
Abstract
Background
Failure to rescue (FTR) patients with postoperative complications contribute to a significant proportion of postoperative mortality. Our main objective was to determine the risk factors for FTR among patients undergoing pancreaticoduodenectomy who suffered a life-threatening complication requiring intensive care unit (ICU) management.
Materials and Methods
Consecutive patients undergoing pancreaticoduodenectomy from 2011 to 2020 were reviewed retrospectively. Causes of organ failure were described as the one that most commonly contributed to patient’s transfer to ICU or death. Two groups were created based on whether patients had FTR and risk factors for FTR were compared. The impact of baseline characteristics, operative characteristics, and risk scoring on FTR was analyzed using multiple logistic regression.
Results
There were 19/58 (33%) FTR patients. Baseline, operative characteristics, postoperative complications, and length of hospital and ICU stay were similar between groups. However, a higher proportion of FTR patients experienced a postoperative pancreatic fistula (POPF) (16% vs 2.6%, P = .062). Among patients who experienced a POPF, the FTR group had a trend in delayed time from diagnosis to treatment (7 vs 23 hours, P=.131). Renal complications (OR 6.12, 95% CI, 1.23 to 38.43, P = .035) and time from POPF diagnosis to treatment (OR 1.05, 95% CI, 1.00 to 1.11, P = .036) were independent predictors of FTR by multivariable analysis.
Conclusion
The occurrence of certain postoperative complications such as renal complications as well as delayed timing of the management of POPF is predictive of FTR following pancreaticoduodenectomy, especially as delayed timing to treatment is a risk factor for FTR.
Key Takeaways
Renal complications and the time from postoperative pancreatic fistula (POPF) or intra-abdominal abscess diagnosis to treatment were independent predictors of failure to rescue (FTR). Risk scoring systems (Charlson comorbidity index and modified frailty index) were not significantly associated with FTR. Occurrence of certain postoperative complications (eg, renal complications) and delayed timing of the management of POPF are predictive of FTR following pancreaticoduodenectomy.
Introduction
Pancreaticoduodenectomies are complex technical operations that carry a high risk of postoperative complications (24-74%).1-4 These complications vary from local complications such as surgical site infection to systemic ones such as pulmonary complications.3-5 Over the past few decades, the proportion of patients who experience postoperative complications following pancreaticoduodenectomy has remained stable.3,4 Although the proportion of patients who die following surgery has decreased, postoperative mortality remains high (1-5%).6-8
Timely recognition and management of postoperative complications among patients undergoing pancreaticoduodenectomy is crucial to preventing postoperative mortality. 9 The term “failure to rescue (FTR)” has been coined to describe mortality among patients with major complications and is an emerging indicator of the quality of surgical care.10-12 Therefore, it is important to understand the factors responsible for FTR as their early identification may allow physicians to better predict and manage complications, ultimately preventing postoperative mortality. However, there are few studies about FTR patients in the context of pancreaticoduodenectomy.
Our main objective was to determine the risk factors for FTR among patients undergoing pancreaticoduodenectomy who suffered a life-threatening complication requiring intensive care unit (ICU) management (ie, Clavien-Dindo grade IV). 13 Secondary objectives were to detail the causes of organ failure and mortality among these patients.
Materials and Methods
Patient Cohort
A retrospective cohort of consecutive, adult patients undergoing pancreaticoduodenectomy for any indication at a single high-volume academic hepatobiliary center from April 1, 2011, to May 30, 2020, were included in this study. Among those, we identified patients who met the following inclusion criteria: transfer to ICU because of organ failure (CDC grade IV); continuous postoperative ICU care for three or more days and any organ failure (CDC grade IV); or 90-day and in-hospital mortality (CDC grade V). Cancer patients who underwent combined organ resection (eg, cholecystectomy and colon resection) were also included. Patients who underwent procedures combined with other surgical techniques (eg, abdominal aorta aneurysm operation) or palliative procedures without pancreaticoduodenectomy (eg, exploratory laparotomy) were excluded. We used a database for hepatopancreatobiliary patients that was collected prospectively (eg, baseline characteristics, operative details, and postoperative complications). Other variables were collected retrospectively (eg, timing to treatment and risk scoring). Institutional ethics approval was obtained prior to initiating this study. Two reviewers read all medical records and came to a consensus on the cause of organ failure and death if applicable for each patient.
