
Abstract
When Benjamin Franklin published the mortality rates from smallpox during the Boston smallpox epidemic of 1752, he revealed that Blacks not only had a higher mortality rate from smallpox (12.8%, 62/485; 8.9% for whites, 452/5,059), but once inoculated, had less protection from fatal disease (mortality rate 5.0%, 7/139; 1.2% for whites, 23/1,954). His report was thus the first publication to document racial disparities in a disease and its treatment. The differential outcomes came about in the context of slavery, poverty, and war, the predecessors of the social determinates of health that we observe today.
During the 1752 outbreak only 28 percent of the Boston’s occupants were inoculated, a level that failed to protect the community. When the contagion returned in 1764, the town selectmen decided to provide inoculations at no cost to all that needed them. That year inoculated smallpox reached 87 percent of the total caseload. “This lowered the death rate for smallpox so markedly,’ wrote John Blake, historian at the National Library of Medicine, ”that for the first time a smallpox year failed to stand out as one of unusual mortality.”
One final observation came from Franklin’s data: the unexpectedly high prevalence of inoculations among Blacks (6.8% of those inoculated, 146/2,143; 8.5% of all those contracting the disease, 693/8,201). Boston’s whites had made certain enslaved Blacks were inoculated, evidence the extent to which slavery was essential to the economy of colonial Boston.
Slavery
James Hardesty of Western Washington University wrote on the lives of blacks in colonial New England. 1 From its beginnings when Native American war captives were traded for enslaved blacks from the Caribbean in 1638, white New Englanders were actively engaged in the importation, sale, and trade of enslaved persons from Africa.
Joanne Pope Melish of the University of Kentucky wrote on the impact of slavery on the economic development of colonial New England. 2 Enslaved blacks were critical to the transformation of New England’s economy from subsistence production and craft enterprises to manufacturing, trade, and a market economy. With enslaved workers tilling fields and doing routine housework, heads of households were freed to pursue artisan and professional occupations, entrepreneurial endeavors that thrived from the work of still more enslaved blacks. “By 1774,” Melish wrote, “half of all ministers, half of all lawyers and public officials, and a third of all doctors owned slaves; about two-thirds of persons leaving estates valued at more than £2000 owned slaves. 2 ”
“Black New Englanders were fixtures in the social fabric of the region,” Hardesty wrote. 1 Boston itself was “a crowded cosmopolitan port town where Africans could easily mingle with whites, Native Americans, and other Africans. 1 ” By 1752, there were 1541 persons blacks in Boston, nearly 10% of the city’s 15,730 inhabitants. The number was likely far larger. Enslaved persons were considered taxable chattel that owners had an incentive to keep hidden from census takers. With the influx of newly arrived enslaved blacks and enslaved sailors coming and going in the busy harbor, the highly fluid black population was without doubt far larger than the official tally. 1
Even when not encumbered by being enslaved, nominally “free” blacks were constrained by curfews, limited to the jobs they were allowed to take, and subject to a separate set of laws that kept them in hand-to-mouth subsistence. Civic authorities monitored closely their activities for any behavior that strayed too far from arbitrary norms that applied only to them. 3
Poverty and War
Gary Nash of the University of California, Los Angeles, noted that the economy of Boston in the mid-eighteenth century was stagnant. 4 It was losing ground as a port to New York and Philadelphia, cities that served more productive agricultural hinterlands and were nearer to terminuses in the West Indies and the southern American colonies.
Fired by British imperialist ambitions in the New World, the colonial wars in of the 18th century (Queen Anne’s War, 1701-1713; War of Jenkins’s Ear, 1739-1748; King George’s War, 1744-1748; French and Indian War, 1754-1763) robbed New Englanders through war taxes and inflationary policies as the British treasury tried to finance the costly conflicts. Boston scrip steadily lost value. Taking data from tax rolls, Nash estimated that roughly one of every four Bostonians no longer were expected to pay taxes because they lived below subsistence levels. 4
Bostonians were pressed into service in conflicts as far away as the Caribbean and French Canada. Only one-tenth of the original group of 500 Massachusetts volunteers survived the Cartegena expedition (1740-1741), most succumbing to “yellow fever, dysentery, and outright starvation. 5 ” Of the 3500 volunteers serving in the Siege of Louisbourg (1758), only 150 died from actual fighting. Half of the total garrison died of dysentery during the campaign. Nash estimated that 8% of the colony’s men aged over 18 years died in the colonial wars of the mid-eighteenth century. With the loss of at least 400 men, Boston was full of war widows. A 1764 census counted 2941 men and 3612 women aged sixteen and over, an indication how war imbalanced the population of the town.
