
Abstract
Introduction
Body mass index (BMI) has been established as an independent risk factor for complications after abdominal hernia repairs. While various thresholds have been proposed, there is no consensus for an ideal BMI for elective hernia repair.
Objective
To identify the BMI threshold at which risk for hernia recurrence is significantly increased in patients undergoing ventral and incisional hernia repair.
Methods
This retrospective review of medical records included patients who underwent ventral or incisional hernia repairs from 2014 to 2020 at a single institution. Patients with hernia defects ≥4 cm were included. The primary outcome measure was hernia recurrence. Classification and Regression Tree (CART) analysis was used to determine the BMI threshold for recurrence. Bivariate and multivariate analyses were used to validate the threshold and to evaluate factors associated with recurrence.
Results
Of the 175 patients included, 9.1% had a recurrence. Classification and Regression Tree analysis identified BMI 35.3 kg/m2 as the critical threshold for hernia recurrence. In bivariate analysis, compared to patients who had no recurrence, patients with recurrence were more likely to have cirrhosis (12.5% vs 0%, P = .008), incarcerated hernias (75.0% vs 31.4%, P = .001), urgent surgery (75.0% vs 22.0%, P = <.001), biologic and no mesh use (25.0% vs 6.4% and 12.5% vs 5.7%, P = .012), and BMI >35.3 kg/m2 (75.0% vs 25.8%, P < .001). In multivariate regression, only BMI >35.3 kg/m2 was associated with recurrence [OR: 20.58 (95% CI: 2.17-194.87), P = .008].
Conclusion
Body mass index >35.3 kg/m2 was the only independent factor associated with hernia recurrence. This highlights the importance of determining a BMI threshold for patients undergoing ventral or incisional hernia repair.
Introduction
Ventral hernias have risen in incidence and cost over the years with complications after repair such as hernia recurrence contributing to these trends. 1 Obesity along with abdominal wall hernias have become more common in the United States and are expected to continue to rise in prevalence. 2 Not only has obesity been shown to increase the risk of developing ventral and incisional hernias, 3 but it has also been established as an independent risk factor for higher overall complications, surgical site infections, surgical site occurrences, and urgent ventral hernia repairs.4-6
To mitigate the increased risk of poor outcomes associated with ventral hernia repair in patients with obesity, patients are often encouraged to lose weight or meet body mass index (BMI) cutoffs, which may be difficult to achieve. 7 Increased BMI may also contribute to patients being overly represented in cohorts of emergent repairs of abdominal wall hernias putting these patients at higher risk of complications. 8 Given these concerns, ideal BMI thresholds for repairing ventral hernias should be carefully evaluated to reduce risk of major complications and hernia recurrence.
While various thresholds have been proposed, there is no consensus for an optimal BMI for elective hernia repair to prevent hernia recurrence as very few studies have data on long-term recurrence.9,10 The primary objective of this study is to identify the BMI threshold at which risk for hernia recurrence is significantly increased in patients undergoing ventral and incisional hernia repair. Our secondary outcome is to identify additional factors that are associated with increased rates of hernia recurrence.
Methods
This is a single-center retrospective observational study on patients who underwent a ventral or an incisional hernia repair from 2014 to 2020 at an urban, tertiary referral, safety-net hospital. Patient data were obtained from electronic medical records. The following Current Procedural Terminology (CPT) codes were used to identify patients who underwent ventral or incisional hernia repair: 49560, 49561, 49565, 49566, 49568, 49570, 49572, 49585, 49587, 49652, 49653, and 49655. Diagnoses were confirmed with chart review. Patients with a single or cumulative ventral or incisional hernia defect size of ≥4 cm were included. Those with umbilical or spigelian hernias were excluded. Patient demographics including age, sex, ethnicity, and race were collected. Comorbid conditions (BMI, tobacco use, diabetes, hypertension, cardiovascular disease, pulmonary disease, chronic kidney disease, and cirrhosis), operative factors (initial or recurrent hernia; reducible, incarcerated, or strangulated hernia; presence of intestinal obstruction; concurrent bowel resection; and mesh type and location), surgical approach (open or minimally invasive), and acuity (elective or urgent) were included in the analysis. Mesh type and type of repair was the choice of the individual surgeon.
Classification and Regression Tree (CART) analysis was used to determine the BMI threshold at which risk of hernia recurrence was significantly increased. Classification and Regression Tree analysis is a tree-building model that applies a dichotomous split in the dependent or explanatory variable, in this case, hernia recurrence, based on independent predictors, in this case, BMI. This technique demonstrates the relationship of variables in terms of explanatory power and variance, and in turn, is useful for informing further intervention. 11 Bivariate and multivariate analyses were used to validate the BMI threshold and to evaluate other perioperative factors associated with recurrence. A 2-sided P < .05 was considered statistically significant. Continuous data were compared using the Student’s t-test, and categorical data were compared using Pearson χ2 and Fisher’s exact tests as appropriate. Multivariate regression was used for any variable with P < .1 in initial bivariate analysis. SPSS, version 24 (IBM Corp, Armonk, New York), was used to perform statistical analysis. The Institutional Review Board of Lundquist Institute at Harbor-UCLA Medical Center approved this study and determined that it did not meet criteria of human subject research.
