
Abstract
Background
COVID-19 is a deadly multisystemic disease, and bowel ischemia, the most consequential gastrointestinal manifestation, remains poorly described. Our goal is to describe our institution’s surgical experience with management of bowel ischemia due to COVID-19 infection over a one-year period.
Methods
All patients admitted to our institution between March 2020 and March 2021 for treatment of COVID-19 infection and who underwent exploratory laparotomy with intra-operative confirmation of bowel ischemia were included. Data from the medical records were analyzed.
Results
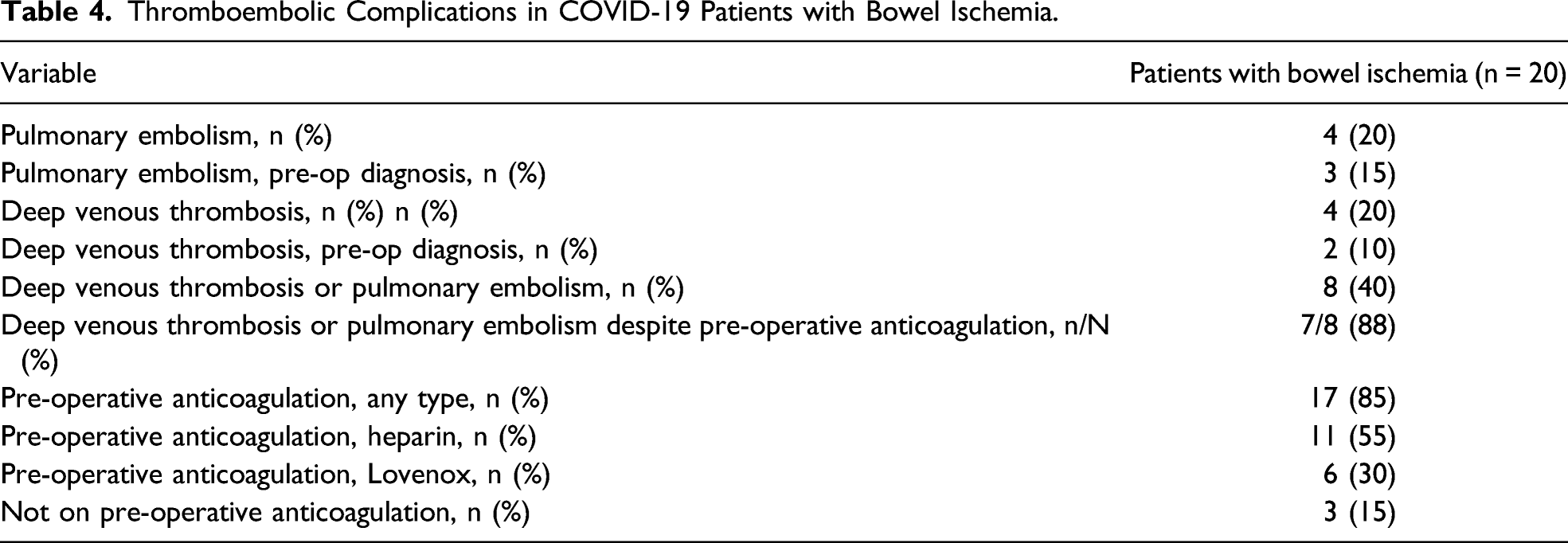
Twenty patients were included. Eighty percent had a new or increasing vasopressor requirement, 70% had abdominal distension, and 50% had increased gastric residuals. Intra-operatively, ischemia affected the large bowel in 80% of cases, the small bowel in 60%, and both in 40%. Sixty five percent had an initial damage control laparotomy. Most of the resected bowel specimens had a characteristic appearance at the time of surgery, with a yellow discoloration, small areas of antimesenteric necrosis, and very sharp borders. Histologically, the bowel specimens frequently have fibrin thrombi in the small submucosal and mucosal blood vessels in areas of mucosal necrosis. Overall mortality in this cohort was 33%. Forty percent of patients had a thromboembolic complication overall with 88% of these developing a thromboembolic phenomenon despite being on prophylactic pre-operative anticoagulation.
Conclusion
Bowel ischemia is a potentially lethal complication of COVID-19 infection with typical gross and histologic characteristics. Suspicious clinical features that should trigger surgical evaluation include a new or increasing vasopressor requirement, abdominal distension, and intolerance of gastric feeds.
Key Take-Aways
• Bowel ischemia is a potentially lethal complication of COVID-19 infection. • COVID-19-induced intestinal ischemia has typical gross and histologic characteristics. • Suspicious clinical features that should trigger surgical evaluation include: - new or increasing vasopressor requirement, - abdominal distension, and - intolerance of gastric feeds.
