
Abstract
This study identifies time-patterned trajectories of housing stability among homeless and vulnerably housed individuals who participated in a multisite four-year longitudinal study in Canada. Findings show four distinct trajectories for the homeless and vulnerably housed: high levels of sustained housing stability, improving levels over time leading to high levels of housing stability, decreasing levels of housing stability over time, and low levels of housing stability over time. The presence of resources rather than risk factors differentiated the trajectories of participants who achieved housing stability from those who had low levels of housing stability. Participants who had better housing stability were more likely to live in subsidized housing. Findings highlight the need for programs and policies directed at addressing the housing affordability problem through income support strategies and the creation of affordable housing.
Homelessness is a significant and visible social problem in Western industrial countries (Abbé Pierre Foundation & FEANSTA 2018; The Council of Economic Advisers 2019; Employment and Social Development Canada 2019). Over the past three decades, the homeless population has become increasingly heterogeneous and includes youth, single adults, and families with young children. Moreover, a multitude of economic, social, health, and personal factors have contributed to people becoming homeless and impeded their ability to becoming housed again and successfully exit homelessness (Gaetz 2010; Thompson et al. 2010; Tsai and Rosenheck 2015). As a result of this heterogeneity, research identifying subgroups of individuals and families who are homeless has played a major role in guiding policies intended to address homelessness in the United States, Canada, and Europe (Aubry et al. 2013; Benjaminsen and Andrade 2015; Culhane et al. 2007; Daly, Craig, and O’Sullivan 2018; Kuhn and Culhane 1998; Rabinovich, Pauly, and Zhao 2016).
Kuhn and Culhane (1998) conducted a seminal study using cluster analysis to identify subgroups of single adults based on length of homelessness and number of episodes of homelessness over several years in New York City and Philadelphia. They found three distinct groups that were termed “transitional,” “episodic,” and “chronic.” The majority of individuals were in the transitional group and were people who stayed in shelters for short periods of time and most often had one stay. The episodic group cycled in and out of shelters while staying for relatively short periods. Finally, the chronic group had the longest shelter stays. Kuhn and Culhane also found episodic and chronic shelter users more likely to have physical and mental health problems and substance use histories compared to the transitional group. As a result, these two groups have been prioritized for receiving more intensive and longer-term support to exit homelessness in the United States, Canada, and many European countries through programs such as Housing First, which facilitates rapid access to housing through the provision of a rent supplement combined with individualized community support (Aubry et al. 2013; Benjaminsen and Andrade 2015; Brown et al. 2017).
Recent Research on the Trajectories of Homelessness
Although this line of research has been impactful in shaping homelessness policies in numerous countries, its utility has been critiqued for using a time-aggregated approach, namely, conducting cluster analyses based on the cumulative time that homeless people were in shelters and the number of discrete episodes in which they experienced homelessness. Because of these limitations, researchers have argued that the results fail to capture the more complex heterogeneity associated with different patterns of being housed or homeless over time (Brown et al. 2017; McAllister, Lennon, and Kuang 2011). Using the same shelter data as Kuhn and Culhane (1998), McAllister, Lennon, and Kuang (2011) conducted a time-patterned approach that resulted in a typology of ten groups that demonstrated different patterns of entering and leaving shelters. They argued that this more fine-grained analysis served to further differentiate individuals and determine their specific needs relative to services and policies.
To date, a small number of studies have conducted analyses based on a time-patterned approach. In the earliest study, Lennon and her colleagues (2005) examined homelessness status on a monthly basis over an 18-month period using latent class growth analysis (LCGA) to identify different trajectories of ninety-six men with mental illness who were homeless and participating in a randomized controlled trial (RCT) of critical time intervention (CTI) involving short-term practical and psychosocial support assisting people to move into housing. They found four latent classes in the control group and three in the CTI group. They did not examine any predictors, and the small study sample produced classes with a small number of men.
Tevendale, Comulada, and Lightfoot (2011) also used LCGA to identify different trajectories of 426 youth and young adults living initially in a setting indicative of homelessness such as on the street, in an abandoned building, in an emergency shelter, or temporarily in a motel or hotel. The study followed participants for two years with longitudinal analyses examining their living situation over three-month periods. Three trajectories emerged from their analyses that included being consistently sheltered, unsheltered for a short amount of time, and unsheltered over a long term. They found younger age, not using drugs other than alcohol or marijuana, less involvement in illegal activity to support oneself, being able to go home, and having been homeless for less than one year associated with the consistently sheltered group relative to the long-term inconsistently unsheltered group.
