
Abstract
Health insurance gives families access to medical services and protects them against the costs of illness and medical treatment. Insured children are more likely than their uninsured peers to use medical services, preventive health services, have a usual source of care, and have fewer unmet medical needs. In this article, we review trends in health insurance coverage for Hispanic children and the factors that influence their coverage. We then discuss health care utilization among Hispanic children and barriers to health care utilization. We conclude with a discussion of strategies to improve Hispanic children’s health care access in the age of COVID-19.
Children who are covered by health insurance are more likely than their uninsured peers to use medical services and preventive health services, have a usual source of care, and have fewer unmet medical needs (Paradise 2014). Insurance has positive impacts on childhood health, which in turn has lasting effects on adult educational attainment, employment, and future earnings from work (Guzman, Chen, and Thomson 2020; Case, Fertig, and Paxson 2005).
The United States is the only rich democracy in the world that has a large proportion of its population without health insurance. About 30 million persons in the United States, including more than 4 million children, were uninsured in 2019. The absence of universal health care means that widespread disparities in health insurance exist in the United States. Insurance coverage varies by income, employment, state of residence, race/ethnicity, citizenship, immigration status, and age.
Hispanic children have long had high uninsured rates. In 2000, 26.1 percent of Hispanic children were uninsured, compared to 8.2 percent of non-Hispanic (NH) white and 15.6 percent of NH Black children (Larson et al. 2016). There has been substantial progress in reducing uninsured rates among Hispanic children over the past two decades, due largely to expanded enrollment in public insurance programs and the impact of the Affordable Care Act (ACA). But disparities persist, and progress in insuring Hispanic children has reversed since 2017. Moreover, the COVID-19 pandemic has laid bare weaknesses and inequities in U.S. health insurance and medical care delivery that disproportionately impact Hispanic families.
Higher uninsured rates mean that Hispanic children use fewer medical services than NH white or NH Black children and are more likely to have unmet medical needs (Larson et al. 2016). Yet lack of insurance coverage is not the only barrier to Hispanic children’s use of medical services. Their access to medical services is also hindered by employment policies limiting parental access to benefits such as sick leave, inadequate public transportation services in their communities, a lack of culturally and linguistically appropriate care, and climates of fear and mistrust. This article summarizes the evidence on Hispanic children’s access to health insurance and use of health care. We conclude by discussing strategies that could improve their access to health care in the context of the COVID-19 pandemic and Biden administration.
Health Insurance Coverage
Americans obtain health insurance from both private sources via employment, direct purchase, or ACA-organized purchasing pools and public programs such as Medicaid, the Children’s Health Insurance Program (CHIP), and Medicare (which covers persons 65 and older as well as younger persons with permanent disabilities who qualify for Social Security Disability Insurance). Most Americans under age 65 obtain coverage through employer-sponsored insurance (ESI), which may cover family members in addition to workers. Persons can also purchase private plans through the ACA’s Health Insurance Marketplace, where low- and modest-income enrollees can qualify for subsidies to help them afford coverage, or from private insurers outside of the marketplace. Medicaid, which is administered by the states within federal rules and with joint state/federal funding, covers low-income persons. Also operated by the states, CHIP covers children in families with modest incomes that earn too much to qualify for Medicaid.
In addition to these insurance arrangements, the United States has a de facto safety net of institutions that directly provide medical services, often to persons who are uninsured or enrolled in Medicaid, for modest or no charges. These Federally Qualified Health Centers (FQHCs), community health centers, and county and city health departments play a vital role in providing medical services to many uninsured Americans and have been an important site of medical care for uninsured Hispanic patients (Perreira and Cofie 2016). Indeed, “Latinos account for more than 35% of patients at community health clinics and health centers (CHCs) nationally” (Ortega, Rodriguez, and Bustamante 2015, 530).
In contrast to countries like Canada or Britain, the United States does not have a single health program that covers the entire population regardless of age, employment, or income. American health care is less a system than a patchwork that has myriad holes, and many Hispanic adults and their children fall through those holes. In 2019, 30 percent of Hispanic adults aged 18 to 64 were uninsured, compared to 14.3 percent of NH Black and 10.2 percent of NH white adults (Cha and Cohen 2019). In 2019, 9.2 percent (N = 1.8 million) of Hispanic children were uninsured, compared to 5.6 percent of NH white (N = 1.7 million) and 4.6 percent (N = 0.5 million) of NH Black children; nearly 40 percent of all uninsured children in the United States are Hispanic (Alker and Corcoran 2020).
These national rates obscure a broader pattern of geographic variation in insurance coverage of Hispanic children, with the highest rates of uninsured concentrated mostly in southern and southwestern states (see Figure 1). Over one-third of all uninsured Hispanic children in the U.S. live in Texas, where nearly 15 percent of Hispanic children lack health coverage (Whitener et al. 2020). Health insurance coverage varies as well by income. In 2018, 6 percent of Hispanic children were uninsured in families with incomes at 250 percent or more of the Federal Poverty Level (FPL), compared to 9.9 percent for children in families with incomes between 138–249 percent FPL, and 8.7 percent for children in families making less than 138 percent FPL (Whitener et al. 2020).
