
Abstract
Introduction
Clostridium difficile is an anaerobic, spore-forming bacillus, which is the most common pathogen associated with nosocomial infections and is the leading cause of diarrhea in hospitalized patients. 1 In the United States, a recent national survey demonstrated that Clostridium difficile infection (CDI) accounts for 15% of all health care-associated infections. 2 Furthermore, CDI is associated with substantial burden on the U.S. health care system. 3 In the last two decades, the dramatic increased incidence and severity of CDI has created a worsening public health challenge.4,5 Moreover, the incidence of CDI has increased among surgical patients in the United States.6-9 Specifically, there has been identified a higher rate of CDI following colorectal and orthopedic surgery. 10 Meanwhile several studies have shown higher in-hospital mortality rate, postoperative complications, prolonged hospitalizations, and hospital cost among surgical patients who develop CDI.3,11,12 However, there has not been such a study investigating CDI rate and outcomes among common laparoscopic abdominal surgeries.
Since the American College of Surgeons National Surgical Quality Improvement Program (ACS-NSQIP) database allocated a specific variable to capture CDI following surgical procedures in 2015, in this study we aimed to determine the incidence and outcome of CDI among laparoscopic abdominal surgery using a national database, hypothesizing that laparoscopic colorectal operations are correlated with higher CDI incidence compared to other common laparoscopic abdominal surgeries.
Materials and Methods
The 2015 to 2019 ACS-NSQIP database was reviewed to evaluate adult (≥18 years-old) patients who developed CDI following laparoscopic abdominal operations including colorectal surgery, bariatric surgery, cholecystectomy, esophageal surgery, appendectomy, and abdominal wall hernia repair. Patients with a diagnosis of disseminated cancer were excluded. Patients were divided into two groups CDI and Non-CDI for comparison of the outcomes. As this is a national deidentified database this study was deemed exempt for IRB approval and a waiver of consent granted.
Variables used in the analysis were provided by the NSQIP database and included patient demographics (age, sex, and race), American Society of Anesthesiologists Physical Status (ASA) score, as well as patient comorbidities including moderate or severe dyspnea, ascites, diabetes mellitus requiring medication, chronic steroid use, history of severe chronic obstructive pulmonary disease (COPD), weight loss more than 10% in last six months, preoperative pneumonia, preoperative acute renal failure, preoperative history of smoke, preoperative wound infection, preoperative sepsis, preoperative history of dialysis, and hypertension requiring medication.
The outcomes evaluated were overall 30-day morbidity and 30-day mortality, surgical site infections (SSI), venous thromboembolism (VTE), pneumonia, unplanned intubation, ventilator dependency more than 48 hours, urinary tract infection, sepsis, septic shock, acute renal failure, unplanned operation, unplanned readmission, and hospital length of stay more than 30 days. Outcomes were evaluated based on the predefined CDI and Non-CDI groups. In addition, the incidence of CDI was calculated across different operations. Risk adjusted analysis was performed to identify associations between CDI and postoperative complications following surgery.
Statistical analysis was performed with SPSS® software, Version 23 (SPSS Inc., Chicago, IL). Logistic regression analysis was used to estimate the association between CDI and each outcome, including 30-day day mortality and all of the considered postoperative complications. P values less than .05 were considered statistically significant. For each outcome, the adjusted odds ratio (AOR) with a 95% confidence interval were calculated and reported to estimate the relative risk associated with CDI. Adjustments were made based on univariate analysis results for hypertension, dyspnea, emergent admission, ASA score more than two, steroid use, COPD, weight loss, ascites, age, sex, and race.
Results
A total of 973 338 patients were studied and the overall incidence of CDI was .3% within 30 days of operation. Of these, the CDI rate was highest for colorectal surgery at 1.0% (1601 of 167 949) and lowest following hernia repair at .1% (144 of 154 389). The CDI rate was .3% following esophageal surgery (96 of 36 799), .3% following appendectomy (628 of 213 706), .2% following cholecystectomy (461 of 278 273), and .2% following bariatric surgery (195 of 121 470). For patients with CDI, mean length of stay (8 ± 9 days) was longer for colorectal operations compared to other abdominal operations (Esophageal 6.5±7.1, Cholecystectomy 6.1±7.1, Bariatric 4.8±7, Hernia 5.2±7.7, and Appendectomy 4.2±5.5, P < .01).