Adair and her colleagues (2017) used multigroup, multilevel growth mixture modeling (GMM) to identify trajectories based on housing stability over 6-month periods and predictors of these trajectories for 2,140 participants in a multicity 24-month RCT comparing persons with serious mental illness with a history of homelessness receiving Housing First to individuals receiving treatment as usual. They identified six trajectories that included one class of individuals housed rapidly that was sustained, another class not housed at all, a class with more gradual gains that were sustained, a class that diverged by treatment arm (Housing First participants improved their prestudy housing stability, while treatment as usual experienced a loss of their prestudy housing stability), another with early housing that was lost, and a class with rapid housing followed by a steep decline in stable housing. Only a small number of predictors of trajectories proved to be significant, with the class of individuals not housed at all serving as the reference group. Male gender, Indigenous ethno-cultural status, longer lifetime length of homelessness, and a greater number of previous hospitalizations were found to be associated with the trajectories showing poorer housing stability outcomes.
Using McAllister, Lennon, and Kuang’s (2011) typology as a guide, Brown and her colleagues (2017) developed a time-patterned typology for a sample of 246 individuals with mental illness using administrative data and based on episodes of homelessness over a four-year period. They identified four groups comprising individuals who were continuously homeless, individuals who were continuously housed after a very short period of homelessness, individuals who were intermittently homeless, and individuals who were temporarily homeless but housed at follow-up. Being male was predictive of being continuously homeless relative to the other groups. Other predictors of being intermittently housed or temporarily housed compared to being continuously homeless that emerged as significant included having a psychotic disorder. Individuals with substance use problems were more likely to be in the intermittently housed group compared to the continuously homeless group.
Most recently, Chu and her colleagues (2020) used LCGA to identify trajectories of shelter use over a 24-month period from the same Canadian multicity trial as Adair et al.’s (2017) study on trajectories of housing stability. The study identified four trajectories made up of consistently low shelter use, mostly low with increased shelter use near the end of the study, early shelter use followed by decline to low shelter use, and high shelter use peaking after the study midpoint and then declining to low use. Older age and having a longer history of homelessness were significant predictors of greater shelter use.
As this research shows, trajectories as they relate to changes in housing status are a promising area of study that can yield findings that are policy relevant (also see the articles by Richter et al., this volume; Lachaud et al., this volume). The findings of these studies typically identify four to six trajectories that include patterns of continuous housing and continuous homelessness as well as a mixture of housing and homelessness that suggest either positive or negative outcomes over time. Differences in trajectories lend themselves to identifying predictors of successful exiting of homelessness.
However, the research conducted to date has a number of limitations, including the size and nonrepresentativeness of samples (Brown et al. 2017; Lennon et al. 2005; Tevendale, Comulada, and Lightfoot 2011), short length of follow-up (Adair et al. 2017; Chu et al. 2020; Tevendale, Comulada, and Lightfoot 2011), location in single cities (Brown et al. 2017; Gleason, Barile, and Baker 2017; Lennon et al. 2005; Tevendale, Comulada, and Lightfoot 2011), focus on specific populations (Adair et al. 2017; Brown et al. 2017; Chu et al. 2020; Lennon et al. 2005; Tevendale, Comulada, and Lightfoot 2011), and limited examination of predictors (Brown et al. 2017; Lennon et al. 2005). Research in this area is also largely atheoretical.
The Current Study
The Health and Housing in Transition (HHiT) study provides an opportunity to address the limitations of research to date and extend the knowledge about the housing trajectories among single adults with a history of homelessness. The HHiT was a prospective cohort panel study that surveyed longitudinally the health and housing status of homeless and vulnerably housed individuals in three Canadian cities. Using a resilience perspective, this study is intended to identify the different trajectories and predictors of these trajectories among individuals who are either homeless or vulnerably housed at study entry.
Research has defined resilience as the achievement of positive outcomes in response to significant adversity such as homelessness (Masten 2001). A combination of risk factors and resources contribute to an individual’s response to adversity. We expected risk factors related to physical health functioning, mental health functioning, and substance use to play a role in achieving enduring housing stability. We predicted that lower levels of physical health functioning and mental health functioning and higher levels of drug use and alcohol consumption would be related to a lower likelihood of achieving sustained housing stability.
For the study, we applied an ecological model to test resources at the individual, interpersonal, and community levels. We predicted that greater access to resources would be related to achieving more positive trajectories of housing stability. Individual resources referred to an individual’s capital that would facilitate becoming and staying housed. In the study, these resources were level of educational attainment and income. Interpersonal resources were defined as assistance available through social relationships and consisted of perceived availability of social support and involvement in an intimate relationship. Community resources referred to economic assistance and environmental factors that would contribute to housing stability, such as access to subsidized housing, perceived quality of housing, and perceived quality of neighborhood.