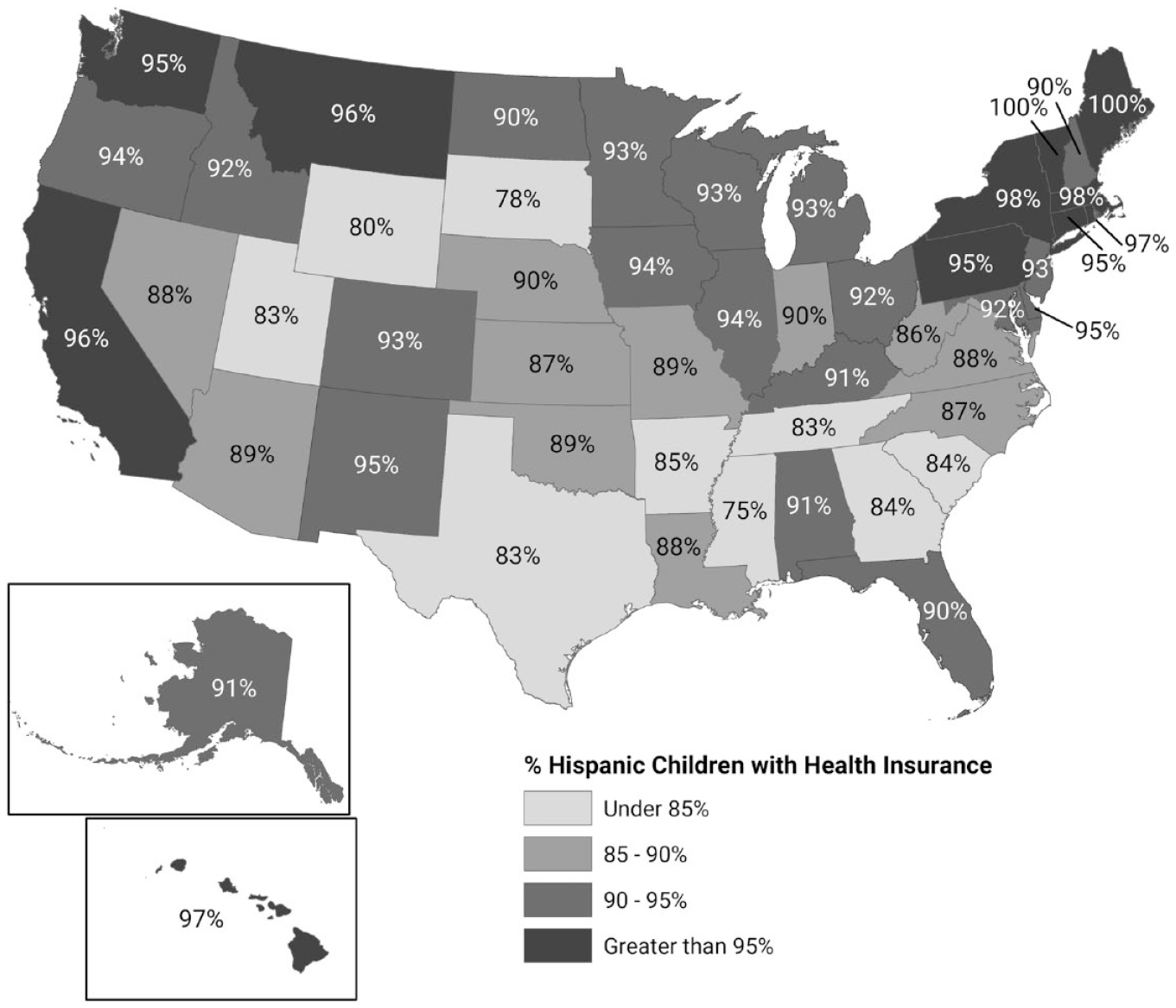
Percentage of Hispanic Children (Ages 0–18) with Health Insurance in 2019, by State
Employer-sponsored insurance (ESI)
The limited availability of health insurance to Hispanic adults directly affects insurance coverage for their children. Only 42.5 percent of nonelderly (ages 0–64) Hispanics had insurance through employers in 2019, compared to 65.8 percent of NH whites and 47.2 percent of NH Blacks (Kaiser Family Foundation, n.d.). The relatively low rate of ESI reflects the fact that many Hispanic adults work in jobs (often low-wage, part-time jobs) that do not provide health insurance, which means that their children have less access to such coverage (Alberto, Pintor, Langellier, et al. 2020). Noncitizens, especially undocumented immigrants, are particularly likely to work in these precarious, low-quality jobs (Young and Mattingly 2016; Massey, Durand, and Pren 2016). In 2019, 31.9 percent of Hispanic children were covered through ESI, compared to 48.1 percent of all children (see Figure 2). While the ACA allows parents to keep their children on their employer insurance plans until age 26, fewer Hispanic families can take advantage of this benefit because of their relatively limited access to employer coverage.
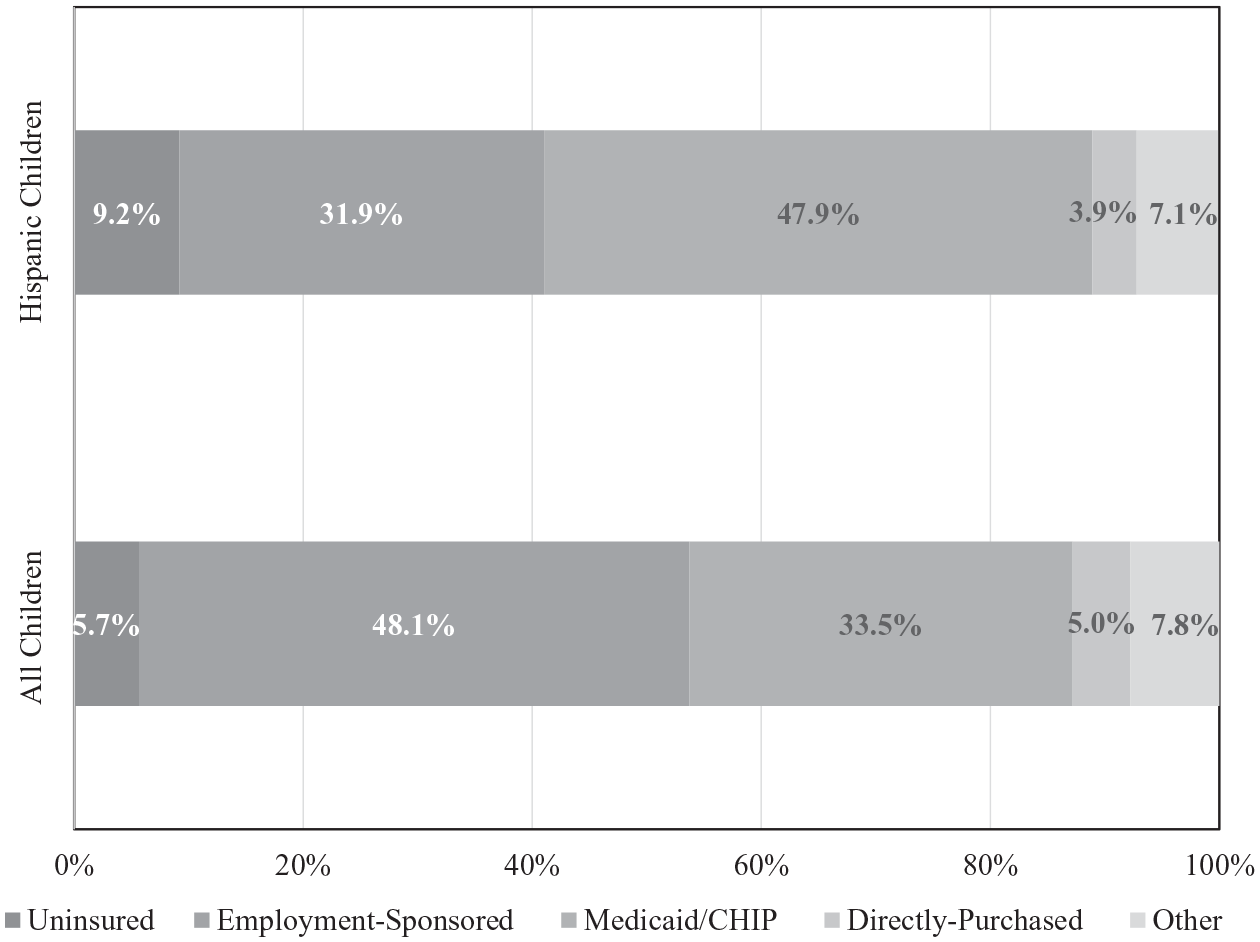
Sources of Health Insurance Coverage for Hispanic Children Compared to All Children (Ages 0–18), 2019
Medicaid and CHIP
As a result of their lower access to ESI, 47.9 percent of Hispanic children are insured through Medicaid and CHIP (Figure 2). However, Medicaid eligibility varies substantially by state for adults; states make policy and political decisions about the availability of health insurance for low-income populations that structure individuals’ access to insurance coverage. Twelve states, mainly in the South, have not expanded Medicaid under the ACA, which leaves many low-income persons in those states without any affordable insurance options. Because parents having health insurance is tightly coupled with children having insurance, the absence of Medicaid expansion in these states reduces children’s coverage (Hudson and Moriya 2017). Interstate variation also occurs in Medicaid/CHIP income eligibility levels for children, although the variation is less than for Medicaid’s coverage of adults. Consequently, states vary widely in the percentage of Hispanic children enrolled in Medicaid/CHIP (see Figure 3). Hispanic children’s uninsured rate was 5.1 percent in Medicaid expansion states and 12.9 percent in nonexpansion states in 2018 (Whitener et al. 2020).