Demographics and Comorbidities of Patients Who Underwent Laparoscopic Abdominal Operations in the United States, 2015-2019(CDI vs Non-CDI).
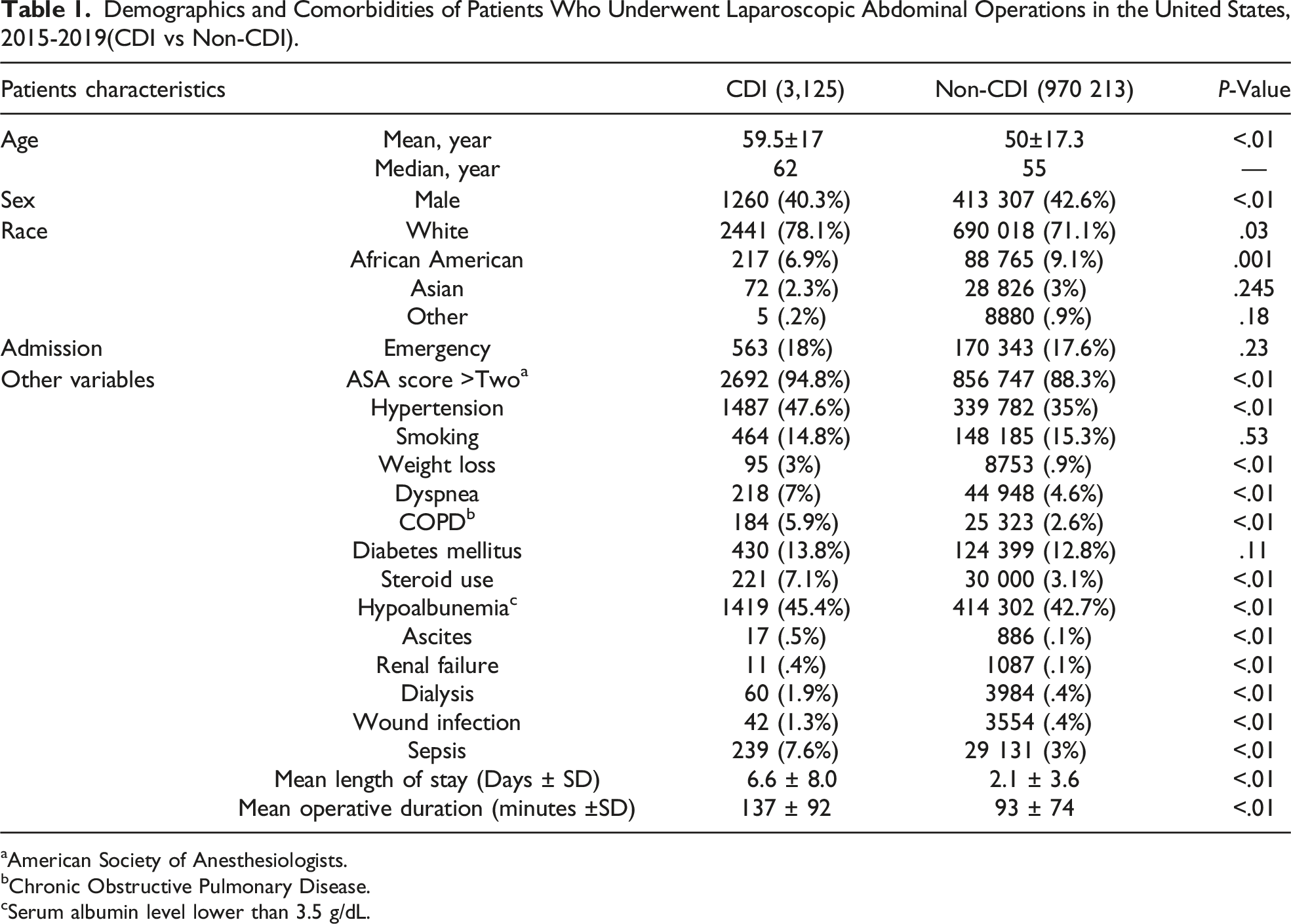
aAmerican Society of Anesthesiologists.
bChronic Obstructive Pulmonary Disease.
cSerum albumin level lower than 3.5 g/dL.