Results
There were a total of 175 patients who underwent ventral or incisional hernia repair from 2014 to 2020 for a hernia defect ≥ 4 cm. The mean age was 53.6 years (SD = 10.6) and mean BMI was 33.4 kg/m2 (SD = 6.0). In the group, 64 (36.6%) were male, 15 (8.6%) were white, 29 (16.6%) were black, 128 (73.1%) were Hispanic, 2 (1.1%) were Asian/Pacific Islander, and 1 (.6%) did not specify their race or ethnicity. The overall rate of hernia recurrence was 9.1%. Recurrences occurred at a median of 400 (IQR = 34-876) days after the initial operation. Median follow-up from initial operation was 538 days (IQR =86-1001).
Bivariate Analysis of Patient Demographics, Comorbidities, and Operative Factors Associated With Hernia Recurrence.
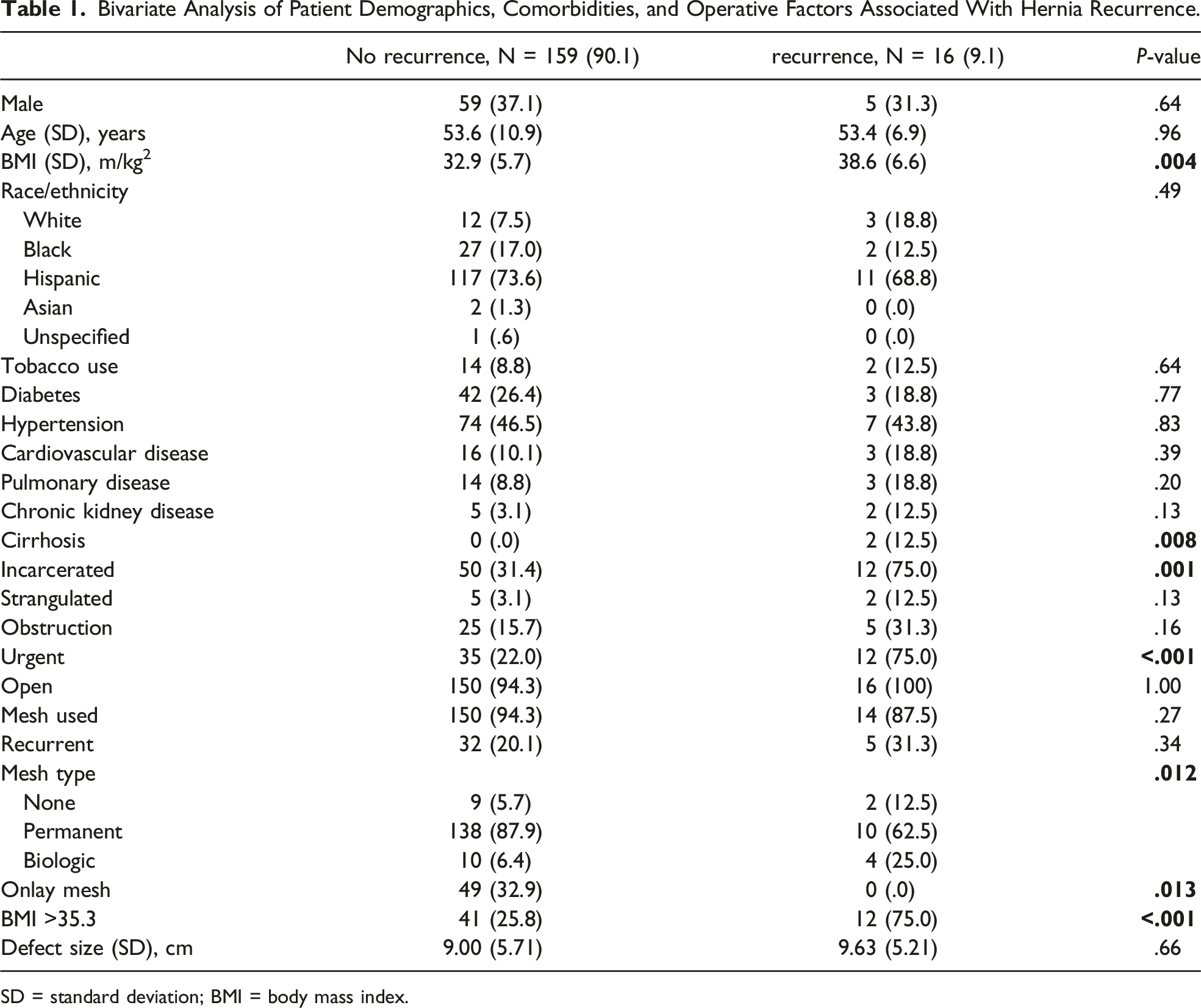
SD = standard deviation; BMI = body mass index.
