
Abstract
Introduction
While literature widely supports early cholecystectomy for mild gallstone pancreatitis (GSP), this has not been reflected in clinical practice. Early cholecystectomy for GSP with end organ dysfunction remains controversial.
Objective
This study aims to evaluate the rate and outcomes of early cholecystectomy (<3 days from admission) in mild GSP patients with end organ dysfunction (+EOD) and without (–EOD).
Methods
Patients with GSP without necrosis were identified from 2017 to 2019 NSQIP database and categorized into GSP±EOD. Coarsened Exact Matching was used to match patients based on preoperative risk factors in each group, and outcomes were compared.
Results
There was a total of 3104 patients –EOD and 917 +EOD in the aggregate cohort. Early cholecystectomy was performed in 1520 (49.0%) of GSP-EOD and in 407 (44.4%) of GSP+EOD. In the matched cohorts, there were no significant differences in 30-day mortality, morbidity, or reoperation for early cholecystectomy in either group. In GSP-EOD, early cholecystectomy was associated with shorter LOS (2.9 ± 1.5 vs. 5.6 ± 3.0 days, P < .001), shorter operative time (69.7 ± 34.4 vs. 73.3 ± 36.6 min, P = .045), and more concurrent biliary procedures (52.1% vs. 35.4%, P < .001). Similarly, early cholecystectomy in GSP+EOD was associated with shorter LOS (3.3 ± 1.8 vs. 6.9 ± 6.6 days, P < .001), shorter operative time (65.9 ± 32.1 vs. 76.0 ± 40.7, P < .001), and more concurrent biliary procedure (46.0% vs. 34.9%, P = .002).
Conclusions
This study supports early cholecystectomy in patients with mild GSP. Even with end organ dysfunction, early cholecystectomy appears to be safe given there is no difference in morbidity and mortality, and the potential benefit of reduced LOS.
Introduction
Current guidelines support cholecystectomy early in the index admission for patients with mild gallstone pancreatitis (GSP). 1 Most studies evaluating safety of early cholecystectomy in GSP have been performed in patients with mild disease. Mild cases are associated with a 1-3% risk for mortality and early cholecystectomy is recommended to prevent recurrent episodes of GSP or other complications.1,2 Despite the overwhelming evidence accumulated over the past decade supporting early cholecystectomy in mild GSP,3-6 the proportion of patients who undergo cholecystectomy during the index admission has been reported to be as low as 40-51%.6,7
Timing of cholecystectomy for GSP patients with end organ damage is less clear. Patients with organ failure, whether transient (moderately severe GSP per revised Atlanta classifications) or persistent (severe GSP), have higher rates of morbidity and mortality compared to mild cases. 8 Current recommendations are to perform delayed cholecystectomy in patients with end organ damage as there is concern that early cholecystectomy may further exacerbate morbidity and mortality. However, one systematic review found these recommendations are based on low quality evidence. 9
Using a large national database, the purpose of this study is to reaffirm the safety of early cholecystectomy in patients with mild GSP and to determine the safety of early cholecystectomy in patients with more severe GSP as defined by the presence of end organ dysfunction (EOD).
Methods
Based on the International Classification of Diseases, 10th revision (ICD-10) code K85.10, patients with GSP without necrosis were identified from 2017 to 2019 American College of Surgeons National Surgical Quality Improvement Program (NSQIP) database. National Surgical Quality Improvement Program includes peer-controlled, validated clinical data that quantifies 30-day risk-adjusted surgical outcomes from 719 hospitals in 2019 nationwide. Elective outpatient surgeries were excluded. Patients were subsequently divided into two groups: those with end organ dysfunction (GSP+EOD) defined by presence of dyspnea, ascites, acute kidney injury, preoperative ventilator use, preoperative sepsis, and/or preoperative blood transfusion and those without end organ dysfunction (GSP-EOD). Each group was then further subdivided based on those who underwent early cholecystectomy (<3 days from admission) and those who underwent delayed cholecystectomy. Data was collected on patient demographics, perioperative comorbidities, markers of end organ dysfunction, American Society of Anesthesiologists (ASA) class (low ASA class was defined as class I and II), and surgical approach. The primary outcome measures were 30-day mortality, morbidity (presence of any NSQIP-defined postoperative complication), and length of stay (LOS). Secondary outcome measures were operative time, concomitant biliary procedures (common bile duct exploration, intraoperative cholangiogram, or intraoperative endoscopic retrograde cholangiopancreatography), and 30-day readmission and reoperation. The overall rate of early cholecystectomy for GSP was also examined. Given the differences in preoperative characteristics between patients who underwent early vs delayed cholecystectomy, Coarsened Exact Matching with K:K methodology was used to match patients within each group (separately for GSP+EOD and GSP-EOD) based on preoperative characteristics to overcome selection bias. The primary and secondary outcome measures were compared between early and delayed cholecystectomy in both aggregate and matched cohorts.
