
Abstract
Introduction
Following breast cancer surgery, patients often require adjuvant radiation and chemotherapy for locoregional and systemic disease control. These procedures may result in postoperative complications, which may delay adjuvant therapy. To potentially decrease these complications, hemostatic agents may be used. This study evaluated the rate of postoperative bleeding complications and duration of Jackson-Pratt (JP) drain use in oncologic breast surgery with and without hemostatic agents.
Methods
After obtaining institutional review board approval, a retrospective chart review was performed. Patients who underwent oncoplastic breast surgery, mastectomy with or without expander/implant-based reconstruction, and subsequent reconstruction with expander to implant exchange were included. Data collected included indication for surgery, type of operation, use of hemostatic agent, specifically fibrin sealant (FS, EVICEL®, Ethicon, USA) or combination powder (CP, HEMOBLAST™ Bellows, biom’up, France), length of follow-up, time to JP drain removal, and post-operative complications (seroma, hematoma, or operating room (OR) takeback). This was a consecutive experience where initially no hemostatic agent was used, followed by use of FS, and then CP.
Results
The use of a hemostatic agent resulted in fewer bleeding complications and significantly decreased time until JP drain removal. Although not significant, subgroup analysis demonstrated that this was more pronounced in the CP group. JP drain duration was decreased among all procedures for CP compared to FS.
Conclusions
The use of hemostatic agents in oncologic breast surgery may result in decreased postoperative complications and significantly reduce time to JP drain removal.
Key Takeaways
The use of hemostatic agents in breast cancer surgery results in an overall decreased incidence of bleeding complications. The duration of time until JP drain removal is decreased with the use of hemostatic agents in breast cancer surgery.
Introduction
Improvements in surgical technique as well as the development of modern hemostatic agents have increased our ability in achieving surgical hemostasis. However, hematoma and seroma formation continue to occur in all surgical subspecialities including breast surgery that includes breast conservation in addition to mastectomy and reconstruction.1-3 Post-operative complications in major breast surgery operations such as mastectomy with or without reconstruction include seroma and hematoma with rates of 8.2% and 3.3%, respectively. 4 Major tissue rearrangement in breast surgery also includes oncoplastic surgery (OPS), which is a broad surgical field in which oncological breast surgery and plastic surgery techniques have been combined for optimal patient outcomes.5,6 Some of the common OPS techniques include local tissue rearrangement, reduction mammaplasty, mastopexy.7-10 A recent literature review of level 2 OPS techniques in the United States, which includes reduction mammaplasty and mastopexy designs, has found the rate of hematoma and seroma to be 2.26% and 1.35%, respectively. 11
Over the past several decades, the development and use of ancillary hemostatic techniques have become more available, as they assist the surgeon in achieving durable hemostasis and reducing the incidence of hematoma and seroma formation. 12 One such product is EVICEL®, a fibrin sealant that consists of BAC2 (human fibrinogen) and thrombin, that is FDA approved for surgical hemostasis. 13 An additional product is the combination powder (CP) by HEMOBLAST™ Bellows, which is made up of porcine-derived collagen, bovine‐derived chondroitin sulfate, human‐derived thrombin, and fibrinogen. 14 The HEMOBLAST™ Bellows CP has been shown to play a superior role in immediate hemostasis in several surgical subspecialities, including cardiothoracic, abdominal, and orthopedic surgery, as compared to the traditional hemostatic matrix.14-16 However, to the authors’ knowledge, the role of these two products in oncoplastic and oncologic breast surgery has not yet been studied and their effectiveness in these procedures are not validated.
Given that the role of hemostatic agents in oncoplastic surgery and breast surgery has had limited study, the aim of this study was to (1) evaluate the frequency of postoperative bleeding complications, and (2) the duration of Jackson-Pratt (JP) drain use in oncoplastic and oncologic breast surgery procedures with and without the use of either EVICEL® or HEMOBLAST™ Bellows.
Methods
A retrospective chart review was performed from a single surgeon’s case database from January 2015 to September 2020. Patients were included who underwent surgery for breast cancer, including oncoplastic breast surgery, mastectomy with or without expander/implant-based reconstruction, and subsequent reconstruction with expander to implant exchange. Those not meeting these criteria were excluded from the analysis.
Data was collected including the indication for surgery, type of operation, use of hemostatic agent, specifically fibrin sealant (FS, EVICEL®, Ethicon, USA) or CP (HEMOBLAST™ Bellows, biom’up, France), length of follow-up, duration of time to JP drain removal, and post-operative complications (seroma, hematoma, or operating room (OR) takeback).
This was a consecutive experience where initially no hemostatic agent was used, followed by use of FS (beginning June 2017), and then CP (beginning August 2019). All patients were consecutively treated within each time period. These changes were motivated by an observed increase in bleeding complications.