Introduction
COVID-19 is a multisystemic disease 1 and the gastrointestinal tract is highly susceptible to infection with the virus 2 since the ACE2 receptor through which the SARS-CoV-2 enters cells is highly expressed in the duodenum, jejunum, ileum, cecum, and the colon. 3 In fact, viral ribonucleic acid (RNA) was detected in stool samples from 48% of COVID-19 positive patients, with RNA detection in stool samples from patients whose respiratory tests were no longer positive. 4 In addition, SARS-CoV-2 RNA has been detected in the gastrointestinal tract. 5
The incidence of gastrointestinal symptoms in COVID-19 infection is as high as 61%. 5 In one study, 45% of patients had gastrointestinal symptoms on admission. 6 Although we previously reported acute intestinal ischemia in COVID-19 infection,6,7 the condition remains poorly described. 8 Furthermore, there appears to be failure to distinguish bowel ischemia due to acute mesenteric thromboembolism from bowel ischemia that is due to COVID-19 infection.8-10
In this report, we describe our institution’s surgical experience with management of bowel ischemia due to COVID-19 infection over a one-year period.
Methods
The study was approved by our institutional review board. All patients included were admitted to the Massachusetts General Hospital between March 2020 and March 2021 for treatment of COVID-19 infection and developed clinical features suggestive of an acute abdominal pathology. Our Acute Care Surgery team was consulted out of concern for bowel ischemia. When the clinical, laboratory, and radiologic features were suspicious for bowel ischemia, the patients were taken emergently to the operating room for an exploratory laparotomy. Only those who had intra-operatively confirmed bowel ischemia were included in the subsequent analysis. Their medical records were reviewed, and the following data were abstracted: demographics, clinical characteristics, laboratory values, imaging results, intra-operative findings and surgical managements, pathology reports, mortality data, and thromboembolic complications. Statistical analysis was performed using SPSS Statistics version 25. Continuous variables were described using summary statistics while percentages were used to describe categorical variables.
Results
Demographics
Demographic and Clinical Characteristics.
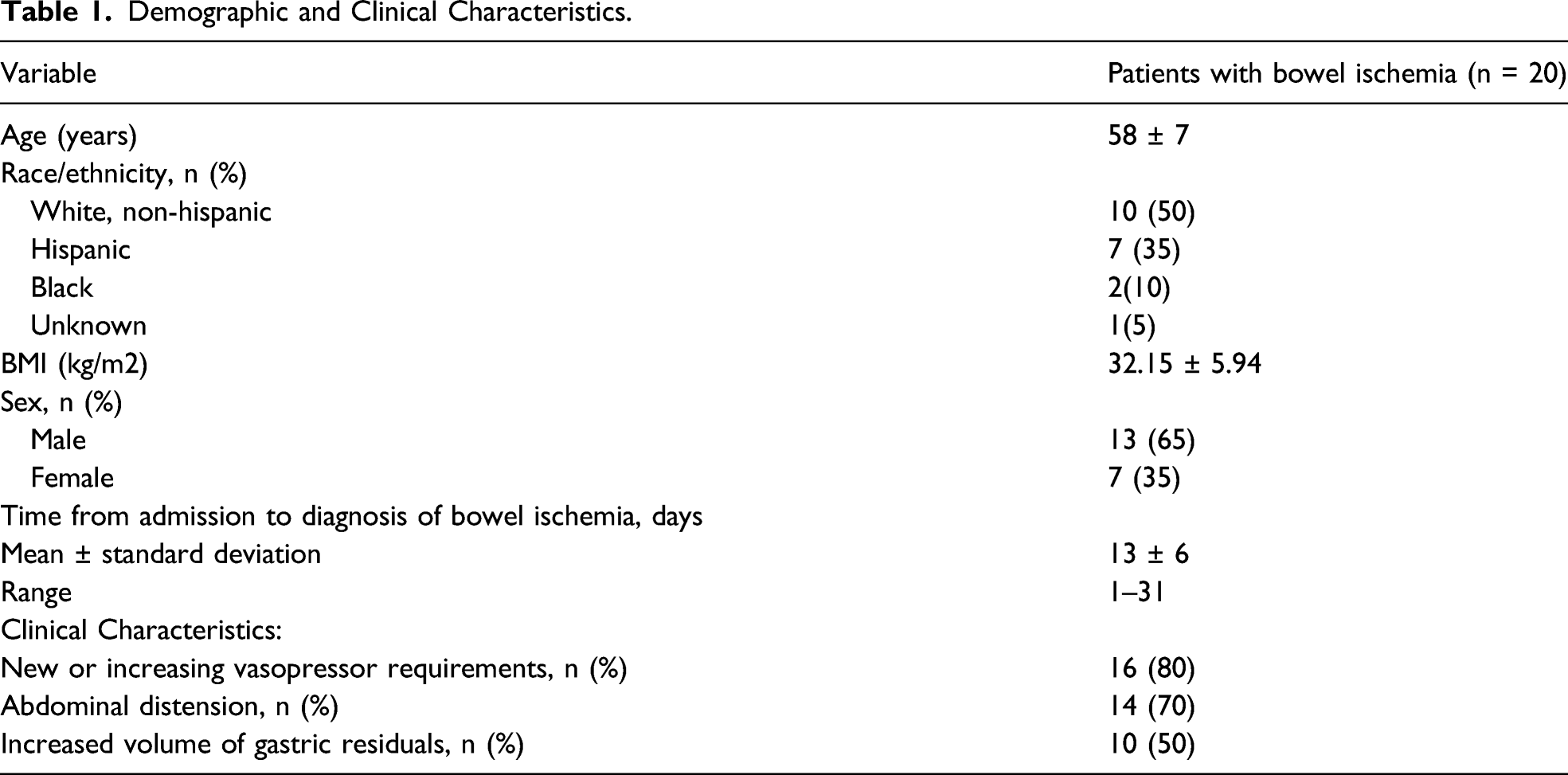
Clinical Characteristics
The average duration between admission for COVID-19 infection and diagnosis of bowel ischemia was 13 days. At the time of diagnosis of ischemic bowel, 45% of patients had documented improvement in their respiratory status. Three clinical features triggered a surgical consult: increase in vasopressor requirements, abdominal distension, and increase in gastric residuals. The proportion of patients with these findings is summarized in Table 1.