Patient characteristics, comorbidities such as vascular insufficiency which was defined as “inadequate blood flow to fulfill the metabolic needs of organs such as brain (ie, carotid artery) or peripheral arteries of the lower extremities organ,” 14 operative details, pathological results, laboratory results, ICU data, and postoperative complications within 90 days were collected retrospectively from electronic medical records. Surgeons followed pancreas fistula risk scoring to determine whether surgical drains should be placed (ie, patients with softer glands and smaller ducts had drains placed, whereas patients with harder pancreas and larger ducts did not). 15 Two drains were placed if applicable, one anterior and one posterior to the pancreatic anastomosis. All patients received 100 μg of octreotide subcutaneously 1 hour before surgery and 3 times a day after surgery for 7 days or until discharge if discharge happened before 7 days. Each complication was deemed as either local or systemic. Certain characteristics such as pancreatic duct size (ie, <3 mm, 3-6 mm, and >6 mm) and texture (ie, soft, intermediate, and hard) were prospectively collected from case report forms starting in 2016. Preoperative comorbidity data was collected and graded using the Charlson comorbidity index and a validated modified frailty index (mFI). 16
Causes of Organ Failure and Mortality
The causes of organ failure and mortality were determined according to previously published classification. 17 This classification describes a “seminal or critical” complication, as the one that most commonly contributed to a patient’s transfer to ICU or to their death. This critical complication was defined as the cause of organ failure and thus eventual death. Patients were grouped based on the causes of organ failure and mortality into five categories: renal failure (acute renal failure); pulmonary failure (pneumonia, prolonged ventilator assistance, and pulmonary edema); cerebrovascular complication (stroke); cardiac complication (myocardial infarction, congestive heart failure, and arrhythmia); and surgical site complication (hemorrhage, surgical site infection, postoperative pancreatic fistula (POPF), and intra-abdominal abscess). For this last category, we also evaluated the time from identification to the time of management of the complication as an important variable for those patients diagnosed with an intra-abdominal collection (ie, abscess). Following the International Study Group of Pancreatic Fistula definition of pancreatic leakage, a POPF was considered to be any “fluid output of any measurable volume via an operatively placed drain with amylase activity greater than 3 times the upper normal serum value.” 18 An infected (ie, signs of sepsis) POPF or fluid collection was classified as an intra-abdominal abscess. Postoperative pancreatic fistula or abscess was diagnosed using CT imaging in all patients. Treatment for POPF or abscess was defined as the use of antibiotics along with percutaneous drainage or reoperation. Major intra-abdominal bleeding was defined following the International Society of Thrombosis and Hemostasis for bleeding in surgical trials, as “fatal bleeding or bleeding that requires a second intervention (open or endovascular), or that causes hemodynamic instability as assessed by the surgeon.” 19 Major bleeding should be associated with a fall in hemoglobin level of > 2 g/dL or transfusion of > 2 units of packed red blood cells. Treatment for bleeding was defined as blood transfusion along with the use of angiography or reoperation.
Statistical Analysis
Baseline characteristics were presented using median (range) and counts (percentage) depending on the variable type and distribution. Normally distributed continuous variables were compared with the t-test, whereas non-normally distributed continuous variables were compared with the Mann-Whitney U test. Proportions were compared using the chi-square test. Univariable analysis was performed to calculate the association of each factor with FTR. The risk factors for FTR identified in the univariable analysis were included in the multivariable logistic regression analysis in a stepwise fashion and expressed using adjusted odds ratios (OR) with 95% confidence interval (CI). Factors associated with FTR were further explored in a qualitative manner via patient chart review to identify potential causes of “delayed escalation,” including failure to recognize, communicate, and/or management of patients upon deterioration. All tests were two-sided and conducted at a significance level of 5% using R 3.6.2 (The R Foundation, Vienna, Austria). Missing data were assumed to be missing at random. This work was performed according to the Declaration of Helsinki (Research Registry: researchregistry6870) and STROCSS criteria. 20
Results
Baseline Patient Characteristics
Baseline Characteristics and Comorbidities.