Of note, before operative closure of any incision site, lidocaine with epinephrine was injected for postoperative analgesia, and the surgeon made sure that the patient was not hypotensive so as to minimize the chances of missing vessels that would potentially bleed when the patient became normotensive post-operatively. No tumescent fluid was used.
JP drains were removed in the clinic when drain output was less than 30 cc/day for 2 consecutive days. JP drain output was compared between groups using Welch’s t-test. Post-operative complications were compared using Fisher’s exact test. Statistical significance was defined as P < .05.
Institutional review board approval was obtained. This study was done in accordance with the principles outlined in the Declaration of Helsinki.
Results
Rates of Post-Operative Complications and Time to JP Drain Removal Within Oncologic Breast Surgery using no Hemostatic Agent vs EVICEL® (FS) and HEMOBLAST™ Bellows (CP).
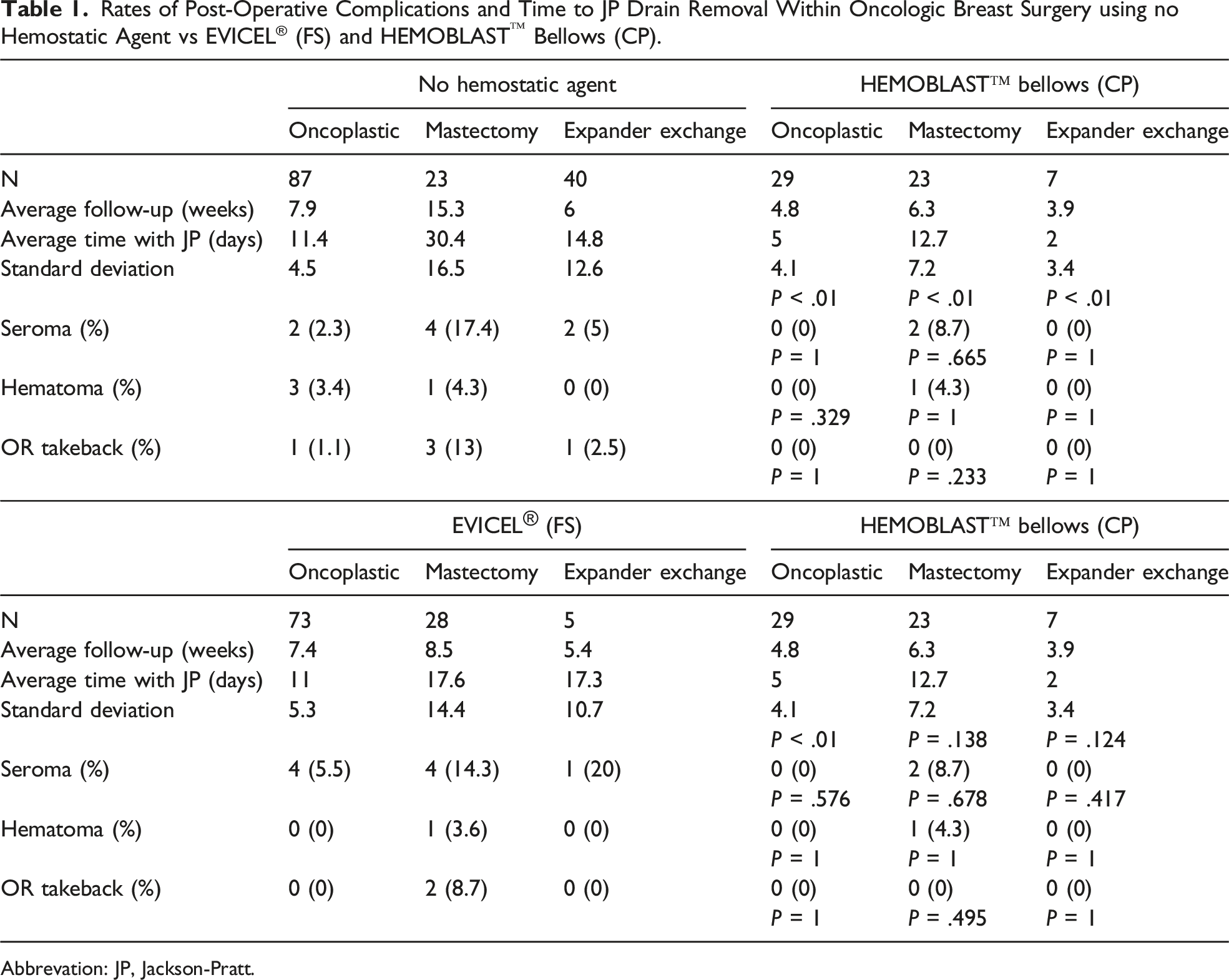
Abbrevation: JP, Jackson-Pratt.