Laboratory Findings
On the day of diagnosis, 84% of patients had leukocytosis, and 5% of patients were leukopenic, with only 11% having a normal WBC count. The WBC count doubled in 26% of patients within 24 hours prior to diagnosis. In 90% of patients, there was increased leukocytosis within the 48-hour period preceding diagnosis. The WBC count doubled within that time frame in 37% of patients. In 47% of patients, there was doubling of the WBC count within the 72-hour period preceding diagnosis. Of note, the median serum lactate level in this group was relatively low at 1.7 mmol/L. For patients in whom pre-operative D-dimer levels were obtained, the average level was 4479 ± 712 ng/mL (normal value: <500 ng/mL).
Imaging Results
Plain abdominal x-ray and/or CT abdomen and pelvis were performed in patients who could tolerate it. Of the 12 patients who had a pre-operative abdominal x-ray, pneumatosis intestinalis was detected in 42%, while portal venous gas was present in 33%. Of 12 patients who underwent a pre-operative abdominopelvic CT scan, pneumatosis was present in 83%, portal venous gas was found in 58%, and the major mesenteric vessels (celiac, superior mesenteric, and inferior mesenteric arteries) were patent in 92% (11 of 12). The one patient with unknown patency of the mesenteric vessels had a CT abdomen and pelvis without IV contrast.
Intra-Operative Findings
Most patients had intra-operative findings that shared distinct features. Most notably, the necrotic bowel had a distinct yellow color, rather than the typical purple or black color of ischemic bowel (Figure 1). There were often few large segments with extensive necrosis together with numerous, smaller areas of necrosis. In general, the large areas involved the entire circumference of the bowel, whereas the smaller areas of necrosis were often antimesenteric. The intervening bowel between the areas of necrosis was pink and well-vascularized, with sharp transition from necrotic to viable segment. The mesentery seemed well-vascularized during the surgical exploration, consistent with the radiologic impression of patent major mesenteric vessels (Table 2). In two patients, the clinical pattern was that of colonic pseudo-obstruction. The bowel from these patients did not show a bright yellow pattern but rather the typical dark purple color of ischemic bowel. Intra-operative appearance of small and large bowel in COVID-19-induced bowel ischemia. A. Full thickness necrosis with yellowish pigmentation affecting the jejunum and proximal ileum. Patient underwent segmental small bowel resection. B. Necrosis affecting both the small and large bowel. Patient underwent a right hemicolectomy and segmental small bowel resection. C. Necrosis involving the small bowel, with typical bright yellow pigmentation. Patient had a segmental bowel resection. D. Necrosis involving the terminal ileum, cecum, ascending colon and proximal transverse colon. E. Patchy yellowish necrosis involving the mid jejunum, with associated desmoplastic reaction. Location is antimesenteric. Intra-Operative Findings of Bowel Ischemia from COVID-19.

Surgical Management
Intra-operatively, ischemia affected the large bowel in 80% of cases, the small bowel in 60%, and both in 40%. Nineteen out of the 20 patients had either resection of the small bowel, large bowel, or both. In the one patient who was excluded from bowel resection, the extent of ischemia was so severe that additional procedures were deemed futile.