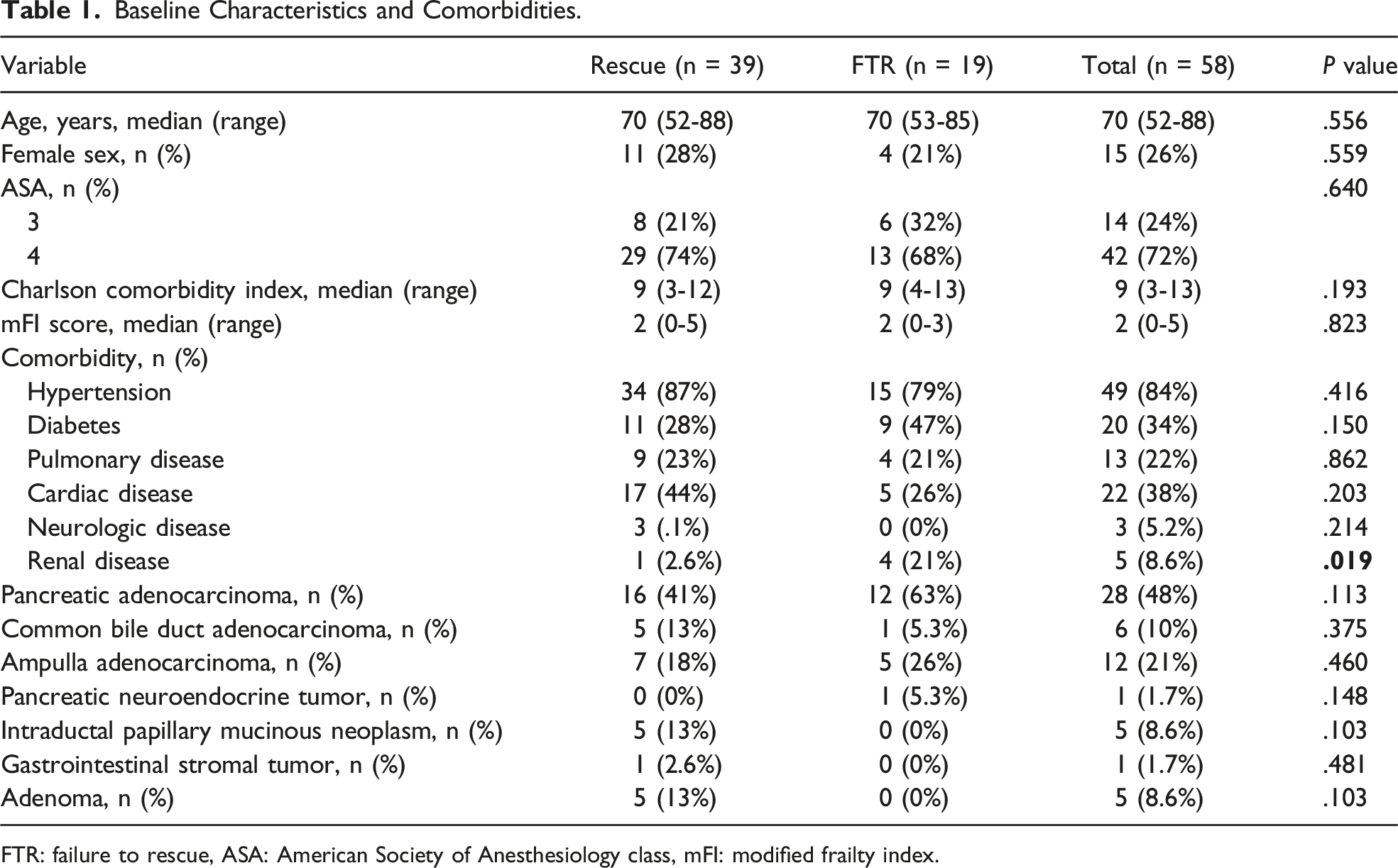
FTR: failure to rescue, ASA: American Society of Anesthesiology class, mFI: modified frailty index.