SPSS V24 (IBM Corp, Armonk, New York) was used to perform statistical analysis. A 2-sided P < .05 was considered statistically significant. Continuous data was compared using the Student’s t test, non-normally distributed data was analyzed using Mann-Whitney U test, and categorical data was compared using Pearson χ2 and Fisher’s exact tests. The Institutional Review Board of Lundquist Institute at Harbor-UCLA Medical Center approved this study and determined that it did not meet criteria of human subject research.
Results
There were a total of 4021 patients included in this study, of which 3104 (77.2%) patients were GSP-EOD and 917 (22.8%) were GSP+EOD. In the total cohort, 1375 (34.2%) were male, 2891 (83.8%) were white, and 886 (23.6%) were Hispanic. The mean age was 52.4 ± 18.9 years. 1612 (40.1%) had simultaneous biliary procedures performed, 3923 (97.6%) underwent laparoscopic cholecystectomy, and 1927 (47.9%) had an early cholecystectomy.
GSP Without End Organ Dysfunction
Demographics and perioperative factors in aggregate GSP-EOD and GSP +EOD.
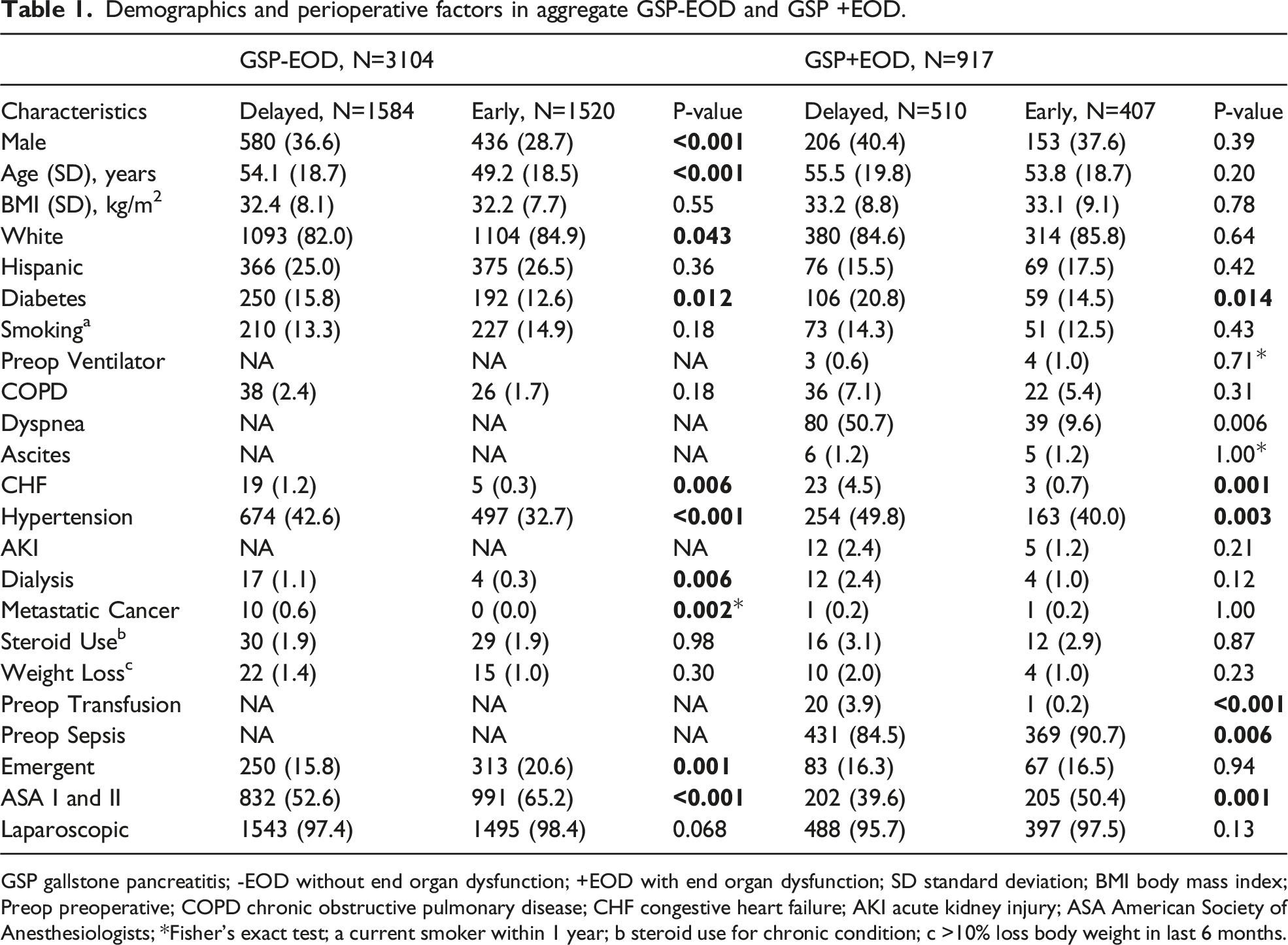
GSP gallstone pancreatitis; -EOD without end organ dysfunction; +EOD with end organ dysfunction; SD standard deviation; BMI body mass index; Preop preoperative; COPD chronic obstructive pulmonary disease; CHF congestive heart failure; AKI acute kidney injury; ASA American Society of Anesthesiologists; *Fisher’s exact test; a current smoker within 1 year; b steroid use for chronic condition; c >10% loss body weight in last 6 months.
30-day Postoperative outcomes for GSP-EOD in aggregate and matched cohort.
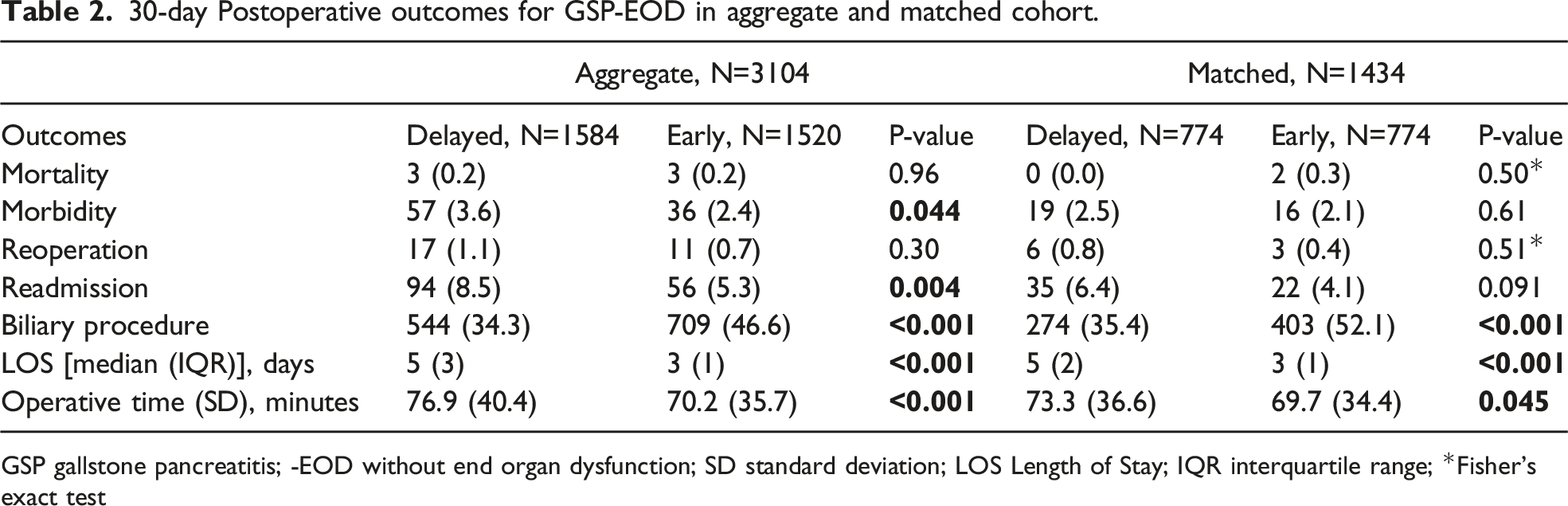
GSP gallstone pancreatitis; -EOD without end organ dysfunction; SD standard deviation; LOS Length of Stay; IQR interquartile range; *Fisher’s exact test
GSP With End Organ Dysfunction