Methods
Study setting
A detailed description of the methods, including the measures, is available in the published protocol paper (Hwang et al. 2011). Data for the analysis originate from the HHiT study, a prospective cohort panel study that examined the health and housing status of a representative sample of homeless and vulnerably housed single adults in three Canadian cities (Toronto, Ottawa, and Vancouver) between 2009 and 2013. The locations are all large urban cities that vary in terms of geographic location, population size, and housing markets.
At the beginning of the HHiT study in 2009, social assistance rates ranged in the three cities between $585 and $610 CDN per month for a single adult and between $906 and $1,053 CDN per month for a single adult with a disability (Hwang et al. 2011). Average monthly rents for a private one-bedroom apartment in these three cities ranged from $853 to $926 CDN, while vacancy rates ranged from 1.4 to 3.0 percent (Hwang et al. 2011). Given the gap between income and market rents, marginalized individuals living on these fixed incomes typically exit homelessness to single-room-occupancy (SRO) hotels in Vancouver and rooming houses in Toronto and Ottawa.
Participants
We recruited homeless and vulnerably housed persons aged 18 or older who were single (i.e., not living with a partner or dependent child) in Ottawa, Toronto, and Vancouver from January to December 2009. We defined homelessness as living within the last seven days in a shelter, public space, vehicle, abandoned building, or someone else’s home; and not having a home of one’s own. Vulnerably housed was defined as currently living in one’s own room or apartment but having been homeless or have had two or more moves in the past 12 months. We excluded full-time students and individuals who were visiting the city for three months or less.
Recruitment
We targeted a sample of six hundred single individuals who were homeless and six hundred individuals who were vulnerably housed (i.e., two hundred per group in each of the three cities). The sampling procedure for recruiting participants who were homeless used the design that Ardilly and Le Blanc (2001) suggested. We recruited study participants at homeless shelters and meal programs. We randomly selected participants recruited in shelters. Homeless participants who did not use shelters were recruited at meal programs proportionally to the estimated number of homeless persons who slept on the street in each respective city.
Vulnerably housed participants were recruited from randomly selected rooming houses in Ottawa and Toronto and from SRO hotels in Vancouver. Due to difficulties in gaining access to some of these locations, we modified the recruitment strategy for vulnerably housed individuals to include meal programs, drop-in centers, and community health centers. As a result of a small number of participants completing more than one interview, the final sample was 1,192 individuals.
Follow-up procedures
Participants were reinterviewed every 12 months over the four-year period of the study. We made efforts to develop a positive rapport with participants, emphasizing the importance of their participation in follow-up interviews. At the first interview, we asked participants to provide contact information not only for themselves but also for friends, relatives, service providers, and case workers who were most likely to know their future whereabouts and who could be contacted to locate them. We also asked participants to give consent for municipal social services departments, hospitals, homeless shelters, prisons, and treatment centers to disclose their updated contact information to the research team.
To increase the quality of the estimation for the trajectory analysis (having four measurements of the tracked housing history), we used the available sample for the four-year period from baseline to the fourth follow-up. For the current study, we calculated the percentage of days (0–100 percent) that participants spent in stable housing (i.e., permanent housing on which rent was paid and individuals had tenant rights) at six-month intervals.
Survey protocol
Study staff conducted in-person interviews with participants at study entry and at each of the annual follow-up contacts. Interviews took approximately 60 to 90 minutes to complete. The survey instrument was made up of validated measures and questions that we selected on the basis of their relevance and previous successful use among homeless and vulnerably housed people, having very good to excellent psychometric properties, being sensitive to change over time, and being easy to administer. We collected housing history over the past year at each follow-up using the Housing Timeline Follow-Back Calendar (HTFBC), a validated method that allows for the collection of detailed and accurate information on housing history (Tsemberis et al. 2007). Data from this measure provided a day-by-day account of the housing history of participants over the four-year period of the study.
Demographic characteristics included gender, age, ethnicity/race, and city. Risk factors, as reported by participants at baseline, were mental health (12-Item Short Form Survey [SF-12]; Ware, Keller, and Kosinski 1995), number of chronic physical health conditions (Burt et al. 1999), alcohol use (Alcohol Use Disorders Identification Test [AUDIT]; Babor et al. 2001), drug use (Drug Abuse Screening Test [DAST]-10; Gavin, Ross, and Skinner 1989), and lifetime history of homelessness before entering the study (i.e., cumulative days of homelessness) and reporting an unmet need for health care in the past year.
Individual resources were level of education reported at baseline, monthly income at the first follow-up interview, and employment status in last 12 months reported at the first follow-up. Interpersonal resources were relationship status (i.e., involvement or not in an intimate relationship) and perceived availability of social support indicated at the first follow-up interview (Social Provisions Scale; Cutrona and Russell 1987). Community resources were perceived housing quality (Housing Quality Score; Toro et al. 1995), and satisfaction with neighborhood reported at the first follow-up (Quality of Life for Homeless and Hard-to-House Individuals; Hubley et al. 2009). We accounted for living in subsidized housing with a dichotomous variable of either no report of subsidized housing or indication of living in subsidized housing at one or more of the four follow-up interviews.