Operative Characteristics
Operative Characteristics.
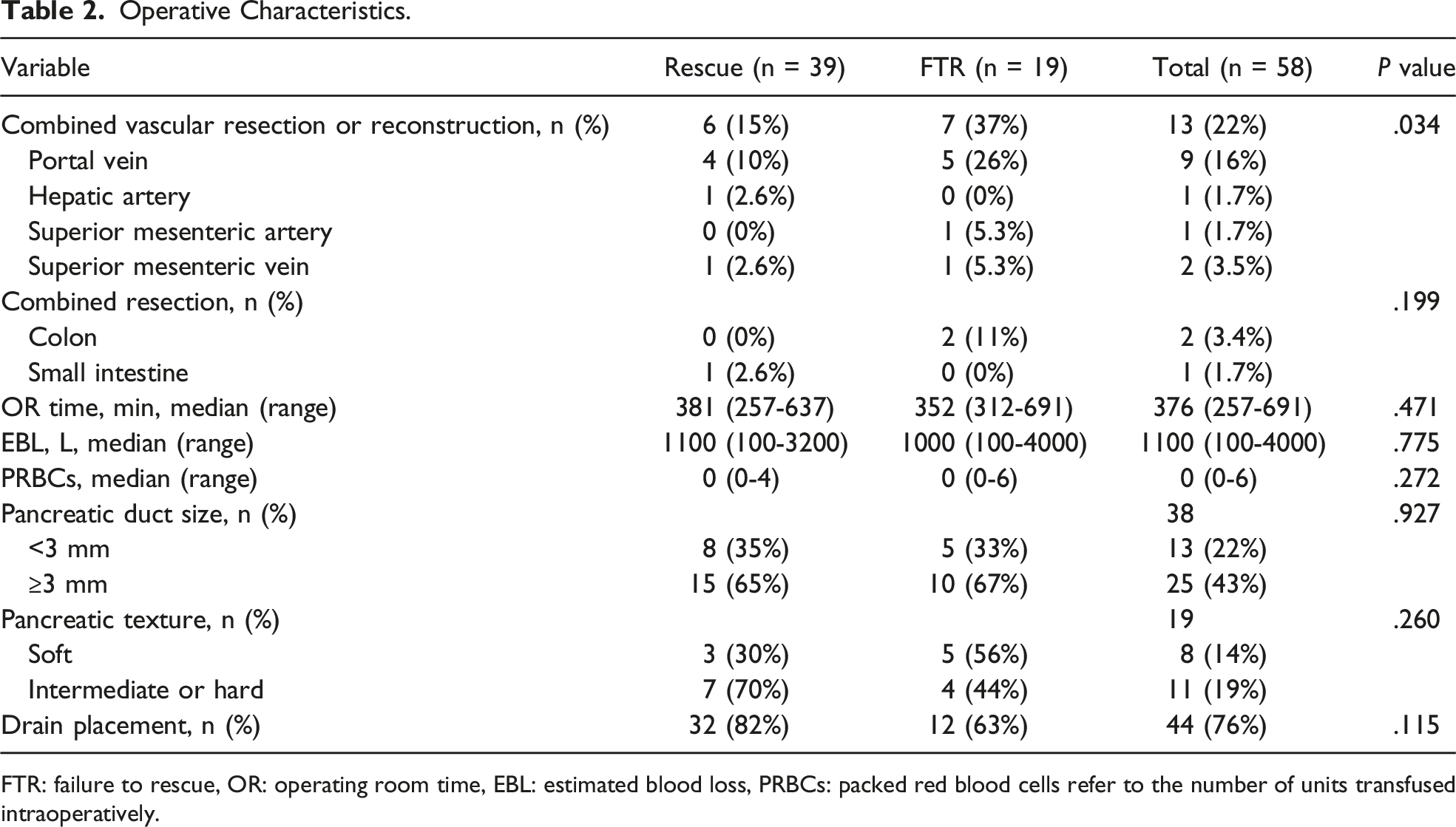
FTR: failure to rescue, OR: operating room time, EBL: estimated blood loss, PRBCs: packed red blood cells refer to the number of units transfused intraoperatively.