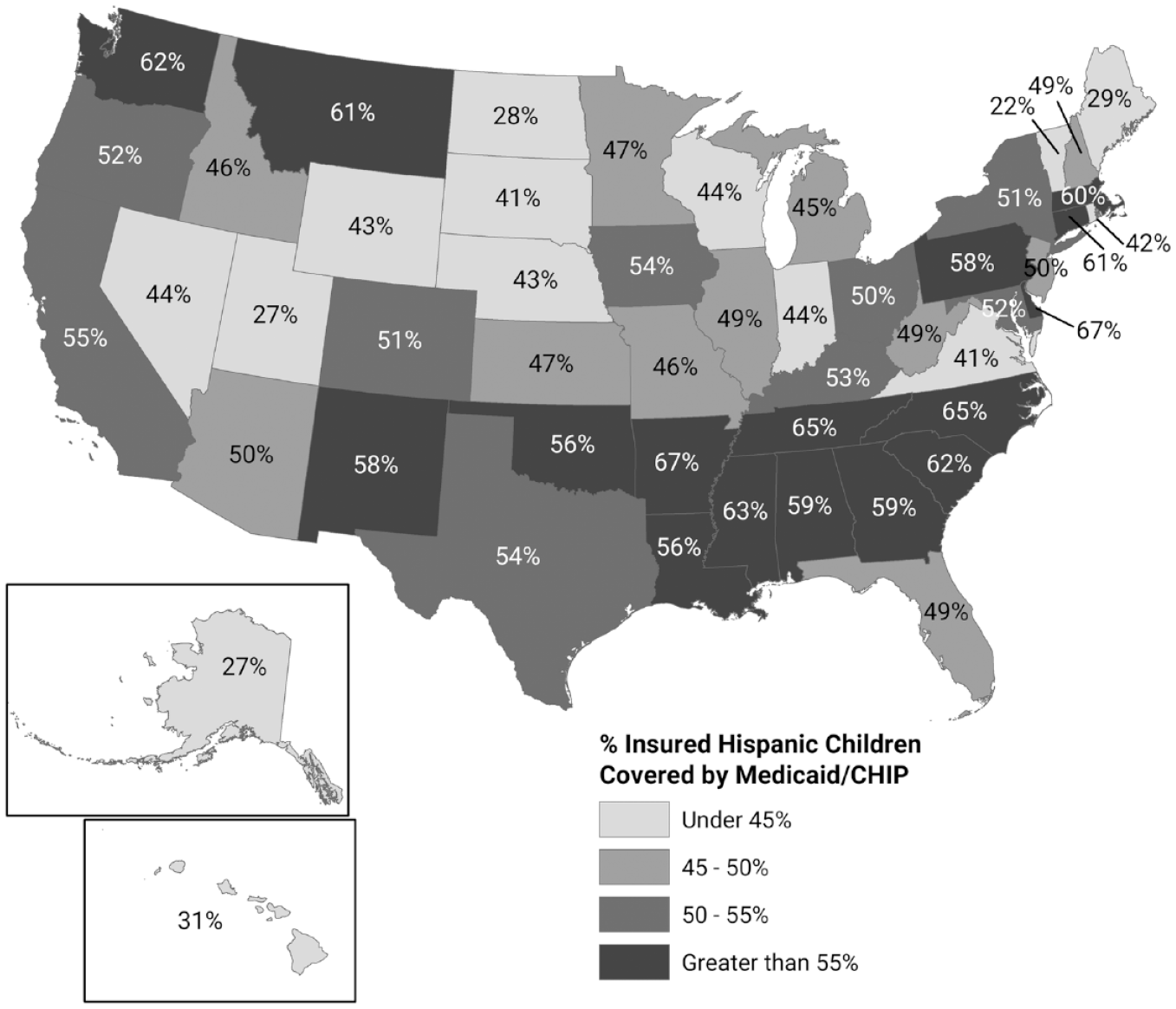
Percentage of Hispanic Children (Ages 0–18) with Medicaid/CHIP Coverage in 2019, by State
Limits on Hispanic children’s access to insurance coverage
Even in Medicaid expansion states, Hispanic children can face substantial barriers to insurance coverage. Although 95 percent of Hispanic children are citizens, 34 percent of these citizen children “live in mixed-status households (i.e., with at least one non-citizen parent)” (Whitener et al. 2020, 10). In these mixed-status families, children may be eligible for health insurance while their parents are not. Parents’ nativity status has an enormous impact on Hispanic children’s insurance coverage (Guzman, Chen, and Thomson 2020). In 2019, noncitizen Hispanic children had an extraordinarily high uninsured rate—51.6 % however, only 4.5 percent of Hispanic children were not U.S. citizens so this group comprises a small share of uninsured Hispanic youth (Figure 4). Additionally, as Figure 4 shows, 10.4 percent of Hispanic, citizen children with a noncitizen parent were uninsured, compared to 5.3 percent of Hispanic, citizen children with U.S.-born parents. Overall, U.S.-born Hispanic children “with immigrant parents are more likely to be uninsured and to have discontinuous health coverage” (Alberto, Pintor, Langellier, et al. 2020, 2).