Data analyses
We kept participants with data on at least three measures of six-month periods of percentage of days stably housed over the course of study for the analyses. Our study included a total of 1,066 participants in the trajectory modeling, representing 90 percent of the HHiT study sample. A breakdown of the sample by housing status at study entry found 522 participants in the homeless group and 544 participants in the vulnerably housed group. We used group-based trajectory modeling (GBTM; Nagin 1999; Nagin and Ogders 2010) with each of these two groups to identify groups of participants who followed distinct trajectory patterns of the percentage of days spent stably housed in six-month periods over four years. We performed the trajectory model analyses with the group-based trajectory statistical program called “traj” (Jones and Nagin 2012) in Stata software (version 16). Further details of the GBTM analyses are provided in the online appendix.
To investigate demographic characteristics, risk factors, and resources associated with subgroups that have distinctive trajectory patterns for each of the groups, we conducted a multinomial logistic regression (MLR) with demographic characteristics entered in the first model, risk factors after controlling for demographic characteristics in the second model, and resources after controlling for demographic characteristics and risk factors in the third model. Demographic characteristics of gender, age, ethnicity/race, and participant’s residential city at study entry served as both predictors and adjustment variables.
Baseline scores on health status measures (i.e., number of chronic illnesses and physical and mental health functioning), substance use measures, and whether participants had unmet needs for health care were entered as risk factors. Level of education at baseline, income and employment in the past year, perceived social support, perceived quality of housing, and satisfaction with the neighborhood, reported at the first follow-up interview, were entered as resources. In addition, we entered a dichotomous measure of access to subsidized housing (i.e., no subsidy vs. access to subsidy at any time over the course of the study) as resources. The analyses estimated the relative risk ratio (RRR) and we performed them at a 95 percent statistical confidence level using Stata software.
The steps that we undertook to estimate missing data for predictor variables in the MLR are also presented in the online appendix. The study removed a small number of participants with missing data for the ethnicity variable as well as transgendered individuals. We included a final sample of 1,020 participants in the MLR analyses.