Postoperative Complications and Length of Hospital Stay
Postoperative Complications and Length of Hospital Stay.
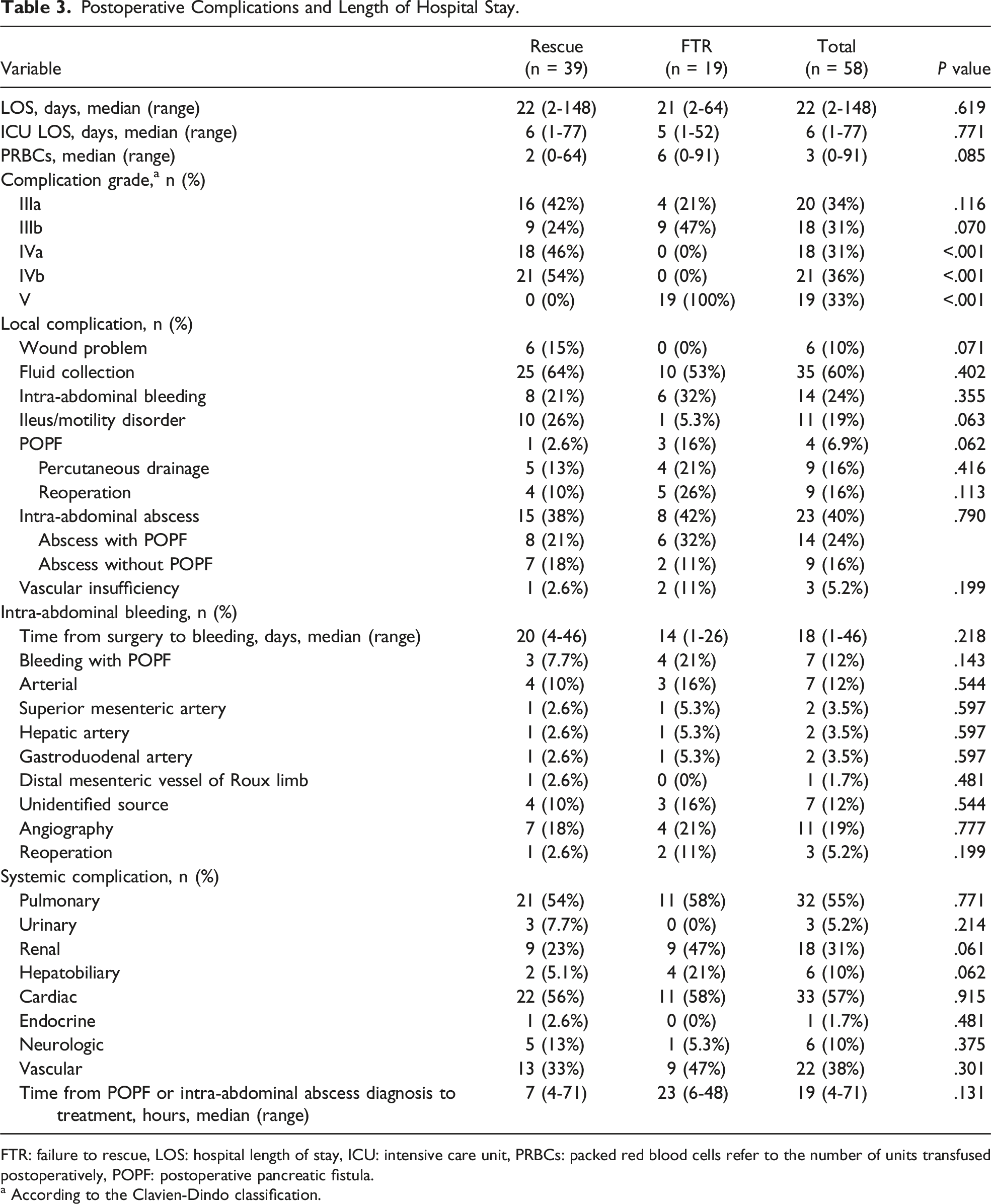
FTR: failure to rescue, LOS: hospital length of stay, ICU: intensive care unit, PRBCs: packed red blood cells refer to the number of units transfused postoperatively, POPF: postoperative pancreatic fistula.
a According to the Clavien-Dindo classification.