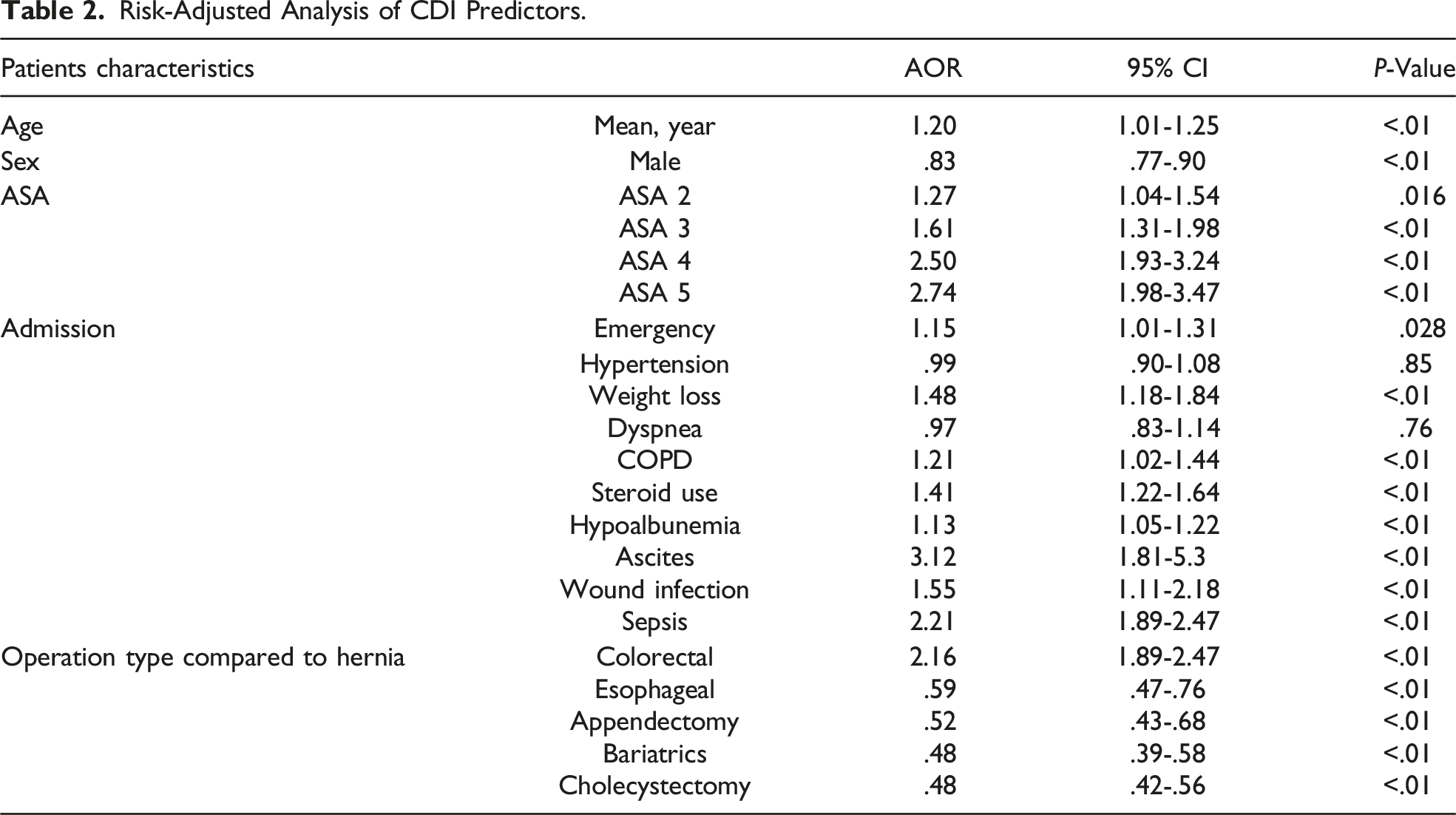
Risk-Adjusted Analysis of CDI Predictors.