In GSP+EOD, 359 (39.1%) were male, 694 (85.2%) were white, 145 (16.4%) were Hispanic, 407 (44.4%) had early cholecystectomy, 359 (39.1%) had simultaneous biliary procedures performed, and 885 (96.5%) underwent laparoscopic cholecystectomy. Patients with GSP+EOD in the aggregate cohort who underwent early cholecystectomy were more likely to have low ASA class (50.4%. vs 38.6%, P = .001) and preoperative sepsis (90.7% vs 84.5%, P = .001). Those who underwent delayed cholecystectomy were more likely to have diabetes (20.8% vs 14.5%, P = .014), congestive heart failure (4.5% vs .7%, P = .001), hypertension (49.8% vs 40.0%, P = .003), and preoperative blood transfusions (3.9% vs .2%, P < .001) (Table 1). After matching, no statistical differences remained between the two groups.
Baseline Characteristics.
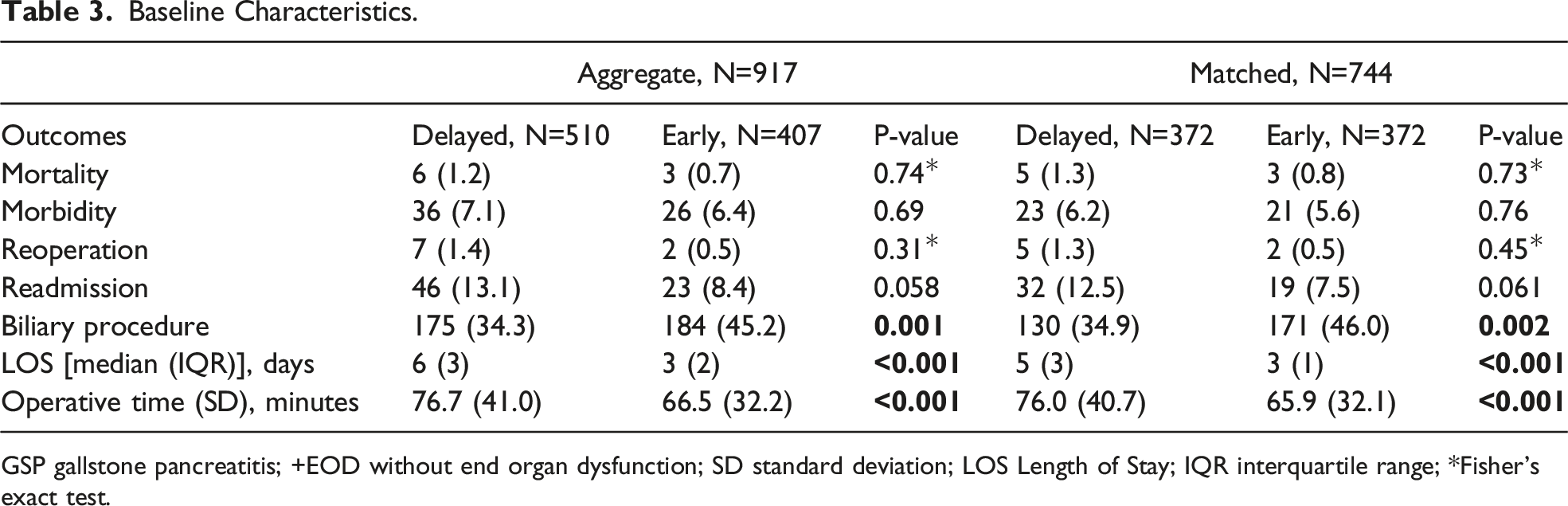
GSP gallstone pancreatitis; +EOD without end organ dysfunction; SD standard deviation; LOS Length of Stay; IQR interquartile range; *Fisher’s exact test.