Results
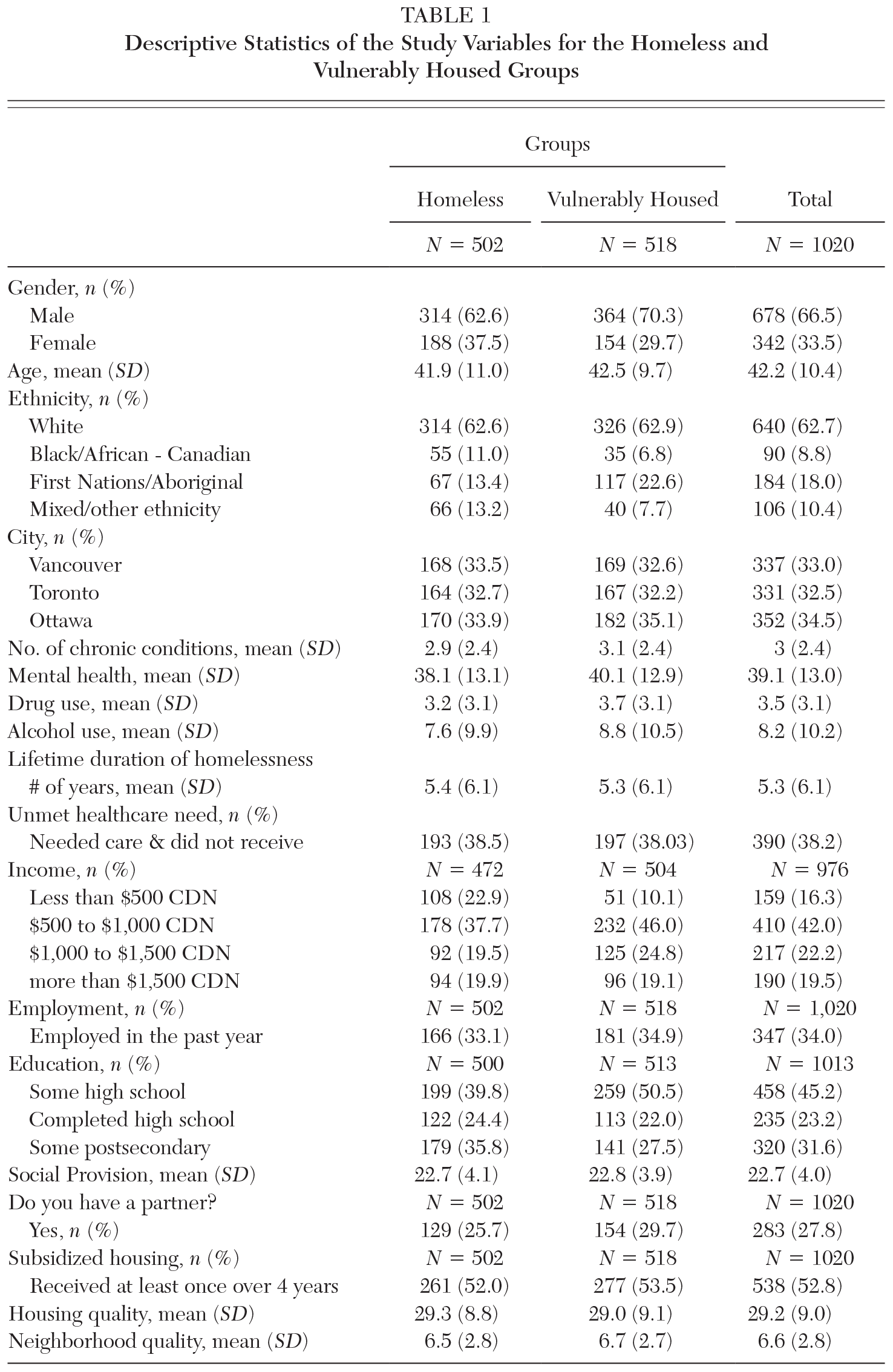
Table 1 presents the demographic characteristics, risk factors, and resources for the homeless and vulnerably housed groups.
Descriptive Statistics of the Study Variables for the Homeless and Vulnerably Housed Groups
Homeless group
As panel A of Figure 1 shows, there were four distinct housing trajectories in the homeless group (a model comprising one trajectory group with a quadratic polynomial shape followed by three trajectory groups with cubic polynomial shape): class 1, low to moderate housing stability (N = 84, 16 percent); class 2, low to high housing stability (N = 104; 20 percent); class 3, moderate rise followed by a fall in housing stability (N = 90; 17 percent); and class 4, moderate to high sustained housing stability (N = 244; 47 percent).
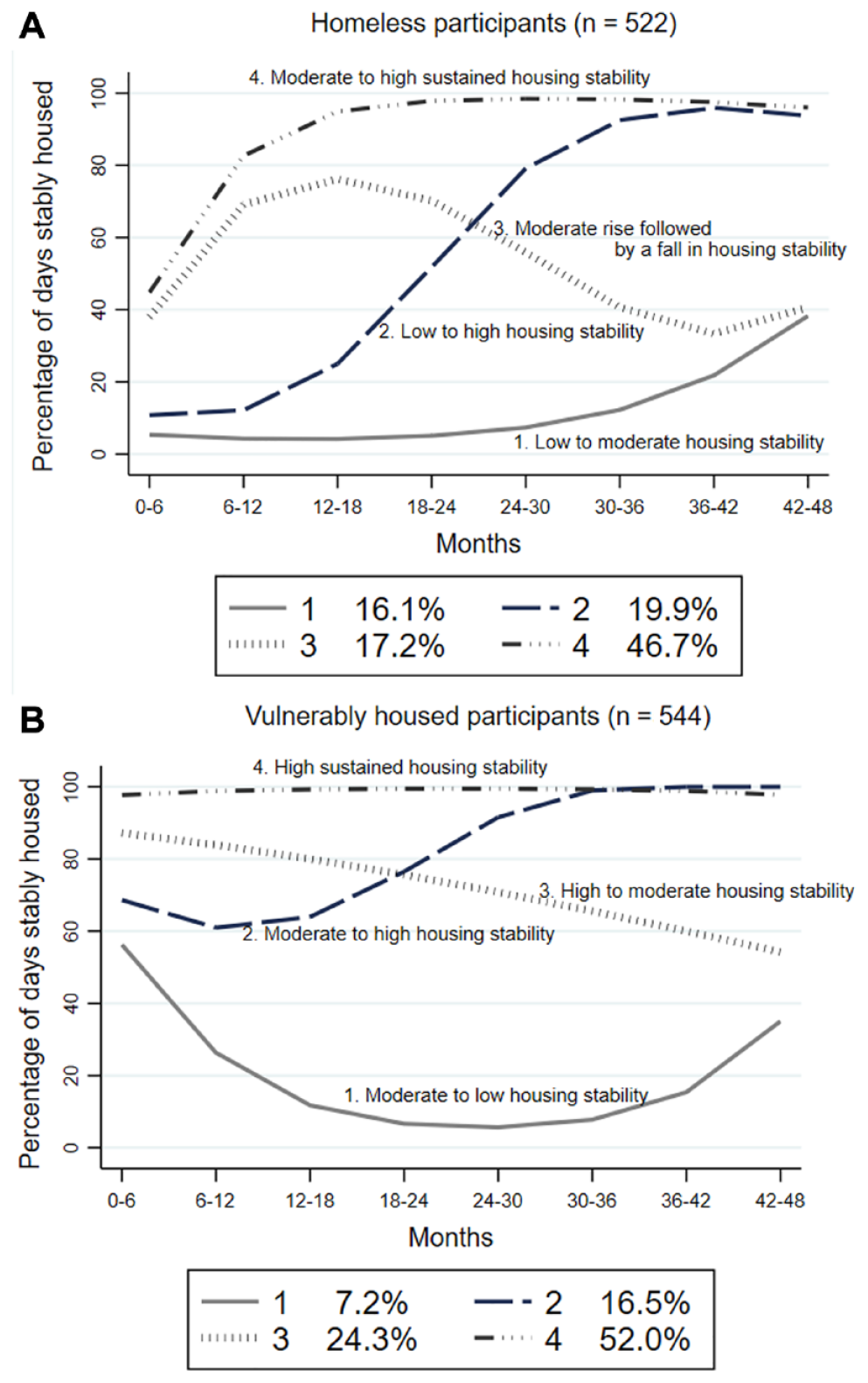
Housing Stability Trajectories for Homeless and Vulnerably Housed Groups
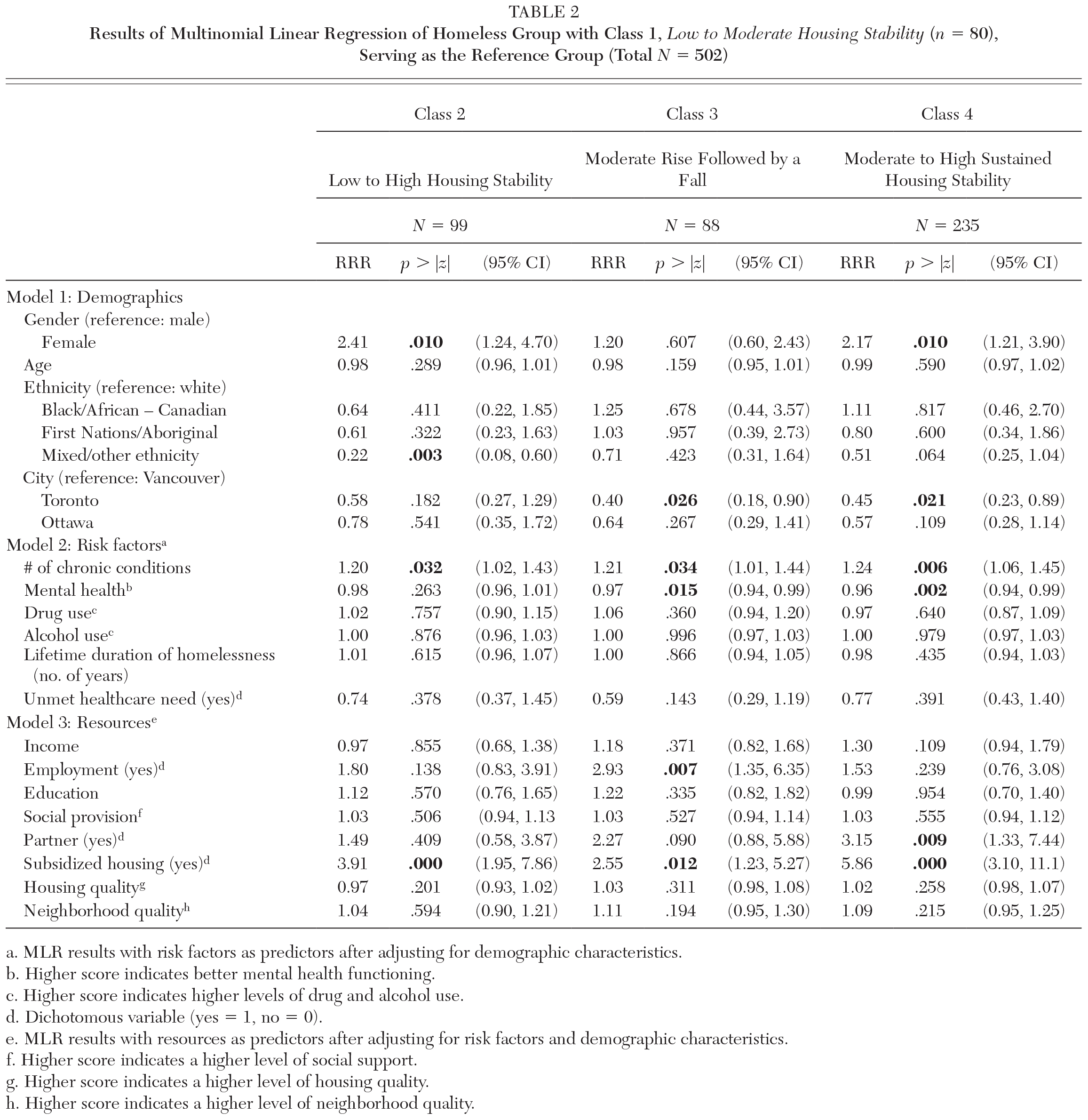
Table 2 presents the results of the three models that the MLRs produced with the moderate to low housing stability trajectory class serving as the reference group. All three models are significant. Further details of the MLR results are presented in the online appendix, including supplementary tables of descriptive statistics of study variables for each of the classes.