Plotting the FTR rate based on complication type, patients who experienced a POPF had the highest mortality rate (75%, 3/4), followed by patients who experienced a renal complication (50%, 9/18) (Figure 1). Mortality rate according to complication type.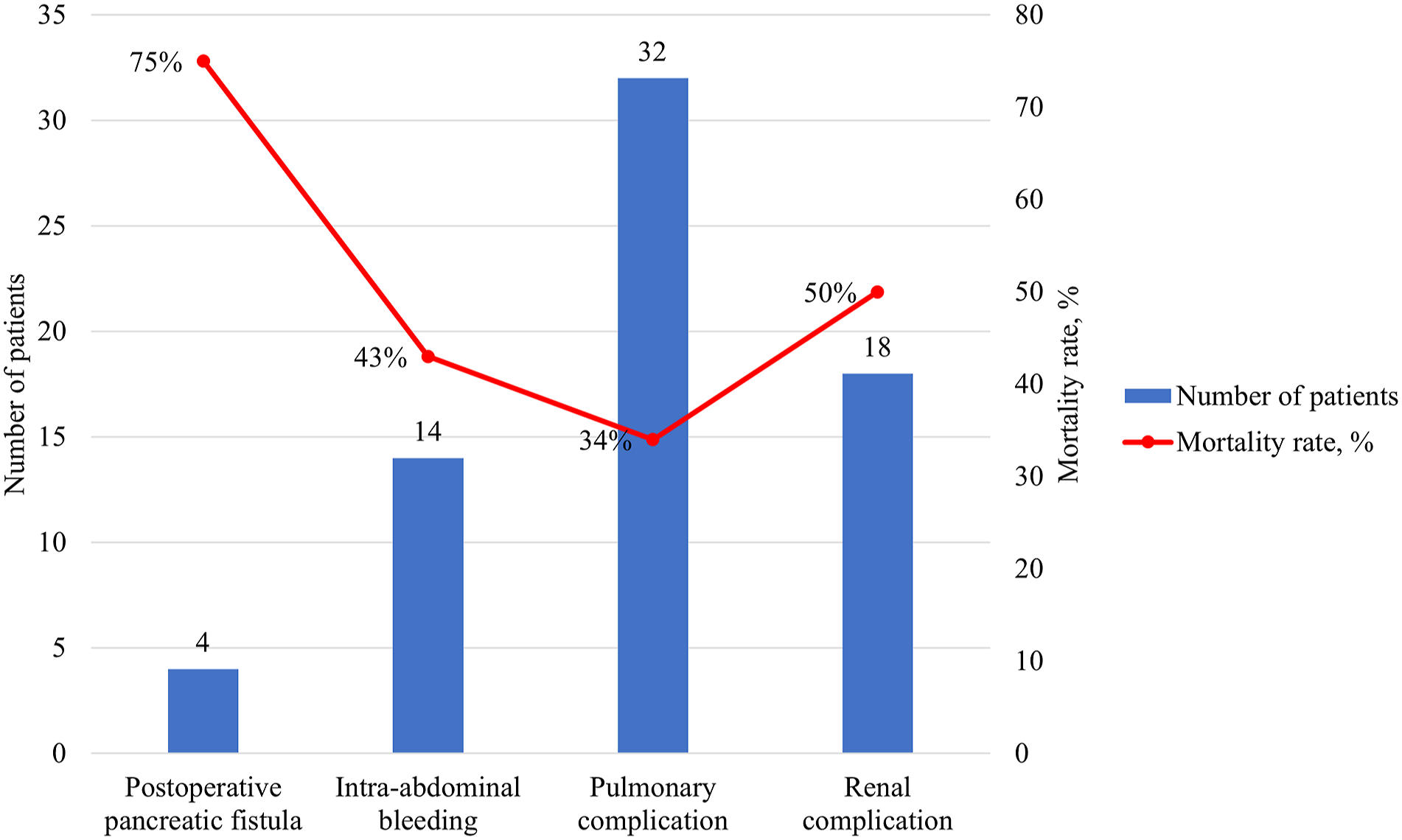
Causes of Organ Failure
The most common cause of organ failure among all patients was sepsis from an intra-abdominal abscess (21%, 12/58). This was followed closely by patients who experienced organ failure secondary to pulmonary insufficiency requiring prolonged ventilator assistance (17%, 10/58), myocardial infarction (16%, 9/58), or pneumonia (14%, 8/58). The proportions of patients with other causes of organ failure were relatively lower (Supplementary Table 1).