Another blow to town commerce came in March 1760 when a great fire swept the town, every fifth residence suffering some degree of loss. Of the 377 households that received aid in the aftermath of the disaster, 58% were classified as poor, and 30% were widows. By the mid-1760s, poverty in the city was appalling. 4
Inoculation in Colonial Boston
Inoculation in colonial Boston was introduced by a black man named Onesimus, who was enslaved to Cotton Mather (1663-1728), the firebrand Puritan minister who embodied the religious fervor in the colony. Onesimus verified that he had undergone the procedure in Africa while awaiting transport to New England. When an outbreak occurred in the holding pens that confined enslaved blacks before they were shipped to the New World, pus was collected from the sores of the first victims to inoculate the rest, preserving the slavers’ grim investment. 5
At Mather’s insistence Zabdiel Boylston, alone among the 14 physicians in Boston in 1721, began to inoculate as many of the citizenry as possible. The procedure itself worked: just 6 died (2.1%) of the 287 that were inoculated, just over 2% of the town’s 11,000 residents (2.6%). An incredible 5759 became infected the “natural” way, more than half the town, of whom 842 died (14.6%). 6
Smallpox returned to Boston in late 1729, just 7 years later. With the success of Boylston’s inoculations still fresh in the mind of the public, many took it upon themselves to undergo the procedure. Acceptance of inoculation had increased to where 10% of cases during the 1729-1730 epidemic came from the procedure, a modest increase given the hard experience of 2 outbreaks coming in quick succession. 5
In January 1752, another outbreak started with when the townspeople of Chelsea rescued the crew of a British merchant ship that ran aground in Nahant Bay. By March 23, town selectmen announced that “there were so many cases they feared no method can be taken to prevent the spreading of that Distemper. 5 ”
“This was the signal,” wrote John Blake of the National Library of Medicine. “Immediately inoculation started, and it proved far more popular than in 1730. 5 ” With the spring months, the numbers of deaths reached its peak: April, 119; May, 205; then June, 203. Then in July, there were only 31 deaths and by mid-August, the epidemic was over. “The reason for the decline is obvious,” Blake wrote. “There were hardly any susceptible people left. 5 ”
In the terms of modern epidemiology, Boston, boosted by inoculation, had reached herd immunity. Of Boston’s 7669 cases of smallpox, 2124 came through inoculation, about 28% of the total.
The rate was likely the highwater mark given the overall poverty of the Boston’s inhabitants. While many raced to get inoculated ahead of the contagion, the working classes were too busy eking out a living to deliberately undergo a procedure that brought the certainty of even a mild form of an illness that still carried a risk of death. 5
Inoculation had become complicated and costly. The fee for the procedure was two to three pounds (one pound roughly equivalent to £194 today). Patients were confined outside city limits in inpatient inoculation hospitals, where they underwent rigorous dietary regimens and pretreatment with mercury and antimony before they were inoculated. One inoculation hospital in Marblehead charged the princely sum of five pounds, fifteen shillings. 7 Another facility in Chelsea charged a daily fee of one pound, five shillings, and four pence for medicines and professional attendance. 5