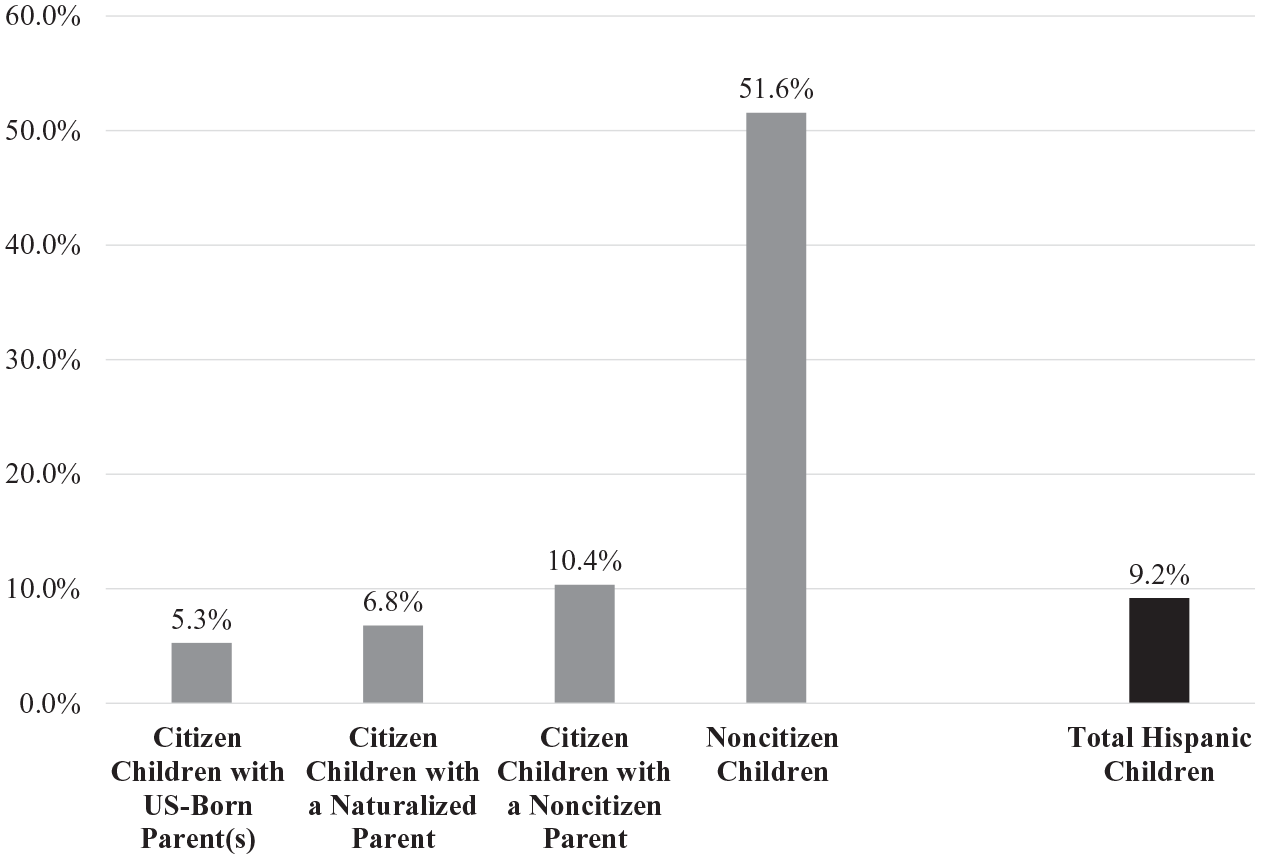
Uninsured Rates among Hispanic Children (Ages 0–18) in 2019, by Children’s and Parents’ Citizenship Status
Some children are ineligible for Medicaid and CHIP because of policies restricting immigrant families’ access to public assistance programs (Bitler et al. 2021). Eligibility for these programs has always been restricted to lawfully present immigrants and U.S. citizens. However, as Bitler et al. (2021) detail, the Personal Responsibility and Work Opportunity Reconciliation Act (PRWORA) of 1996 imposed new restrictions on lawfully present immigrants’ access to federally funded health insurance. Under PRWORA, only certain “qualified” immigrants—such as legal permanent residents, refugees, and asylees—can gain coverage through insurance programs and then only if they have lived in the United States for at least five years. And while all lawfully present immigrants are eligible under the ACA to purchase private coverage through the ACA’s Insurance Marketplace, unauthorized immigrants are barred from doing do, even if they use their own money (Ortega, Rodriguez, and Bustamante 2015).
The 2009 Children’s Health Insurance Program Reauthorization Act (CHIPRA) loosened PRWORA’s eligibility restrictions. States can choose to extend Medicaid and CHIP coverage, with federal funding, to qualified immigrant children who have lived in the United States for fewer than five years and cover nonqualified immigrants with state-only funds. In 2019, thirty-four states extended coverage to children who had been in the United States fewer than five years, and six states (California, Illinois, Massachusetts, New York, Oregon, and Washington) and the District of Columbia covered unauthorized immigrant children in Medicaid/CHIP (Whitener et al. 2020).
However, many children who are eligible for Medicaid/CHIP are not enrolled. Parents not receiving Medicaid are less likely to enroll their eligible children in Medicaid/CHIP than parents who are enrolled in Medicaid. Additionally, confusion regarding eligibility rules for Medicaid/CHIP as well as the complexity of some states’ enrollment procedures create obstacles to children’s coverage. Such obstacles to coverage are more formidable in families where parents are immigrants. They may encounter language barriers in accessing coverage options and be less familiar with America’s byzantine health insurance arrangements. Many also fear interactions with government officials who may make inquiries into their and family member’s immigration status as well the consequences for that status of enrolling their children in public programs (Pintor et al. 2018).
The ACA and Hispanic children’s insurance coverage
The years following the ACA’s enactment saw substantial progress in reducing Hispanic children’s uninsured rate, which dropped from 15.1 percent in 2010 to 7.7 percent in 2016 (Whitener et al. 2020). Those gains reflected ACA policies that boosted coverage among adults, which led to an increase in parents enrolling children in coverage. Such policies included expanding Medicaid eligibility and income-related subsidies to help uninsured persons buy private coverage, as well as measures to promote outreach and help screen persons for public insurance program eligibility (Hudson and Moriya 2017; Pintor et al. 2018). Nevertheless, reflecting long-standing differences in citizenship and immigrant status, uninsured rates varied substantially across different Hispanic backgrounds. During 2014 to 2016, following implementation of the ACA’s major coverage provisions, relatively low percentages of Puerto Rican (2.5 percent) children lacked health coverage, while children from Mexican (9.9 percent) and Central or South American (9.1 percent) backgrounds had much higher uninsured rates (Pintor et al. 2018).