Discussion
The present study, using a national multicenter database, reaffirmed that early cholecystectomy for patients with mild pancreatitis does not result in increased morbidity or mortality when compared to delayed cholecystectomy. Rather early cholecystectomy is associated with decreased LOS, decreased operative time, and more concurrent biliary procedures. The role of early cholecystectomy was further evaluated in more severe pancreatitis, as defined by evidence of EOD. Similar to mild pancreatitis, early cholecystectomy in those with EOD was associated with decreased LOS and operative time and higher rates of concurrent biliary procedures with no difference in 30-day morbidity, mortality, reoperation, or readmission. These findings add further evidence that early cholecystectomy is safe even with EOD.
This study confirms that one of the major advantages of early cholecystectomy is shortened LOS, observed in both GSP with and without EOD. Early cholecystectomy in patients with mild GSP has previously been shown to be associated with shortened hospital stays without increased risk of morbidity or mortality,3-6,10 in addition to reduce healthcare system costs. 11 In our study, early cholecystectomy was also associated with shorter operative times, although it is unclear whether longer operative times for delayed cases were due to technical challenges from delaying intervention or from the underlying severity of the initial disease. Delaying cholecystectomy for mild GSP has not been proven to lead to more complicated surgery or unnecessary conversion to open approach.6,11
While guidelines support early cholecystectomy for mild GSP, few studies have evaluated optimal timing of cholecystitis in GSP+EOD. One concern regarding early cholecystectomy is that it may lead to an increase in complications and mortality. Historically, high morbidity and mortality in patients undergoing cholecystectomy early in their disease course were attributable to patients with moderate and severe disease, 12 and thus, these patients have since been managed with supportive measures followed by interval cholecystectomy. 1 In this study, there was no increase in morbidity nor mortality for both patients with GSP with and without EOD who underwent early cholecystectomy. This is in line with other studies that have shown early laparoscopic cholecystectomy has not been associated with differences in morbidity, mortality, operative difficulty, or reoperation in patients with mild and in select patients with moderately severe GSP.4,10,13,14 Increased complications and longer hospitalizations have been found to be associated with early cholecystectomy in more severe GSP cases with presence of fluid collections that required further management or progressed to infected pseudocysts. 15 However, early cholecystectomy may be safe in more severe cases of GSP without necrosis given the findings of this study.
Despite increasing evidence to support early cholecystectomy for GSP, many patients still have delays in surgery. Early cholecystectomy was performed in just under half (49.0%) of patients with GSP-EOD, despite guidelines supporting early cholecystectomy for mild GSP. In GSP+EOD, early cholecystectomy was even lower (44.4%), which may reflect treatment strategies of supportive management and delayed cholecystectomy for this group of patients. In previous studies, delay in surgery has also been attributed to patient factors such as old age and presence of comorbid conditions, as well as lack of initial surgical consultation.1,16
Despite using a large national sample, this study had limitations. Our sample size decreased after matching, potentially contributing to type II errors. The database did not provide data on reasons as to why surgery was delayed in patients who did not receive early cholecystectomy, so it is difficult to conclude why this significant delay for GSP patients exists. Data was also limited to the institutions contributing to the NSQIP database and may not be applicable to all hospital settings. End organ dysfunction in this study was determined by presence of various perioperative factors available in the database and not based on published risk calculators that are often used to stratify severity of acute pancreatitis. 17 Additionally, transient and persistent end organ dysfunction could not be differentiated, and thus, these findings may not directly reflect outcomes of moderate or severe GSP. Further research is needed to evaluate factors contributing to low rates of early cholecystectomy in GSP and to the safety of performing early cholecystectomy in GSP.
In conclusion, cholecystectomies early in the index hospitalization do not confer increased risk for morbidity, mortality, reoperation, or readmission in non-necrotic GSP with and without EOD. In additional to being safe in mild GSP, early cholecystectomy appears safe in GSP with EOD provided there is no evidence of pancreatic necrosis. Despite safety of early cholecystectomy in non-severe GSP, most patients do not undergo early cholecystectomy early in admission. Further studies will be helpful in evaluating factors contributing to improved outcomes with early cholecystectomy in both GSP with and without EOD, and ultimately, increasing the rate of patients with GSP undergoing early cholecystectomy when appropriate.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.