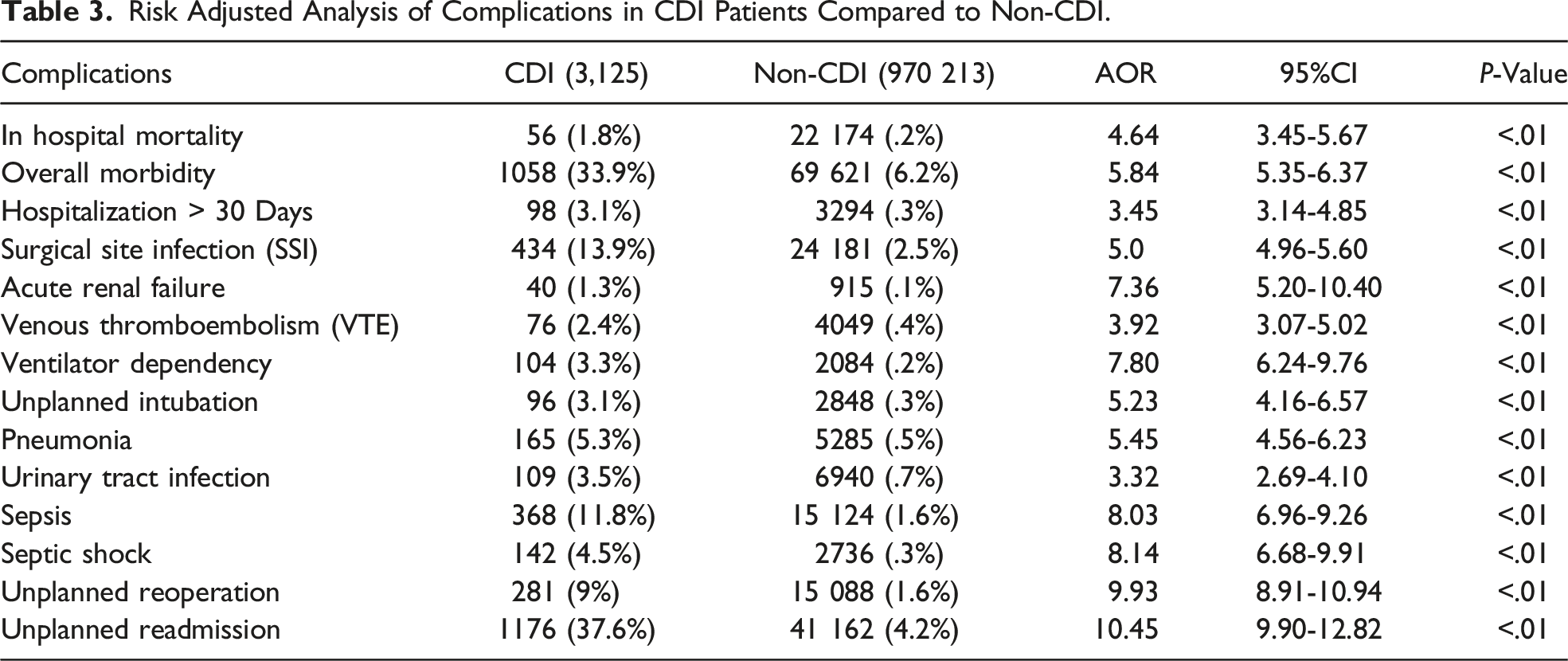
Risk Adjusted Analysis of Complications in CDI Patients Compared to Non-CDI.