Results of Multinomial Linear Regression of Homeless Group with Class 1, Low to Moderate Housing Stability (n = 80), Serving as the Reference Group (Total N = 502)
MLR results with risk factors as predictors after adjusting for demographic characteristics.
Higher score indicates better mental health functioning.
Higher score indicates higher levels of drug and alcohol use.
Dichotomous variable (yes = 1, no = 0).
MLR results with resources as predictors after adjusting for risk factors and demographic characteristics.
Higher score indicates a higher level of social support.
Higher score indicates a higher level of housing quality.
Higher score indicates a higher level of neighborhood quality.
Relative to the reference group, class 2, low to high housing stability, participants were less likely to have a mixed ethnic background (RRR = 0.22, 95 percent confidence interval [CI] = 0.08, 0.60) and more likely to be female (RRR = 2.41, CI = 1.24, 4.70), report a higher number of chronic conditions (RRR = 1.20, CI = 1.02, 1.43), and have accessed subsidized housing during the study (RRR = 3.91; CI = 1.95, 7.86). In comparison to the reference group, class 3, moderate rise followed by a fall in housing stability, participants were less likely to live in Toronto (RRR = 0.40; CI = 0.18, 0.90) and more likely to report a higher number of chronic health conditions (RRR = 1.21; CI = 1.01, 1.44), indicate lower mental health functioning at study entry (RRR = 0.97, CI = 0.94, 0.99), be employed at the first follow-up (RRR = 2.93, CI = 1.35, 6.35), and have had access to subsidized housing (RRR = 2.55, CI = 1.23, 5.27). Compared to the reference group, class 4, moderate to high sustained housing stability, participants were less likely to live in Toronto (RRR = 0.45, CI = 0.23, 0.89) and more likely to be female (RRR = 2.17, CI = 1.21, 3.90), report more chronic health conditions (RRR = 1.24, CI = 1.06, 1.45), indicate a lower level of mental health functioning (RRR = 0.96; CI = 0.94, 0.99), be in an intimate relationship at study entry (RRR = 3.15, CI = 1.33, 7.44), and have accessed subsidized housing during the study (RRR = 5.86; CI = 3.10, 11.10).
Vulnerably housed group
As panel B of Figure 1 shows, there were also four distinct housing trajectories in the vulnerably housed group (a model comprising three trajectory groups with quadratic polynomial shapes): class 1, moderate to low housing stability (N = 39; 7 percent); class 2, moderate to high housing stability (N = 90; 17 percent); class 3, high to moderate housing stability (N = 132; 24 percent); and class 4, high sustained housing stability (N = 283; 52 percent).