Failure to Rescue
Multivariable Analysis of Factors Associated With Failure to Rescue.
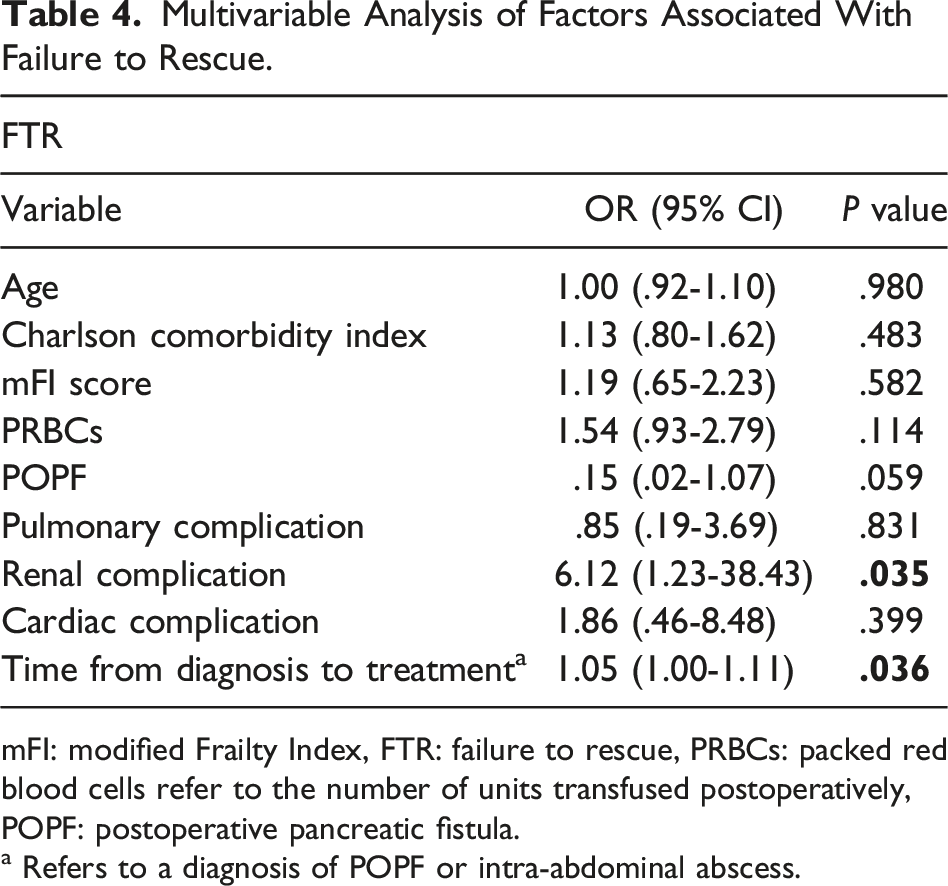
mFI: modified Frailty Index, FTR: failure to rescue, PRBCs: packed red blood cells refer to the number of units transfused postoperatively, POPF: postoperative pancreatic fistula.
a Refers to a diagnosis of POPF or intra-abdominal abscess.