Finally, on multivariate analysis, a comparison of the likelihood of developing CDI following common laparoscopic abdominal procedures demonstrated the odds of developing CDI was significantly higher following colorectal surgery compared to all other surgeries (AOR 2.16, CI 1.89-2.47, P < .01) (Figure 1). Adjusted odds of developing CDI by surgical procedure relative to hernia repair. On multivariate analysis, the odds of developing CDI was significantly higher following colorectal surgery compared to all other surgeries (AOR 2.16, CI 1.89-2.47, P < .01).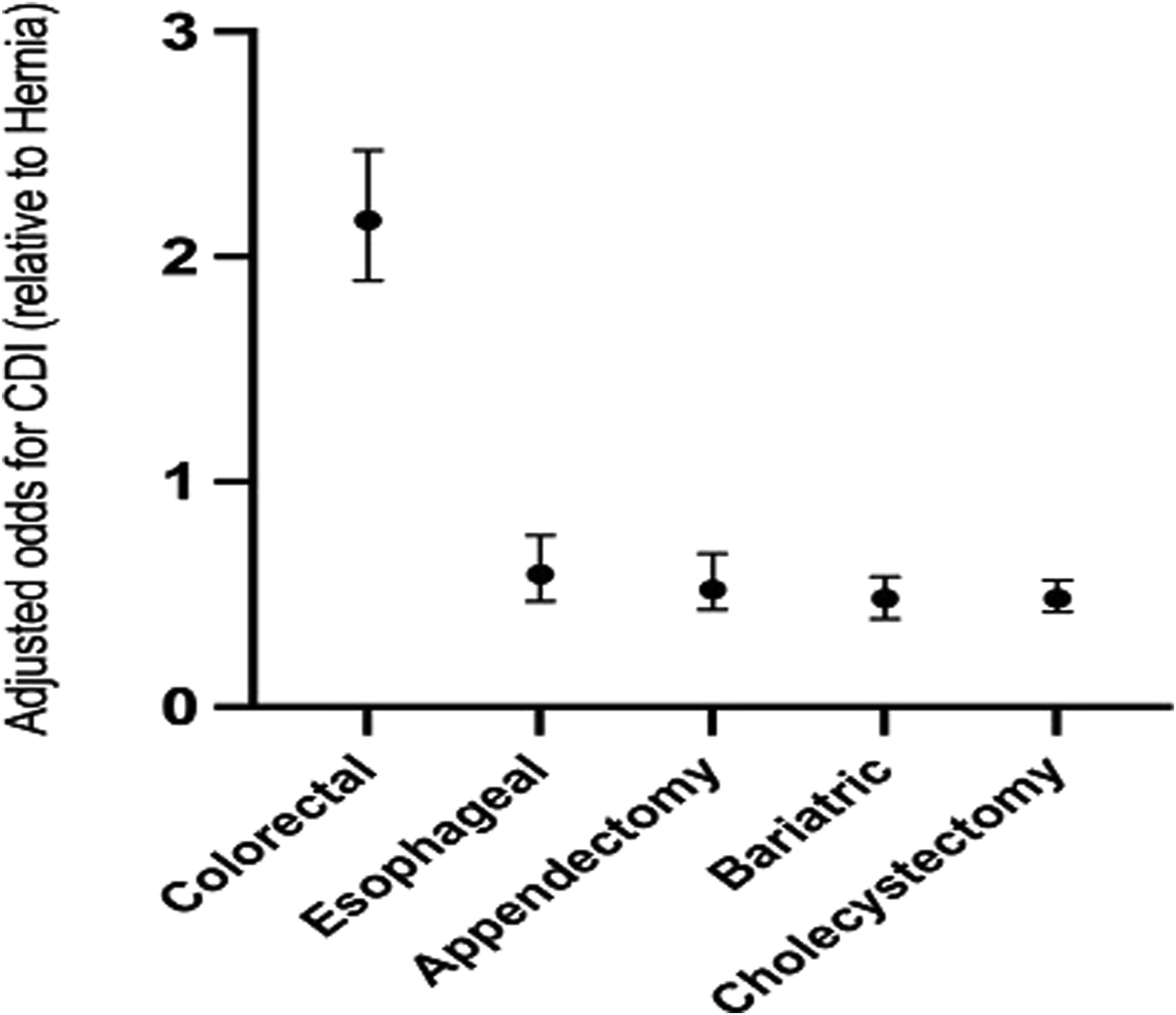
Discussion
Clostridium difficile infection remains a substantial burden on the healthcare system and is associated with increased morbidity and mortality following laparoscopic. While prior reports have identified risk factors, in this study, it is the first-time using ACS-NSQIP database to focus on five major laparoscopic procedures including colorectal surgery, bariatric surgery, cholecystectomy, esophageal surgery, and appendectomy and abdominal wall hernia repair to explore to investigate the incidence of CDI and how CDI affects the surgical outcome.
