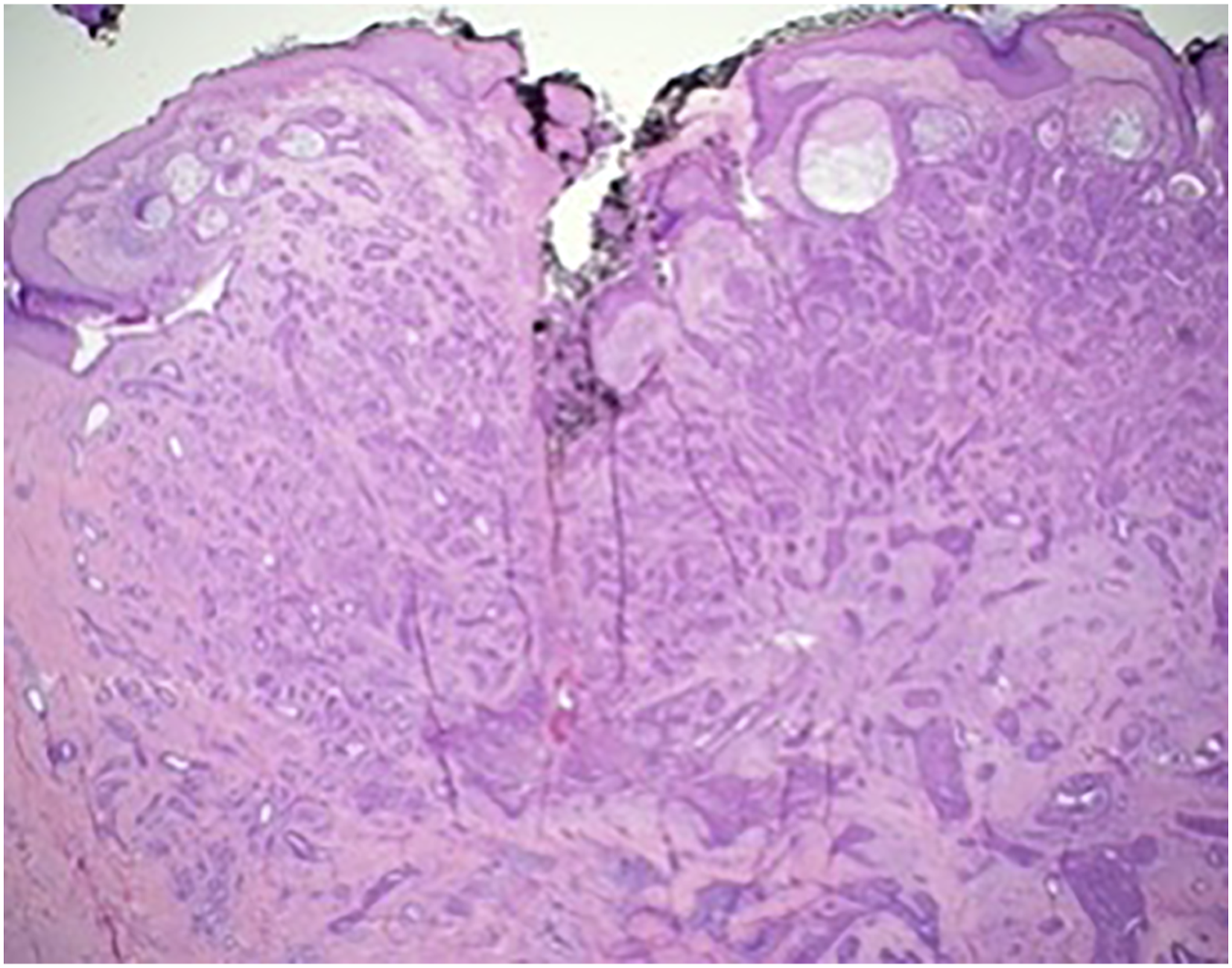

The main histologic feature of NA is ductal proliferation of gland-like structures within the stroma with well-circumscribed borders and without encapsulation. The key to diagnosing NA histologically is to identify two cell populations, epithelial and myoepithelial, the presence of which differentiates NA from carcinoma. 4 There are three main histologic subtypes: (1) Epithelial hyperplasia, with patterns including tubular, solid papillary, and pseudocribriform; necrosis might be present; (2) Adenosis type, where the NA is within the dermis, and (3) Pseudoinfiltrating type, with distorted ducts and squamous cysts without epithelial hyperplasia. 2 Differentiating between subtypes does not have significance with respect to diagnostic workup or management.
Surgical excision to negative margins is the standard treatment to prevent recurrence, but this recommendation can be challenging to accept due to poor cosmesis. Multiple techniques have been described from nipple-preserving to more radical procedures involving excision of the central nipple or complete of the nipple altogether. The key is to ensure complete excision of the NA to avoid recurrence, which has been reported as high as 25 to 55% following incomplete excision. 3
The three cases presented in this report all had varying but suspicious presentations: Case 1 had an excoriated mass lesion, suspicious for Paget’s, Case 2 presented with a shiny palpable nipple mass and serous discharge, and Case 3 had an enlarged nipple with a scaly ulcerated appearance, reinforcing that NA can have variable presentations that can be highly suspicious for malignancy. Though reportedly rare, all three cases presented over a 2-year time frame, suggesting that this entity may be more common and may go unrecognized if not familiar with NA. Lastly, complete excision is reportedly required to successfully manage NA. While Case 1 required removal of the nipple given the extent and position of the NA, Case 3 was able to be managed with preservation of 70% of the nipple, with satisfactory results. Interestingly, in Case 2, the previously palpable and visible lesion (biopsy-proven to be NA) is no longer apparent on examination 18 months after incisional biopsy, suggesting that necrosis or other regression can possibly occur and validating that the growth pattern of these lesions can also be indolent. Regression has not been described previously in the literature for NA.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.