Compared to no hemostatic agent, the use of CP was resulted in decreased incidence of seroma, hematoma, and return to OR, especially in the mastectomy group, with an 8.7% seroma and 0% return to OR rate in the CP group (n = 23), as compared to 17.4% seroma and 13% return to OR rate in the non-hemostatic agent group (n = 23). These were without statistical significance. Additionally, JP drain duration was statistically significantly decreased in the CP group as compared to the non-hemostatic agent group among oncoplastic (5 vs 11.4 days, P < .01), mastectomy (12.7 vs 30.4 days, P < .01), and expander exchange (2 vs 14.8 days, P < .01) operations.
Subgroup analysis demonstrated that the CP group experienced no hematomas, seromas, or return to OR for the oncoplastic (n = 29) and expander exchange (n = 7) procedures as compared to the FS group with a 5.5% seroma rate in oncoplastic (n = 73) and 20% seroma rate in expander exchange operations (n = 5). The seroma rate after mastectomy was 8.7% with CP (n = 23) compared to 14.3% with FS (n = 28). The OR takeback rate after mastectomy was 0% with CP (n = 23) compared to 8.7% (n = 28) with FS. These differences in post-operative complications were without statistical significance. Lastly, JP drain duration was statistically significantly decreased among oncoplastic (5 vs 11 days with P < .01), but not mastectomy (12.7 vs 17.6 days with P = .138), and expander exchange (2 vs 17.3 days with P = .124) for CP as compared to FS (Figure 1). Duration of time to Jackson-Pratt drain removal (* = statistically significant as compared to no hemostatic agent, # = statistically significant as compared to EVICEL® (FS)).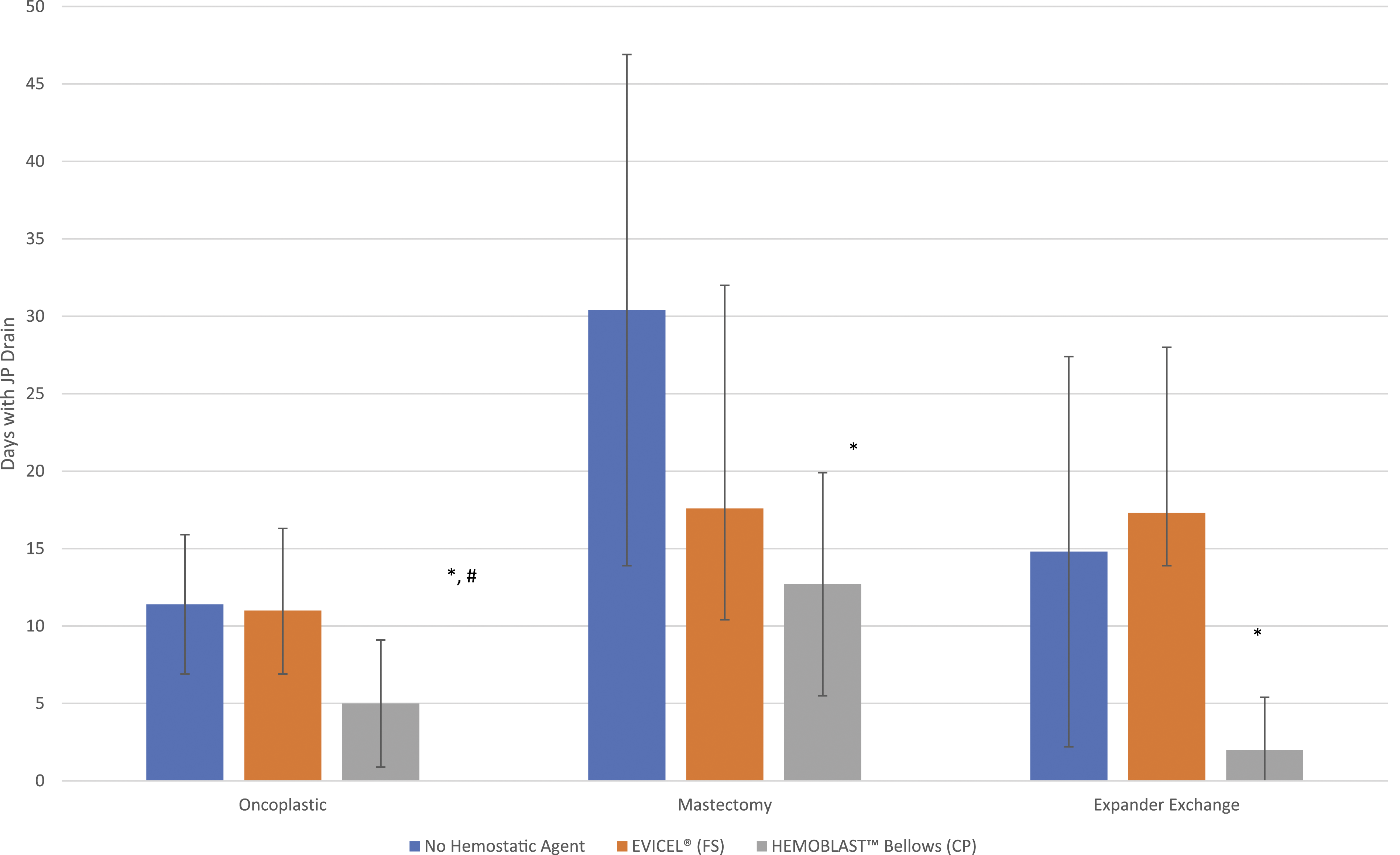
Discussion
Oncoplastic surgery is an innovative reconstructive approach that has continued to gain in popularity for certain patient populations. Women with large tumors and moderate to large ptosis can benefit from a partial mastectomy while utilizing local tissue for rearrangement in order to reconstruct the breast. The large partial mastectomy allows for decreased positive margins while the implementation of autologous tissue creates an optimal aesthetic outcome.17,18 Oncoplastic surgery showed the most favorable PROMs when compared to other reconstructive modalities. 19 Its oncologic utility lies in the ability to perform a large partial mastectomy, resulting in a decreased positive margin rate, while utilizing local tissue rearrangement to reconstruct the breast. OPS can be further categorized into level 1 volume displacement, level 2 volume displacement, and volume replacement based on the American Society of Breast Surgeons definitions. 20
However, similar to all procedures, OPS and other oncologic breast surgery, including mastectomy and expander/implant-based reconstruction, is not without associated complications. Seromas and hematomas are a relatively common complication due to increased dead space created from the surgical process. Surgical complications can result in delays of adjuvant radiation and chemotherapy leading to worsened outcomes. 21 Therefore, the use of hemostatic agents can possibly reduce these complications. Our results noted decreased hematoma and seroma formation when hemostatic agents were used in addition to statistically significantly lower drain duration times. The latter decreases patient discomfort and theoretically prevents the chances of drain infections. It is interesting to note that even with statistically decreased drain times, the hemostatic agent groups showed a decreased incidence of seromas supporting a mechanism for decreased post-operative seroma complications other than the presence of a drain. This could be due to the ability of the hemostatic agents to collapse deadspace, something that is seen in the abdominoplasty/plastic surgery literature. 22