The overall incidence rate of CDI among nearly 1 million patients undergoing laparoscopic surgery was .3%, which is lower than prior published incidence rates. Zerey M et al reported .52% CDI incidence rate at U.S. hospitals for patients undergoing a general surgical procedure from 1999-2003. 6 Moreover, a prospective, population-based study by Abdelsattar Z et al found that .51% patients undergoing surgery including amputation, endocrine, gynecologic, and general procedures developed a hospital-acquired postoperative CDI. 10 Another study found that the overall incidence of CDI was low with .13% developing CDI after laparoscopic bariatric surgery, 13 which indicated the difference in the overall incidence of postoperative CDI among different types of procedure. For instance, the study by Abdelsattar reported that incidence rate of CDI was as high as 2.6% after lower-extremity amputation. 10
The incidence rate of CDI in patients undergoing colorectal surgery is 1% in our current study, which is consistent with other studies.6,10 In the hospitalized population, immune-compromised status, exposure to C. difficile spores and disrupted normal colonic microbiome are main risk factors for CDI. 14 Previous studies have shown that gastrointestinal surgery, particularly colorectal surgery is associated with CDI. 15 High incidence rate of CDI among colorectal operations might be explained by disruption of the gut microbiome by maybe bowel prep and/or surgical procedure on the colon itself. 16 Antibiotic use can have several negative effects on the gut microbiota, including reduced species diversity, altered metabolic activity, and the selection of antibiotic-resistant organisms, which in turn can lead to antibiotic-associated diarrhea and development of CDI. 17
Our study demonstrated that other risk factors for CDI development included preoperative ascites, higher ASA score (>2), preoperative sepsis (AOR 2.21, P < .01), preoperative wound infection, preoperative weight loss, male gender, steroid use, and hypoalbumenia which is similar to previously published study which was conducted in veteran health administration. 18
Also, we found that people who develop postoperative CDI have higher in-hospital mortality rate, postoperative complications, prolonged hospitalizations which is consistent with previously published studies investigating patients among various surgical specialties.11,18 These findings emphasize on use of risk stratification tools to identify the perioperative risk of CDI development and aids in clinical triage, decision making, and quality assessment in a wide variety of surgical fields. This can be combined with appropriate antibiotic stewardship program interventions for patients at risk for CDI.
There are several limitations in this study. The main limitation is the retrospective nature of our study that prevents the ability to identify causation. The wide variation in hospital setting, hospital quality, and surgeons’ expertise in a nationwide database can also confound data from this study but alternatively allows better generalizability. Also, there is no available data in NSQIP database regarding the antibiotic regimen perioperatively and any antibiotics that were given later in the hospital course. Despite these limitations, our study is one of the largest samples of the impact of CDI on common laparoscopic abdominal operations to date.
Conclusion
Postoperative CDI continues to be cause of morbidity for common laparoscopic surgery including increased length of stay, postoperative complications, and mortality. Furthermore, laparoscopic colorectal surgery appears to have the greatest risk. Future research is needed to determine the exact cause in order to decrease the incidence of CDI by reconsidering the protocol of antibiotic use within the high-risk population.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.