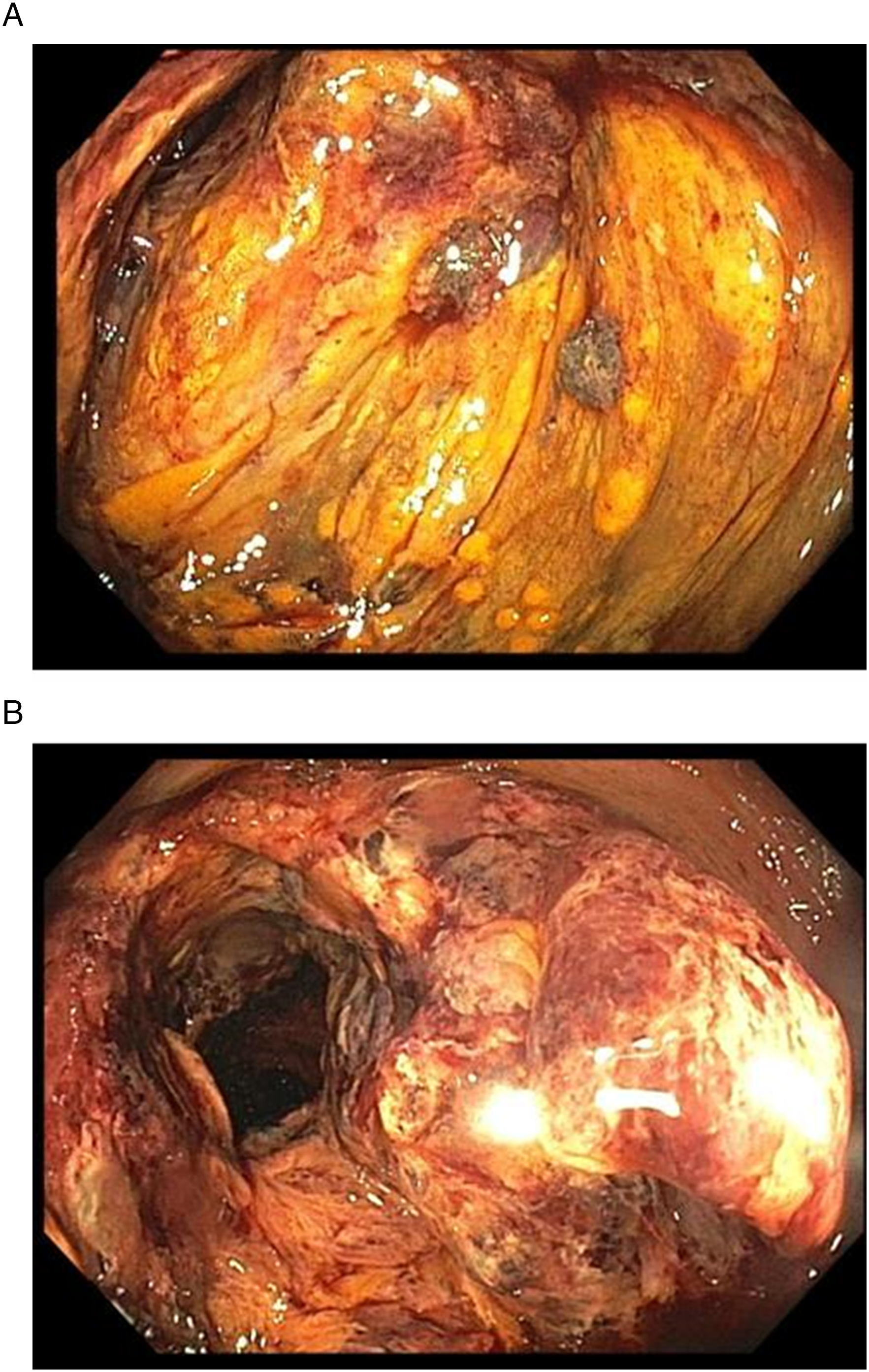
The majority of patients (85%) had a bowel resection during the initial exploratory laparotomy. In nearly two-thirds (65%), the abdomen was left open at the initial laparotomy. Of those who survived and came back for a second-look or subsequent laparotomy, 33% of them had bowel resection at this subsequent trip to the operating room. Notably, one patient had his first bowel resection at the third-look laparotomy as the colon looked questionable for ischemia during the first and second laparotomies. During the third-look laparotomy, intra-operative colonoscopy was performed, which showed clearly necrotic colonic mucosa (Figure 2), necessitating colonic resection. The appearance of the colonic mucosa