The disease reemerged in early 1764. By March with the contagion nearly out of control, the town voted to treat the poor free of charge. The demand was so great that on March 13 the Selectmen voted to offer inoculation to all regardless of the city of residence. By the end of the outbreak, the Overseers of the Poor sponsored 1025 inoculations, another 400 came from outlying towns and neighboring colonies. Blake noted that in effect, the entire city had become “one great hospital. 5 ”
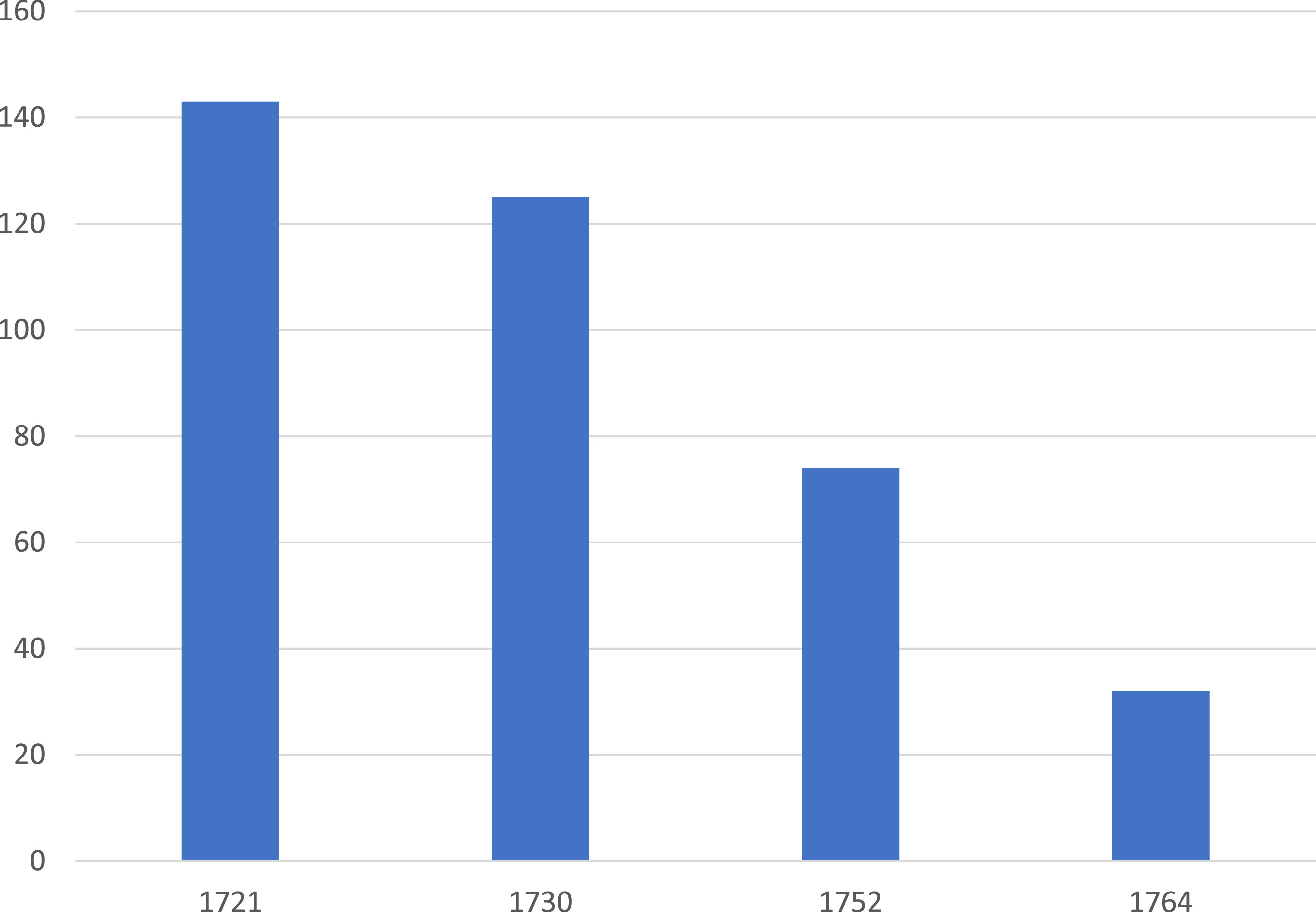
Offering inoculations to the poor had the desired effect. In the 1764 outbreak, 87% of the vulnerable population had undergone the procedure. Overall mortality from smallpox in Boston was just 3.2%, a level that directly correlated with the prevalence of inoculation (Figure 1). “For the first time, a smallpox year failed to stand out as one of unusual mortality,” Blake wrote. “One of the major reasons for this change was that for the first time, arrangements had been made for inoculating the poor.
5
” Deaths per 1000 cases, smallpox epidemics in Boston, MA, in 1721, 1730, 1752, and 1764. Data from Blake, 1953.
7
Benjamin Franklin
During the 1752 epidemic, Franklin (1706-1790; Figure 2) saw that the expense of inoculations prevented the working classes from having the benefit from the procedure. “The expense of having the operation performed by a surgeon weighs with others, for that has been pretty high in some parts of America,” Franklin wrote. “When a common tradesman or artificer has a number in his family to have the distemper, it amounts to more money than he can well spare.
5
” Antoine Maurin, artist. Benjamin Franklin. Public domain.
Franklin published a simple step-wise procedure that was written so that anyone could follow its instructions. He foresaw parents inoculating their own children. “It would be better to have inoculation performed by anybody, or by any matter,” he wrote, “than to suffer this disease to come on in the common way . . .. 8 ”
His source was “a nameless physician” who was motivated by “a disinterested benevolence. 8 ” While Franklin was not a physician, he famously published under a pseudonym throughout his career in publishing. During the 1721 outbreak, he posed as “Silence Dogood,” a pious but highly opinionated widow during his days as a teenaged apprentice to his brother James, who founded one of the publications in the newspaper war over inoculation. 9 And school children know he was Richard Saunders, the author of Franklin’s popular “Poor Richard” yearly almanacs of 1732-1758.
Still unanswered is why Franklin reported the outcome of inoculation for blacks (Figure 3). He perhaps wanted to show the blacks, no doubt inoculated with less involved procedures to the ones available to wealthy whites, responded to inoculation with the same lower mortality rates as whites. In doing so, he was the first to document disparate impact of disease and its treatment by race. Table from Franklin, 1759
8
Public domain.
What Franklin’s data also shows is that the prevalence of inoculation among blacks was only slightly below their estimated overall proportion of the population of the town. Blacks comprised 8.5% (693 of 8201) of all contracting the disease, which can be assumed to approximate their proportion of the general population. 8
The percent of blacks among those inoculated was lower at 6.8% (146 of 2143). That relatively fewer blacks were inoculated is not surprising; what is unexpected is the prevalence of inoculation was that high. The level reflects an uncomfortable and underrecognized feature of colonial New England: the widespread ownership of enslaved persons up to the time of Declaration of Independence. Enslaved blacks were integral to the Boston economy. Whites who owned their labor could not do without them and made certain that they were protected to the same extent as themselves and their families.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.