In recent years, the coverage gains among Hispanic children that followed the ACA’s enactment have reversed, part of a broader decline in insurance coverage among children. Between 2017 and 2019, the number of all uninsured children in the United States grew by 726,000, increasing the uninsured rate for children from 4.7 percent to 5.7 percent (Alker and Corcoran 2020). Concentrated among Hispanic children with foreign-born parents, much of this increase likely reflects restrictive immigration policies that made families reluctant to enroll children in public programs because they feared it could jeopardize their immigration status (Guzman, Chen, and Thomas 2020).
In particular, in 2018 the Trump administration announced a new “public charge” rule that denied legal permanent residency to immigrants who received a range of government programs, including Medicaid. Although use of Medicaid by persons under age 21 was excluded from determination of public charge in the final rule and the rule was subject to legal challenges, the announcement of this policy had a chilling effect on children’s Medicaid enrollment (Barofsky et al. 2020; Bitler et al. 2021). That reduction was largely due to confusion about the rule’s provisions; in a 2019 Urban Institute survey, “over three-quarters (76.8 percent) of adults in immigrant families with children did not understand that children’s enrollment is not [a] factor in their parents’ public charge determination” (Haley et al 2020, 9). In total, during 2016 to 2019, noncitizen participation in Medicaid/CHIP for persons with incomes below 200 percent FPL declined by 20 percent, compared to 8 percent for U.S-born citizens and 5 percent for naturalized citizens, underscoring the public charge rule’s chilling effect on enrollment in such programs (Capps, Fix, and Batalova 2020). Additionally, states, with the encouragement of the Trump administration, adopted policies that made it more difficult to enroll and stay enrolled in public insurance programs (Guzman, Chen, and Thomas 2020). Moreover, prior research has also shown that immigration enforcement activities increase fear in immigrant communities, lead individuals to avoid interactions with government officials, and thereby reduce participation in public programs like Medicaid (Perreira and Pedroza 2019).
Health Care Utilization
Health care utilization is highly dependent on health insurance coverage. Health care utilization can be viewed as a choice or behavior influenced by individual characteristics as well as broader societal determinants. The Expanded Health Belief Model, widely used to understand health and illness behaviors, proposes that health care utilization occurs in response to perceived susceptibility to and severity of illness, perceived benefits and costs (including nonmonetary costs) of medical care, self-efficacy to seek and obtain medical care, and cues to action (e.g., information, people, and events) that motivate individuals to seek and obtain care (Rosenstock, Strecher, and Becker 1988). A second commonly used framework to understand utilization, Anderson’s Socio-Behavioral Model, proposes that societal norms, public health technologies, and the organization and availability of health care resources shape health care utilization at a societal level (Derose et al. 2009; Carrillo et al. 2011). In turn, individual health care utilization occurs in response to individual predisposing (e.g., demographic characteristics, socioeconomic background, and health beliefs), enabling (e.g., insurance, established patient-doctor relationships, and availability of care in the community), and need factors (e.g., perceived illness and severity).
Such models, though, do not adequately capture the realities of health care utilization among children. Children’s use of medical services is often not their own choice but, rather, a decision made by parents and other family members to seek care for them. Consequently, children’s utilization of medical care largely reflects the health beliefs, socioeconomic circumstances, and access to insurance and other health care resources of their families. Moreover, standard models of health care utilization do not sufficiently account for the systemic, structural barriers to care that make Hispanic children, especially Hispanic children of immigrants, vulnerable to having unmet physical and mental health needs (Bourgois et al 2017; Larson et al. 2016).
Disparities in utilization
Health care utilization by Hispanic children generally follows the same pattern of health care utilization by Hispanic adults (Bustamante et al. 2010, 2009; Derose et al. 2009). Hispanic children on average have more unmet medical needs and use fewer health care services than NH white and NH Black children (Larson et al. 2016; Newacheck et al. 2000). However, their use of services varies substantially by health insurance status and the key factors determining access to health insurance—state of residence, children’s nativity, and parents’ nativity. In this section, we evaluate trends in Hispanic children’s utilization, focusing on indicators of unmet need, a medical home, well-child visits, childhood vaccination rates, emergency department (ED) use, and mental health care use. In the following section, we examine the barriers that Hispanic children and their parents face to utilizing health care.
Unmet medical need
After rising from 10.5 percent to 13.6 percent between 2000 and 2008, unmet need declined to 8.8 percent among Hispanic children in 2014 (Larson et al. 2016). In 2020, 7 percent of first-generation (foreign-born children with foreign-born parents), 3 percent of second-generation (U.S.-born children with a foreign-born parent), and 5 percent of third-generation (U.S.-born children with U.S. born parents) Hispanic children reported that at least once over the past 12 months they were unable to access needed medical, dental, prescription medications, or other health care (Koball and Hartig 2020). These reductions in unmet needs during 2008 to 2020 have been attributed to the CHIPRA option that expanded Medicaid eligibility as well as other policies that expanded immigrants’ rights (e.g., sanctuary policies) (Saloner, Koyawala, and Kenney 2014; Koball and Hartig 2020). Reductions in unmet needs also reflected the ACA’s impact in boosting insurance coverage rates among Hispanic children. Compared to those without insurance, children with public health insurance have greater odds of having a usual source of care, a doctor’s visit in the past year, and a preventive care visit in the past year (Langellier et al. 2016). Using regression-based decomposition models, Langellier et al. (2016, 141) conclude that “differences in health insurance status between Latinos and Whites contribute 58 percent to the explained disparity in having a usual source of care, 27 percent to disparity in delayed care,18 percent to disparity in having visited the doctor in the previous year, and 17 percent to disparity in receiving a preventive care visit.”
Medical home
Establishing a medical home can be a critical first step in reducing unmet medical needs among children. The medical home is a health care delivery model intended to promote cost savings, use of preventive care, satisfaction with care, and better health. It is measured by asking whether children have a personal doctor or nurse and a usual source for sick care, and whether they receive needed referrals, effective care coordination, and family-centered care. The vast majority (94 percent) of Hispanic children have a usual source of care; and after adjusting for a variety of factors, researchers find no differences in having a usual source for those living in emerging (rather than established) immigrant destinations (Larson et al. 2016; Saloner and Gresenz 2016). However, Hispanic children with parents who do not speak English are significantly more likely than those with parents who speak English to have no usual source of care (20.6 percent vs. 8.2 percent). And U.S.-born Hispanic children with foreign-born parents were also significantly more likely than those with U.S-born parents to have no usual source of care (15.7 percent vs. 6.6 percent) (Avila and Bramlett 2013). These parents are also more likely to report that they have problems getting referrals, effective care coordination, and family-centered care (Avila and Bramlett 2013). Consequently, nearly 62 percent of Hispanic children (compared to 32 percent of NH white children) were categorized in 2007 as having no medical home (Avila and Bramlett 2013).