on colonoscopy was similar to that performed pre-operatively in another patient who was on ECMO and developed lower gastrointestinal bleeding (Figure 3). The colonoscopy revealed the necrotic mucosa in the cecum as the source of the bleeding. Intra-operative colonoscopy. A. The mucosa of the transverse colon appears ischemic and ulcerated on intra-operative colonoscopy. The typical yellowish pigmentation of ischemic bowel is obvious. B. Mucosal necrosis extended to the descending colon, with a transition zone of healthy appearing bowel mucosa at the sigmoid colon-descending colon junction. Pre-operative colonoscopy. A, B. Necrotic colonic mucosa with typical yellowish pigmentation.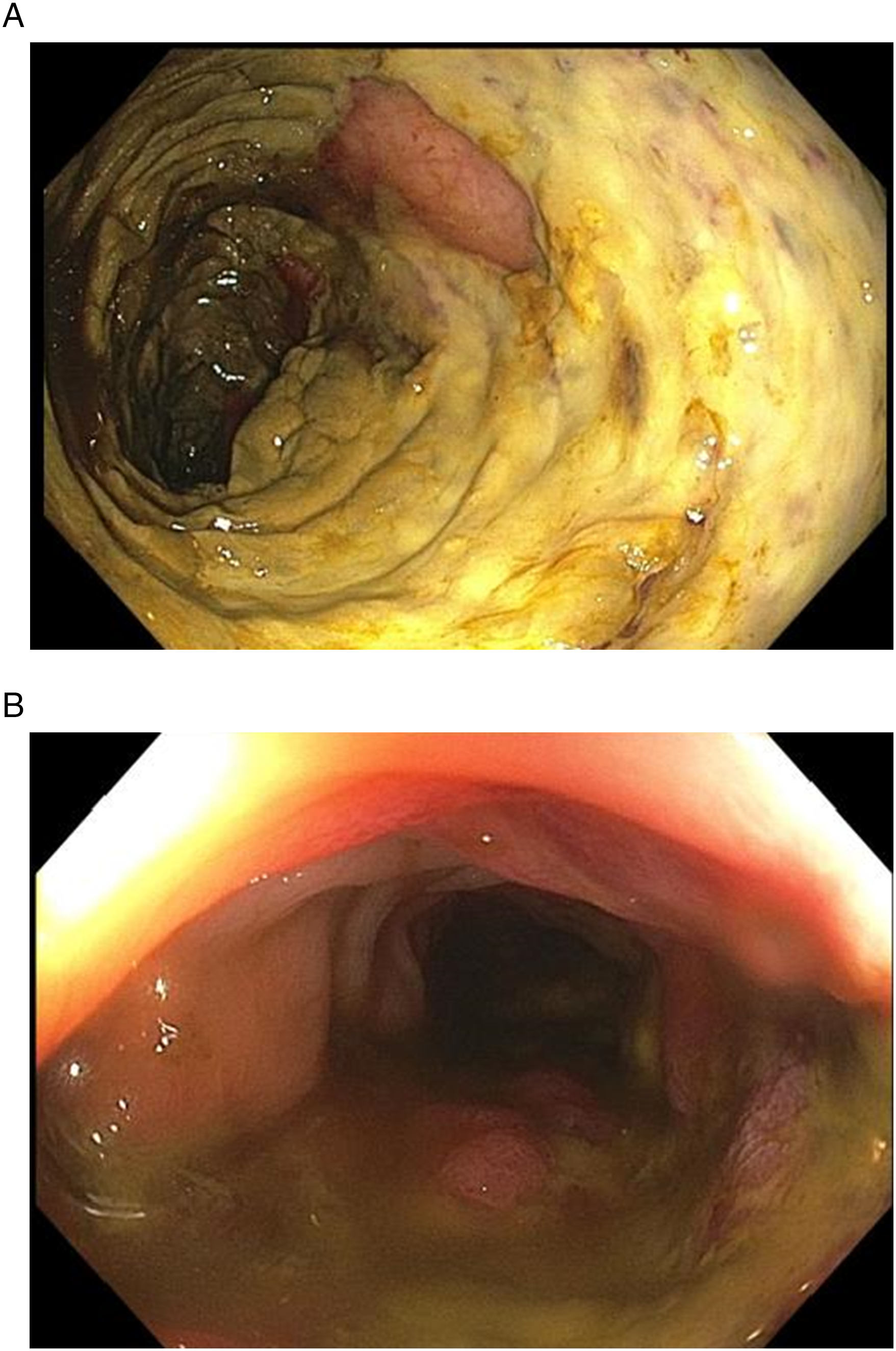
Surgical Management.