Discussion
This study found that a BMI >35.3 kg/m2 is independently associated with hernia recurrence in patients presenting with ventral or incisional hernias with a defect of at least 4 cm. Risk factors associated with hernia recurrence included cirrhosis, incarcerated hernia, urgent surgery, primary repair, use of biologic mesh, and elevated BMI. However, the only factor independently associated with recurrence was BMI >35.3 kg/m2.
Our finding of a higher BMI, particularly a BMI >35.3 kg/m2, being significantly associated with recurrence is consistent with prior studies that demonstrate the association of obesity with increased complications. The stepwise relationship between increasing BMI and complications after ventral hernia repair has been demonstrated in multiple studies.12,13 However, no clear BMI threshold has been established for preventing hernia recurrence or other complications. Previous published studies show that patients with BMIs ≥30 to ≥40 kg/m2 are associated with postoperative complications after ventral or incisional hernia repairs.9,10,14 The wide-ranging BMI cutoffs could be attributable to a variety of perioperative factors influencing patient outcomes in different hospital settings and rather highlights the importance of individually tailoring preoperative evaluation prior to ventral hernia repair in obese patients.
Our institution currently uses a BMI cutoff of 35 kg/m2 or less as criteria for accepting patients for elective ventral hernia repair. While the cutoff was arbitrarily chosen for our patient population based on the previous literature, concerns remained that in our primarily underrepresented minority patient population, this working BMI cutoff may have been unnecessarily delaying or denying patients access to repair of their ventral or incisional hernias. Even with a BMI cutoff of 35 kg/m2, there were still patients presenting above the threshold for hernia repair with the maximum BMI ranging up to 58.3 kg/m2. However, patients who present in our clinics with a BMI >35 kg/m2 are typically recommended to lose weight with diet and exercise or a structured weight loss program prior to scheduling surgery. Requiring preoperative weight loss can delay treatment or result in patients presenting for urgent hernia repair, increasing the risk for higher morbidity, mortality, and health care costs. 3 Nonsurgical interventions for weight loss in obese patients have been unsuccessful in most patients, particularly in one study using patients from a safety-net urban hospital.10,15 While our patients can be referred to a weight loss program located at another medical campus, some of our patients have difficulty completing these referrals as they require additional transportation, time off from work, or time away as a caregiver. Mrdutt et al 8 found that obese patients are over-represented in emergent ventral hernia repairs, experience worse outcomes, and are at increased risk for hernia recurrence. For these reasons, the risk of recurrence and other complications after hernia repair should be carefully weighed against the risk of delaying care in obese patients.
Our study found several additional risk factors were associated with hernia recurrence including cirrhosis, incarcerated hernia, urgent surgery, primary repair, and use of biologic mesh. Repair with biologic mesh or primary repair over use of synthetic mesh and presence of cirrhosis has been established as a risk factor for recurrence,16-18 while patients presenting with incarcerated hernia and urgent surgery have increased risk of postoperative morbidity. 19 However, once these factors in this study were controlled for in multivariate regression analysis, only BMI ≥35.3 kg/m2 was independently associated with hernia recurrence emphasizing the significant impact that obesity can have in ventral hernia repair outcomes.
This study had limitations. The study was retrospective in nature, limiting data collection to the information provided in the electronic medical record. While mesh location and recurrent ventral hernia could be easily extrapolated from chart review, hernia defect size was not consistently reported in operative notes. Patients were excluded if the dimensions of the defect were not recorded. Additionally, the choice of operation and location and type of mesh used was surgeon dependent. The study size was small after excluding patients based on inclusion criteria and missing key variables. It is possible that some of the variables that were significant in bivariate analysis or variables that approached significance could become significant with a larger sample size. A larger, multicenter study or prospective clinical trial could validate the findings of this study and reveal additional risk factors associated ventral hernia recurrence.
Presently, few studies evaluate long-term outcomes of ventral and incisional hernia repairs. An advantage of this study was that patients could be followed over the study period as long as they continued their medical care at our institution. Further analysis would aid in determining specific risk factors and BMI thresholds for other operative outcomes as this could influence how patients are optimized for surgery and counseled on their preoperative risk.
Conclusions
In our patient population, patients with BMI >35.3 kg/m2 are at significantly increased risk for ventral hernia recurrence. This suggests that patients with BMIs above this threshold should be appropriately counseled on the risk of recurrence and, if feasible, encouraged to lose weight to avoid recurrence. Body mass index proves to be a significant influence on operative outcomes after ventral hernia repair. This highlights the importance of determining specific evidence-based BMI thresholds for specific patient populations rather than broadly applying arbitrary cutoff points, which may not be applicable or attainable, or affect outcomes in specific patient populations.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.