Well-child care
The American Academy of Pediatrics (AAP; 2020) recommends well-child visits annually (more frequently from age zero to three). At well-child visits, children receive developmental, social, physical, mental/behavioral, hearing, dental, and vision screenings, as well as vaccinations (AAP 2020). Three-quarters of Hispanic youth receive timely well-child care (Ortega et al. 2018). Foreign-born children have lower preventive care use than U.S.-born children (Ortega et al. 2018), and unauthorized immigrant children are less likely to receive preventive care, compared to authorized immigrant children (Pourat et al. 2014). The ACA has improved access to preventive care for Hispanic children but has not narrowed Hispanic–NH white disparities (Ortega et al. 2018). Immigration enforcement and state laws that restrict immigrants’ rights are associated with lower utilization of preventive care among Hispanic children of immigrants (Perreira and Pedroza 2019). In contrast, expansions in immigrants’ rights are associated with better access to a medical home and preventive care (Koball and Hartig 2020).
Vaccinations
Childhood vaccinations include MMR (measles, mumps, and rubella), DTaP (diphtheria, tetanus, pertussis), chickenpox, HPV (human papillomavirus), and an annual flu shot (AAP 2020). Approximately 72 percent of all Hispanic children receive recommended childhood vaccinations by age three, a vaccination rate similar to the rate (73 percent) among NH white children (Hill et al. 2016). However, Hispanic children under age three are less likely than white children (79 percent vs. 82 percent) to receive an annual flu vaccine (Anandappa et al. 2018). Among Hispanic children, vaccination rates also differ substantially by income, with lower-income children having lower vaccination rates (Walsh, Doherty, and O’Neill 2016).
Emergency department care
About 12 percent of both Hispanic and NH white children have had an ED visit in the past year (Schlichting et al. 2017). Children with citizen mothers are more likely than children with noncitizen mothers to utilize the ED (Langellier et al. 2016; Alberto, Pintor, Martínez-Donate, et al. 2020). Unauthorized and authorized immigrant children visit the ED at similar rates (Pourat et al. 2014). Medicaid-insured children visit the ED at the highest rates, uninsured children at the lowest rates (Schlichting et al. 2017). When uninsured children (including unauthorized immigrant children) visit an ED for emergency care, their care can be covered by Emergency Medicaid. Access to FQHCs (key sources of preventive care for Hispanic children) is associated with reduced ED use among both uninsured and Medicaid-insured children (Nath et al. 2016).
Mental health care
Only 54 percent of Hispanic children (ages 2–17) who need mental health care receive it (Lu 2017). First-generation Hispanic children are less likely than second- and third-generation children to receive mental health care. Children of unauthorized immigrant parents are the least likely to receive needed services (Finno-Velasquez et al. 2016). States can reduce these disparities by funding culturally responsive care. For example, changes in California’s Medicaid funding rules encouraging counties to provide culturally and linguistically sensitive services decreased Hispanic-white disparities in mental health care utilization (Snowden et al. 2017).
Barriers to care
The literature identifies five critical barriers to health and human services for Hispanic children and their parents: (1) medical costs, (2) nonmedical costs (e.g., sick leave), (3) transportation, (4) knowledge and communication, and (5) fear and mistrust (Carillo et al. 2011; Perreira et al. 2012). Each of these barriers is magnified for the children of immigrants, whose access to care is explicitly limited by policies of exclusion directed at foreign-born persons living in the United States (Perreira and Pedroza 2019).
Medical costs
Medical costs, the primary financial barrier to care, include the costs of health insurance premiums, copayments, and deductibles. In national studies, 14 percent of Hispanic adults experienced financial barriers to care (Kullgren et al. 2012). Financial barriers to care are greater for those who are uninsured, parents, and parents who have a child with a chronic illness (Kullgren et al. 2012; Flores, Olson, and Tomany-Korman 2005). Uninsured and underinsured Hispanic children are more likely to have unmet medical, dental, and vision care needs than insured Hispanic children (Larson et al. 2016; Newacheck et al. 2000). They often do not seek preventive care services (e.g., annual check-ups), delay recommended tests and treatments, and forgo necessary prescription medications (Langellier et al. 2016; Ortega et al. 2018).
Nonmedical costs
Financial barriers to care can also result from nonmedical costs that increase the difficulty of accessing care. One national study reported that 55 percent of Hispanic adults in the workforce had no access to sick leave (DeRigne, Stoddard-Dare, and Quinn 2016). For Hispanic parents who work low-wage jobs without sick leave or family medical leave, taking time off to care for sick children can result in loss of income or even a job (UnidosUS 2019). For Hispanic parents living in medically underserved inner-city or rural areas, nonmedical barriers also include long travel and wait times for primary and specialty care providers (Flores et al. 2002). Insurance preauthorization requirements, complex forms to ensure payment or reimbursement for the cost of care, and other challenges navigating health care systems in the United States further diminish the likelihood of health care utilization (Carillo et al. 2011; Perreira et al. 2012).
Transportation
Transportation, a major nonmedical cost limiting access to care, is frequently cited by Hispanic parents as a reason for delaying their children’s medical care and missing their appointments (Nageswaran, Rosado, and Beveridge 2018). Moreover, limited transportation has been associated with lower preventive and primary care use and higher ED use (Syed, Gerber, and Sharp 2013). Hispanic parents may lack transportation for a variety of reasons. For example, lower-income parents may not be able to afford a car, parents with low literacy may not be able to complete a driver’s license test, and unauthorized immigrant parents may not be able to obtain a driver’s license. Only fifteen states and the District of Columbia have enacted laws to allow unauthorized immigrants to obtain driver’s licenses (National Conference of State Legislators [NCSL] 2020). In addition, public transportation may not be routinely available in either the rural or inner-city areas in which many Hispanic families live. Although states are federally mandated to provide nonemergency medical transportation (NEMT) to Medicaid beneficiaries, access to these services varies across states, and children who are not enrolled in Medicaid do not have access to such services (Musumeci and Rudowitz 2016).
Knowledge and communication
Beliefs about illness, prevention, and appropriate treatment; awareness about health care resources; understanding of diagnoses and treatments; health care literacy, patient-provider language concordance; the availability of translation and interpretation services; and cultural misunderstandings can all contribute to the underutilization of medically necessary care, medical errors, and dissatisfaction with the quality of care (Flores, Olson, and Tomany-Korman 2005). In national U.S. studies, 21 percent of Hispanic adults experienced these nonfinancial barriers to care, which, like financial barriers, are greater for parents (Kullgren et al. 2012). To help address these barriers, the U.S. Department of Health and Human Services (U.S. DHHS) adopted national standards for Culturally and Linguistically Appropriate Services (CLAS) in 2013 (U.S. DHHS 2013). Additionally, Title VI of the 1964 Civil Rights Act and provisions of the ACA require that culturally and linguistically appropriate care be available to patients (U.S. DHHS 2013; Chen, Youdelman, and Brooks 2007). Yet the availability of culturally and linguistically appropriate care continues to be a primary barrier for Hispanic adults and their children, especially those who are immigrants and living in regions of the country with fewer established Hispanic populations (Derose et al. 2009; Cunningham, Hibbard, and Gibbons 2011).