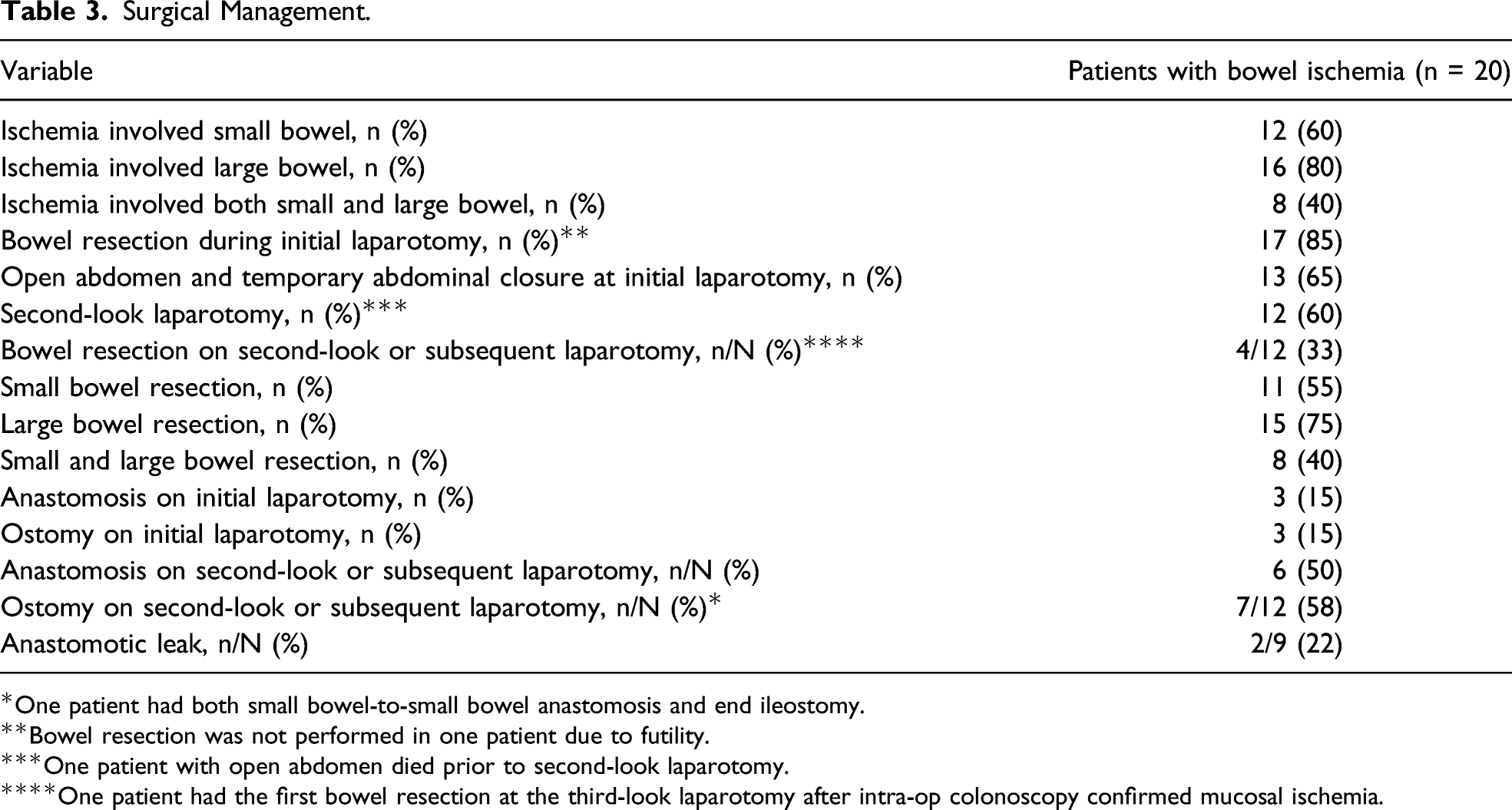
*One patient had both small bowel-to-small bowel anastomosis and end ileostomy.
**Bowel resection was not performed in one patient due to futility.
***One patient with open abdomen died prior to second-look laparotomy.
****One patient had the first bowel resection at the third-look laparotomy after intra-op colonoscopy confirmed mucosal ischemia.
Histology
A detailed pathologic description of these cases will be reported separately. Briefly, the histologic features were similar. The specimens showed mucosal necrosis, and mural or transmural necrosis in slightly more than half of the cases. Pneumatosis was identified pathologically in some of the cases (Figure 4(A)). In nearly all cases, the areas of mucosal necrosis showed fibrin thrombi in small vessels in the submucosa and lamina propria (Figure 4(B)). In some specimens, the bowel resections showed well-defined areas of mucosal necrosis juxtaposed to areas of viable mucosa with a relatively sharp transition point. This pattern mirrors the sharp demarcation between ischemic and normal bowel segments seen grossly in Figure 1. Three cases, including one presenting as pseudo-obstruction, lacked fibrin thrombi, but had fibrosis of the external layer of the muscularis propria with varying degrees of superimposed acute ischemic changes. Representative histologic appearance of COVID-19-associated bowel ischemia. A. Low power view of a colonic resection in COVID-19. The mucosa shows necrosis and hemorrhage. The submucosa is markedly edematous, with empty spaces representing pneumatosis intestinalis (arrowheads). Submucosal vessels show fibrin thrombi (arrow). 40x hematoxylin and eosin. B. Higher magnification of the same case shows fibrin thrombi in several small vessels (arrowheads). 200x hematoxylin & eosin.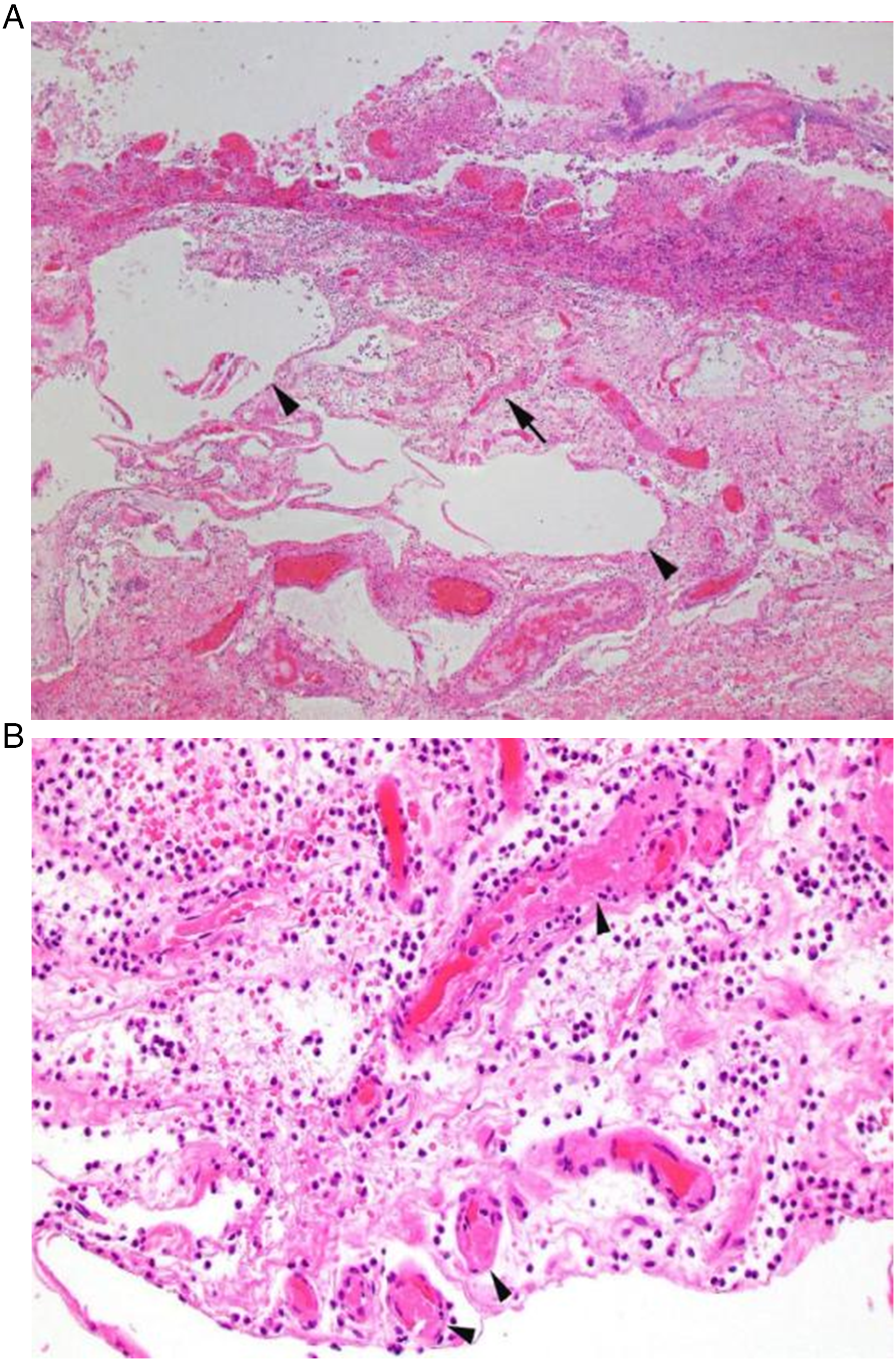
Outcomes: Mortality and Thromboembolic Complications