Discussion
We divided a cohort of patients undergoing pancreaticoduodenectomy who experienced a significant organ failure leading to ICU admission into two groups, those that survived and those that died (ie, those that we failed to rescue or FTR patients). The baseline characteristics of these patients were similar, except for a slightly higher proportion of patients with previous history of renal disease in the FTR group as well as a higher proportion of patients undergoing pancreaticoduodenectomy combined with major vascular resection in the FTR group. Postoperatively, we noticed that patients in the FTR group had a higher rate of POPF, leading to a higher proportion of postoperative complications requiring reoperation (Clavien-Dindo Class IIIb). Due to the retrospective nature of this study, we were unable to determine the factors that led the surgeon to reoperate as opposed to treat an intervention not requiring general anesthesia. We can presume that the decision was made after careful review of the physical and radiological findings, including hemodynamic instability and nature of the problem (ie, bleeding vs abscess). However, it is important to note that the FTR group had a higher proportion of patients undergoing reoperation than the rescued group and that the use of reoperation instead of interventional radiology procedures could have increased their risk of death. The most common cause of organ failure among all patients was sepsis from an intra-abdominal abscess. Patients who experienced a POPF had the highest mortality rate followed by patients who experienced renal failure. Most importantly, we found that the presence of renal complications leading to renal failure and a delayed time from diagnosis of a POPF or an abscess to treatment was associated with FTR. Based on our findings, we have changed the way patients with septic complications are managed by following our “surviving sepsis campaign,” which favors the administration of intravenous antibiotics within 1 hour in patients with sepsis and within 3 hours in patients suspected of having sepsis.21,22 Also, the first dose of the antibiotic is not renal adjusted.
This study suggests that certain postoperative complications as well as the management of the timing of those complications are independent predictors of FTR following pancreaticoduodenectomy. These findings are generally consistent with the results of prior studies, which have investigated the causes of organ failure and mortality in surgical patients.23-25 They confirm that baseline patient characteristics are not routinely associated with FTR, rather postoperative factors such as “delayed escalation” (ie, delayed time from diagnosis to treatment of the complication) are more important. 26 We did not find issues with “recognition” or “communication” of deterioration, but rather we identified problems with management of deterioration, which were mostly due to initial patient stability that did not trigger a high “early warning score,” leading to delayed treatment. Other known factors associated with FTR, such as hospital volume, nurse staffing levels, and ICU admissions, were not relevant to our study as all cases reported here were performed at a high-volume hepatobiliary center with excellent nursing staff and 24-hour access to interventional radiology, operating rooms, surgeons, and ICU physicians on call.
This study has some limitations. As a retrospective study, it is unknown whether patients were transferred to the ICU due to an expected higher rate of postoperative complications among high-risk patients or due to the complications themselves. For example, it is possible that patients with baseline history of renal failure were transferred earlier to the ICU (as a preventative measure), therefore escalating their care sooner than patients without history of renal failure. Also, the small sample size and consequently relatively small number of patients in the FTR group makes it difficult to quantify issues associated with delayed management. Lastly, it is possible that continued quality improvement initiatives within the hospital system may have altered our results (ie, the initiation of an “early warning score” system in 2014 or a higher nurse to patient ratio of one nurse for three patients implemented in 2012). This study has certain advantages that make it unique; to our knowledge, this is the first single institution series on patients undergoing pancreaticoduodenectomy to address factors associated with FTR, including the identification of organ failure and mortality. We also performed a thorough review of the patients’ electronic medical records to identify factors associated with “delayed escalation” leading to FTR.
Conclusion
In conclusion, the occurrence of certain postoperative complications and “delayed escalation” are predictive of patients at risk of FTR following pancreaticoduodenectomy. Early identification of POPF via radiological imaging and early implementation of treatment (ie, antibiotic therapy, interventional radiology drainage, or surgery) may lead to lower postoperative mortality associated with FTR. This can assist clinicians in the decision-making process during the postoperative management of these patients.
Footnotes
Author Contributions
All authors provided substantial contributions to the conception and design of the work, drafting the work, and revising it critically for important intellectual content and gave final approval of the version to be published. The authors agree to be accountable for all aspects of the work.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
The study protocol was reviewed and approved by the Hamilton Integrated Research Ethics Board (11107-C).
Supplemental Material
Supplemental material for this article is available online.