Fear and mistrust
As federal-, state-, and county-level policies have been adopted to reduce access to health and human services for immigrant populations in the United States, marginalize English-language learners, and increase the deportation of unauthorized immigrants, climates of fear and mistrust could now pose one of the greatest barriers to health care for Hispanic parents (Perreira and Pedroza 2019; Pedraza, Nichols, and LeBrón 2017). In one national study using data collected in 2015, 80 percent of Hispanic adults indicated that they believed that there was an anti-Hispanic or anti-immigrant environment in the United States today, 45 percent worried that their friends or family members might be detained or deported due to their immigration status, and 9 percent indicated that they would avoid visiting a health care provider because they do not want to be asked about their citizenship (Sanchez, Pedraza, and Vargas 2015; Vargas and Ybarra 2017). Consequently, numerous studies have found that noncitizen Hispanic parents are more likely to delay medical care, forgo annual check-ups, and avoid ED use for their children (Alberto, Pintor, Martínez-Donate, et al. 2020; Alberto, Pintor, Langellier, et al. 2020, Langellier et al. 2016).
Strategies to Improve Health Care Access in the Age of COVID-19
In sum, even after substantial progress produced by the ACA and other public policies, myriad barriers to health insurance coverage and use of medical care services persist among Hispanic children. Moreover, the COVID-19 pandemic has worsened inequalities and magnified persistent gaps in U.S. health care, with a disproportionate impact on Hispanics. As of November 2020, the Centers for Disease Control and Prevention (CDC) reported that Hispanics were 1.7 times more likely than NH white persons to have had COVID-19, 4.1 times more likely to have a COVID-related hospitalization, and 2.8 times more likely to die from COVID (CDC 2020). Hispanics are more likely to contract COVID partly because they are, among all major U.S. racial/ethnic groups, the most likely to hold jobs that require in-person work in close proximity to others (Dubay et al. 2020).
Yet even as they are at greater risk for exposure to the novel coronavirus, many Hispanics, especially immigrants, lack health insurance and face substantial barriers to vaccination, testing, and treatment (Capps and Gelatt 2020; Morales 2021). Preliminary data revealed large disparities in vaccination rates by race/ethnicity. As of February 23, 2021, NH whites accounted for 55.9 percent of all COVID-19 cases in the United States but composed 64.2 percent of all persons who had been vaccinated with one or more doses (CDC, n.d.). NH Blacks accounted for 12.2 percent of COVID cases and 6.4 percent of those vaccinated. Hispanics composed 20.8 percent of all cases but only 8.7 percent of persons who had been vaccinated (CDC, n.d.). State-level data underscored the magnitude of those disparities. As of February 16, 2021, in California, Hispanics accounted for 40 percent of the state’s total population, 55 percent of COVID-19 cases, and 16 percent of those vaccinated; in Florida, Hispanics composed 27 percent of the population, 37 percent of cases, and 16 percent of vaccinations (Ndugga et al. 2021).
The pandemic thus highlights the need to reduce barriers to health insurance and medical care for Hispanics through further expansions in private and public insurance coverage, the elimination of nonfinancial barriers to care, the creation of a more culturally responsive health care system, and investments in public health systems where funding has declined over the past decade (Maani and Galea 2020). The Biden administration, which came to office with narrow Democratic Party majorities in the House and Senate, has an opportunity to pursue policies that will improve access to health insurance and health care for Hispanic children.
Expand insurance coverage
Because health insurance is tied to employment, many American workers and their families lost health coverage when they lost their jobs during the COVID-related recession that started in April 2020. Although many of these jobs did not provide health insurance, preliminary work by the Urban Institute estimated that 3.3 million adults had lost ESI by mid-July 2020 (Gangopadhyaya, Karpman, and Aarons 2020). A subsequent analysis concluded that the number of adults with ESI declined by 5.5 million persons between March 2019 and April 2021 (Karpman and Zuckerman 2021). Hispanic households were hit particularly hard by the economic crisis precipitated by the pandemic, with nearly 24 percent of Hispanic adults (a much higher rate than for Black or white adults) reporting in September 2020 “that they or their spouse or partner lost or were laid off from a job since the beginning of March” (Karpman, Zuckerman, and Kenney 2020). Preliminary estimates were that 1.6 million Hispanic adults lost employer-sponsored health insurance between March and September 2020 (Gangopadhyaya, Karpman, and Aarons 2020). Among Hispanic adults who lost jobs or work-related income because of the pandemic, 28.5 percent reported an unmet medical need in their families due to cost (Gonzalez et al. 2020).
Because of the widespread erosion of ESI, analysts expected that the U.S. uninsured population would rise during 2020 (Gangopadhyaya, Karpman, and Aarons 2020). And given disproportionate job and income losses, we had reason to believe that the increase in the uninsured population would especially impact Hispanics, potentially including children. At this writing, we do not have data on changes in insurance coverage for Hispanic adults or children during 2020 and 2021. However, emerging data suggest, surprisingly, that among all Americans overall insurance coverage did not decline during 2020 (Karpman and Zuckerman 2021). That the uninsured population held steady despite large losses in ESI partly reflects the protective effects of the ACA, which provided a vital safety net that enabled many persons who lost job-based insurance to obtain coverage via Medicaid or through the Marketplace. In particular, large increases in Medicaid enrollment during this period countered the decline in ESI; in other words, while private coverage eroded, public insurance expanded, preventing a spike in the uninsured rate (Karpman and Zuckerman 2021).
Still, options for the newly uninsured were constrained in the states that had not expanded Medicaid eligibility under the ACA. In fact, the uninsured population increased during 2019 to 2021 in these states (Karpman and Zuckerman 2021). Since large Hispanic populations exist in some of those states, including Texas and Florida, the uninsured rate among Hispanics may have increased in some areas of the country.