The overall mortality in this cohort was 50%. Patients <65 years of age had a mortality of 33%. Although patients aged ≥65 years constituted only 25% of the patients, this condition was highly lethal in this population, with a mortality of 100%.
Thromboembolic Complications in COVID-19 Patients with Bowel Ischemia.
Discussion
Acute bowel ischemia due to COVID-19 infection is a potentially lethal complication. In our study, the mortality in affected patients was 50%, with those over 65 years having a 100% mortality and patients less than 65 years having a mortality of 33%. This underscores the need for rapid diagnosis and prompt surgical management.
The three most consistent clinical variables in our patients with bowel ischemia were a new or increasing vasopressor requirements, significant abdominal distension, and increased gastric residual volume. These, along with concerning laboratory findings, triggered a surgical consultation. Increasing leukocytosis, especially a doubling of the white blood cell count over the 24-72-hour period preceding the concerning clinical exam, was an important adjunct in raising clinical suspicion for this complication. Of note, the average time interval between hospitalization for COVID-19 infection and diagnosis of bowel ischemia was 13 days, and at the time of diagnosis of the latter, nearly half of all patients had a documented improvement in their respiratory status. It is well known that viral RNA has been detected in stool samples of patients whose respiratory tests were no longer positive for COVID-19. 4 This constellation of findings should raise the clinical index of suspicion for COVID-19 bowel ischemia and help clinicians make the diagnosis in a rapid fashion, especially since these patients are often intubated, sedated, and sometimes prone, making the physical exam challenging and unreliable.