This is the first study to examine these agents in oncologic breast surgery and evaluate their efficacy. Examining postoperative outcomes from hundreds of patients, the use of CP and FS resulted in a decreased incidence of postoperative complications, including seroma, hematoma, and OR takeback, with a more pronounced effect in the CP group when examining time prior to JP drain removal. Therefore, the use of the agents could potentially decrease delays in further therapies and improve outcomes. In general, decreased post-operative complications leads to improved patient satisfaction outcomes and decreased cost burden further underscoring the importance in the study of technologies that can aid surgical technique.23,24
While this study is novel, it is not without limitations. Although this study incorporated many patients, all oncologic breast surgery procedures were performed at a single institution, by a single surgeon. Therefore, larger studies at multiple sites will better address whether this data is reproducible and generalizable. In addition, it is important to mention that this study was retrospective and not blinded, which could potentially introduce bias. However, it is not feasible to blind the surgeon to which product is being used due to the differences in product preparation. Furthermore, while promising post-operative outcomes were noted, the lack of statistical significance favoring hemostatic agents could be related to sample size with larger samples possibly showing statistical significance with avoidance of a potential Type II statistical error. It should also be mentioned that the cost of the hemostatic agent is an important consideration that contributes to the overall cost of the operation. A cost-effectiveness analysis examining the use of these two hemostatic agents compared to no hemostatic agent would be worthwhile to rationalize the routine use of hemostatic agents in breast surgery.
Future studies should be performed to evaluate long-term outcomes to greater assess the utility of hemostatic agents in this population, especially with regard to mitigating delays in adjuvant therapy. In the end, we hope to provide a more detailed and standardized data set incorporating many institutions in order to analyze outcomes more precisely and accurately.
Conclusion
The use of hemostatic agents in oncologic breast surgery significantly shortens time to JP drain removal and may decrease postoperative complications, including seroma, hematoma, and OR takeback. Subgroup analysis of the individual hemostatic agents demonstrated a statistically significant decreased duration of time prior to JP drain removal in the oncoplastic group. in the CP group as compared to FS.
Data Availability Statement
The data that support the findings of this study are available on request from the corresponding author. The data are not publicly available due to privacy or ethical restrictions.
Footnotes
Acknowledgments
Thank you to all who helped make this project possible.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was supported in part by an Investigator Initiated Study grant from Biom’Up. Dr Chatterjee is a consultant for Biom’Up.