While uncertainty remains regarding the pandemic’s effects on insurance coverage, what is certain is that substantial, ongoing gaps persist in insurance coverage for Hispanic children. Such gaps require expanding Hispanic children’s enrollment in public and private insurance plans. Given the strong associations between parental and child coverage, perhaps the most important opportunity to improve insurance coverage among Hispanic children is to expand Medicaid eligibility for adults in the states that have not done so. While Medicaid expansion remains a state decision, in March 2021 the Biden administration supported and Congress enacted a law (the American Rescue Plan Act, or ARPA) offering enhanced fiscal incentives to entice more states to expand. However, those incentives may not overcome partisan and ideological opposition in states that have not expanded Medicaid. At this writing, congressional Democrats are considering legislation that would enable low-income persons in states that have not expanded Medicaid to buy subsidized insurance coverage in the short term while creating a new federal Medicaid option to enroll them in the long term. Additionally, the 2021 ARPA increased the generosity of the subsidies for private insurance purchased in the ACA’s Marketplace. That will make coverage under the ACA more affordable, although further legislation will be required to make those changes permanent. In its first year, the Biden administration also boosted ACA enrollment outreach efforts and reversed Trump administration and state policies that linked Medicaid coverage for some enrollees to work requirements. Moving forward, it will be crucial for the Biden administration to lower state barriers to enrolling and reenrolling in Medicaid/CHIP, which could increase insurance coverage among Hispanic children.
Invest in public health systems
State and county health departments, together with FQHCs, are the backbones of our public health infrastructure (Perreira and Cofie 2016). They have been essential locations for no-cost COVID-19 testing across the United States and for contract tracing. To address racial/ethnic disparities in COVID-19 vaccination rates, they should also become essential locations for COVID-19 vaccinations. They are often located near areas where Hispanic families live; they are required to have translation and interpretation services available; and many have established trust with the Hispanic communities they serve. Although Congress passed a series of aid packages in 2020 that included increases in federal funding and grants for COVID-19 testing and treatment in community health centers (Capps and Gelatt 2020), additional funds will be needed for vaccination programs together with continued COVID-19 testing, contact tracing, and treatment.
Build trust and eliminate barriers to care
As with other forms of health care utilization, COVID-19 testing and vaccination among Hispanic children are likely to vary as a function of their parents’ perceived susceptibility to COVID-19 infection, perceived severity of the infections, perceived benefits of a COVID-19 vaccine, and perceived costs of the vaccine. Additionally, trust in their child’s health care provider is a critical determinant of parents’ vaccination decisions for their children (Gilkey et al. 2014). However, policies of exclusion and experiences with discrimination or unconscious bias can erode trust in health care providers, especially among mixed-status families, which include both U.S. citizens and noncitizens (Viruell-Fuentes, Miranda, and Abdulrahim 2012). These policies and experiences also increase the emotional cost of obtaining health care (Viruell-Fuentes, Miranda, and Abdulrahim 2012).
Initial studies of adults showed few racial/ethnic differences in COVID-19 vaccine hesitancy: about 26 percent of Hispanic, NH Black, and NH white adults reported that they would probably or definitely not get a COVID-19 vaccine (Kearney, Lopes, and Brodie 2021). Yet substantial racial/ethnic disparities in vaccination rates have nonetheless emerged (Ndugga et al. 2021), making it clear that barriers to vaccinations (not vaccine hesitancy) may be the primary factor explaining these disparities. While young children have yet to be included in COVID-19 vaccination programs, it will be essential to build trust and to reduce both financial and nonfinancial barriers to vaccinations to achieve high vaccination rates among both Hispanic adults and their children. Previous research (Crosnoe et al. 2012; Yoshikawa et al. 2014) suggests that community-based collaborations that promote health education and utilize community health workers to assist Hispanic populations with accessing health and human services can greatly facilitate vaccination efforts. Hispanic parents need to know that COVID-19 vaccinations are available at no cost, and health insurance is not required for vaccination. Hispanic parents also need to know that COVID-19 vaccinations are available to all residents of the United States regardless of their citizenship or immigration status; they will not be asked their citizenship or immigration status at vaccine clinics; and receipt of a free COVID-19 vaccine will not be considered in a public charge determination.
More generally, overhauling U.S. immigration policy could help to improve trust in providers and reduce barriers to medical care. The Biden administration’s reversal of the Trump administration’s public charge rule in March 2021 is a major step forward. Further actions by the Biden administration, including extending and making DACA (Deferred Action for Childhood Arrivals) permanent, offering a pathway to citizenship for unauthorized immigrants, and ending workplace raids, could reverse the chilling effects of the Trump administration’s restrictive policies and boost health insurance and health care access for Hispanic children.
Create a culturally responsive health care system
A culturally responsive health care system is also needed to help improve trust in health care providers and reduce nonfinancial barriers to care (Batista et al. 2018; Hussen et al. 2020). Building such a system requires investments in strategies to improve cultural responsiveness at both individual and systems levels. A culturally responsive workforce is better able to communicate with individuals from different backgrounds, understand different conceptions of health and illness, assist patients with the navigation of health systems, and address structural barriers to care (Hussen et al. 2020). Culturally responsive systems are designed to promote inclusivity through location and hours of operation, hiring and retention practices, ongoing training opportunities, multilingual signage, transportation services, and other policies and practices. Ultimately, these individual and system-wide efforts work together to facilitate health care utilization, improve patient satisfaction, and improve health outcomes (Batista et al. 2018; Hussen et al. 2020).
Conclusion
The Biden administration has an opportunity to leverage these strategies and improve access to health insurance and medical care for Hispanic children. In its first year, the administration has already started to make good on that opportunity by implementing policies to expand insurance coverage. Such policies could enhance Hispanic children’s access to health care. And by moving away from exclusionary immigration policies, the administration can create a less hostile environment for immigrants and reduce the fear that has contributed to an erosion of progress in health insurance coverage for Hispanic children. But barriers to meaningful change in health and immigration policies—from partisan polarization in Congress to divisions among the states and the influence of the courts—persist. It remains to be seen, then, whether the United States can in coming years restore progress in expanding Hispanic children’s access to health insurance and health care.
Footnotes
NOTE:
This research was supported by the Carolina Population Center (CPC) and its National Institutes of Health (NIH)/National Institute of Child Health and Human Development (NICHD) Grant Award Number P2C HD50924 as well as the Inclusive Science Program of the North Carolina Translational and Clinical Sciences (NCTraCS) Institute through Grant Award Number IL1TR002489 (Perreira).
Krista M. Perreira is a professor of social medicine at the University of North Carolina School of Medicine at Chapel Hill. Her scholarship combines qualitative and quantitative methodologies to study Hispanic/Latino health, immigration, and the consequences of structural inequalities and public policies affecting Hispanic/Latino and immigrant populations.
Chenoa D. Allen is an assistant professor of health sciences at the University of Missouri and a research affiliate at the University of Wisconsin Center for Demography of Health and Aging. Her current work studies the effects of state and local immigrant policies on Hispanic children’s health.
Jonathan Oberlander is a professor and chair of social medicine in the School of Medicine and a professor of health policy & management, Gillings School of Global Public Health, at the University of North Carolina at Chapel Hill. He is author of The Political Life of Medicare (University of Chicago Press 2003) and coeditor of The Social Medicine Reader.