In our experience, patients with findings concerning for bowel ischemia may be too unstable to travel to the CT scanner for imaging and the decision to operate is often made without a CT scan. Therefore, having clinical and laboratory findings that may inform this decision, especially when other causes of clinical deterioration have been ruled out, is extremely useful. For patients who are deemed stable enough to undergo imaging, a CT scan of the abdomen and pelvis is preferable; otherwise, a bedside abdominal x-ray is an option to consider. In addition to the typical imaging features of bowel ischemia such as pneumatosis and portal venous gas, a notable finding is that the major mesenteric vessels were patent. In two cases, the use of colonoscopy aided the diagnosis and may be considered pre-operatively or intra-operatively if conditions warrant its use.
Several case reports have described “acute mesenteric ischemia” in COVID-19 patients with a failure to distinguish ischemia due to COVID-19 infection and ischemia due to thromboembolic phenomenon.2-4 As our experience shows, while surgical management is required in ischemic bowel necrosis, these two conditions are different in terms of their pathogenesis and overall management. Acute thromboembolic mesenteric ischemia can happen in any critically ill patient and, by definition, is due to mesenteric vascular occlusion. We found that intestinal ischemia due to COVID-19 infection is not due to major mesenteric vessel thrombosis. In fact, nearly 100% of our patients that underwent an abdominopelvic CT scan had patent mesenteric vessels on imaging. Intra-operatively, the superior mesenteric artery pulsation was typically strong on palpation. While anticoagulation and thrombo-embolectomy are major cornerstones in the management of thromboembolic bowel ischemia, there appears to be no role for them in intestinal ischemia due to COVID-19. Further supporting the lack of a role for anticoagulation in acute management is the fact that 40% of patients developed either a DVT or PT and 88% of them were on anticoagulation pre-operatively. Two of these patients were on ECMO and were fully anticoagulated pre-operatively with heparin. While these two ECMO patients were not among those that developed DVT or PE despite anticoagulation, they still developed bowel ischemia. In fact, recent data from clinical trials have shown that therapeutic anticoagulation did not reduce need for organ support in critically ill COVID-19 patients requiring ICU support. 11
The gross appearance of the ischemic bowel and the histologic findings appear to provide an insight into the potential mechanism of intestinal ischemia in COVID-19 infection. The affected bowel mostly had a distinct yellow color; the ischemia was predominantly antimesenteric; there was sharp transition from necrotic to viable bowel segment; and the mesentery was well-vascularized. Histologically, the majority of patients had findings of acute ischemic necrosis with fibrin thrombi in the small vessels of the lamina propria and submucosa. There was also evidence of acute inflammation with mucosal necrosis and mural necrosis. Our histologic findings are very similar to those reported by Ignat et al in their two COVID-19-positive patients with bowel ischemia. 12 Taken together, our findings suggest that COVID-19 infection induces a distinct acute inflammatory ischemic injury in the small vessels of the intestinal submucosa and lamina propria that is characterized by fibrin thrombi deposition and intestinal mucosal necrosis, with or without mural necrosis. However, the exact mechanism by which COVID-19 induces this is unclear. In our study, there were three cases without the typical histologic findings of fibrin deposition in the small vessels of the submucosal or lamina propria. In one case, the patient’s clinical course was clinically similar to Ogilvie syndrome, with progressive colonic dilatation prior to the diagnosis of bowel ischemia. In another case, the patient had clinical and radiologic suspicion of large bowel obstruction. In the latter, the histology showed evidence of pseudo-obstruction. Intra-operatively, these two patients did not have any evidence of mechanical large bowel obstruction. Given that the incidence of clinical or radiologic ileus in COVID-19 patients is as high as 56%, 9 the presence of a second phenotype of bowel ischemia that follows this pathway is plausible.
We tended to favor a damage control laparotomy, as these patients were often on high dose vasopressors. Sixty percent of patients had a second-look laparotomy, and on second or subsequent laparotomy, 33% of these had a bowel resection. Only 47% of those who underwent a bowel resection had an anastomosis, with twice as many of these occurring during the second or subsequent laparotomy than they did during initial laparotomy. Two patients had an anastomotic leak. While the exact etiology of these leaks is subject to speculation, we note that in one patient in this entire cohort, histology showed that the bowel resection margins showed evidence of bowel ischemia, even though the margins appeared healthy on intra-operative inspection.
A limitation of this study is that there were patients who were positive for COVID-19 and had concerning clinical features in different combinations but either did not have evidence of bowel ischemia on imaging or their families opted against any surgical intervention. Given the obvious limitations with imaging and the fact that some patients were too unstable to obtain them, the true incidence of COVID-19-induced bowel ischemia is difficult to estimate. Also, this study did not explore the risk factors for developing bowel ischemia in patients who were positive for COVID-19, neither were the exact causes of death explored. These are opportunities for future research in order to better understand opportunities for prevention or rapid diagnosis.
In conclusion, bowel ischemia is a potentially lethal complication of COVID-19 infection with typical gross and histologic characteristics. Suspicious clinical features that should trigger surgical evaluation include a new or increasing vasopressor requirement, abdominal distension, and intolerance of gastric feeds.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.