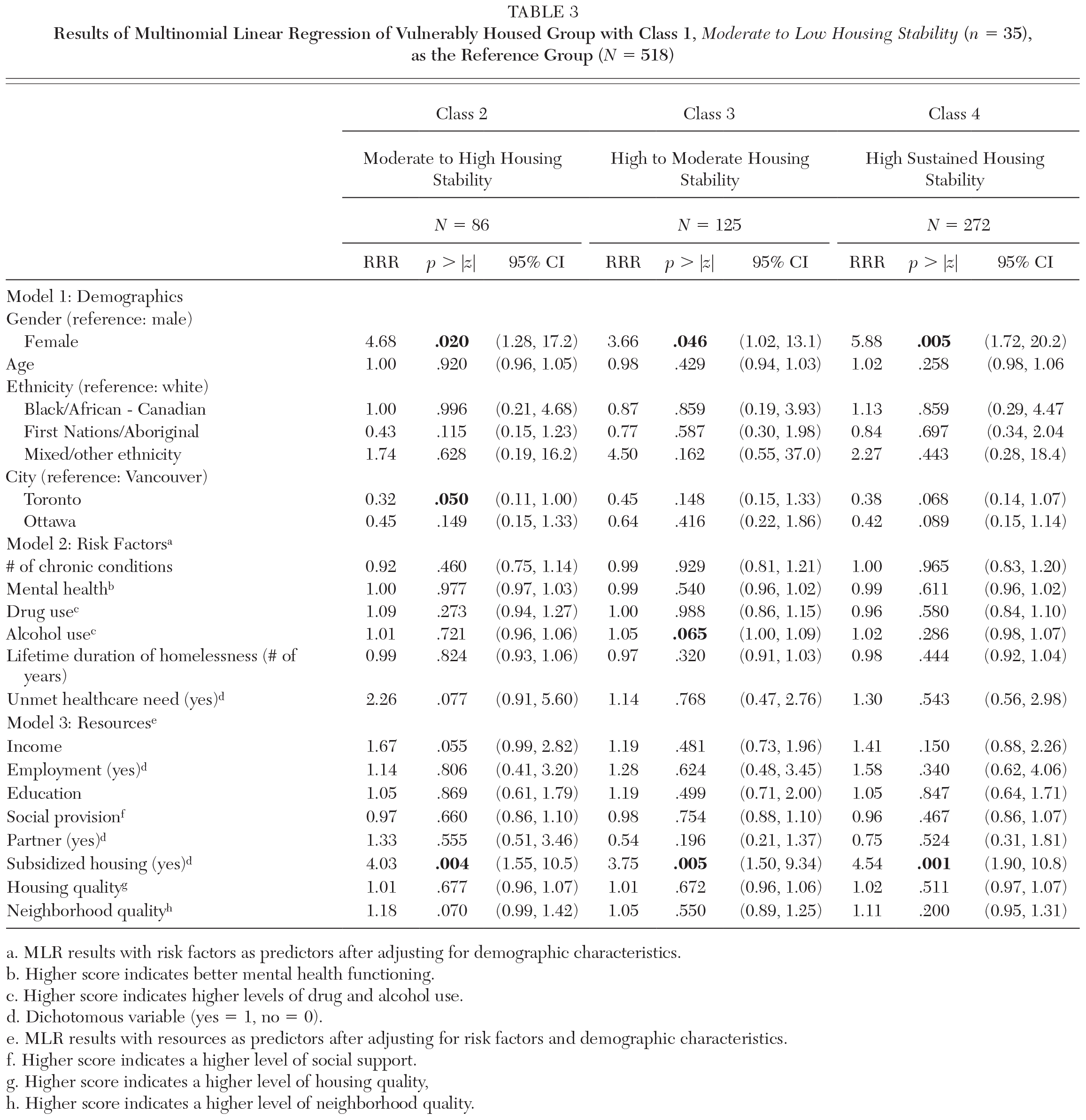
Table 3 presents the results of the three models that the MLRs produced with the moderate to low housing stability trajectory class serving as the reference group. All three models are significant. Additional information about the MLR results for the vulnerably housed group are presented in the online appendix, including supplementary tables of descriptive statistics of study variables for each of the classes.
Results of Multinomial Linear Regression of Vulnerably Housed Group with Class 1, Moderate to Low Housing Stability (n = 35), as the Reference Group (N = 518)
MLR results with risk factors as predictors after adjusting for demographic characteristics.
Higher score indicates better mental health functioning.
Higher score indicates higher levels of drug and alcohol use.
Dichotomous variable (yes = 1, no = 0).
MLR results with resources as predictors after adjusting for risk factors and demographic characteristics.
Higher score indicates a higher level of social support.
Higher score indicates a higher level of housing quality.
Higher score indicates a higher level of neighborhood quality.
Compared to the reference group, class 2, moderate to high housing stability, participants were less likely to live in Toronto (RRR = 0.32; CI = 0.11, 1.00) and more likely to be female (RRR = 4.68; CI = 1.28, 17.20) and have accessed subsidized housing during the study (RRR = 4.03; CI = 1.55, 17.20). Relative to the reference group, class 3, high to moderate housing stability, participants were also more likely to be female (RRR = 3.66; CI = 1.02, 13.10) and have accessed subsidized housing (RRR = 3.75; CI = 1.50, 9.34). Similarly, class 4, high sustained housing stability, participants were more likely to be female (RRR = 5.88; CI = 1.72, 202.20) and to have lived in subsidized housing over the four-year period (RRR = 4.54; CI = 1.90, 10.80).
Discussion
Our study identified trajectories of housing stability for a group of single adults who were homeless and for a group of single adults who were vulnerably housed living in three large Canadian cities over a four-year period. Based on a resilience model, we examined differences in demographic characteristics, risk factors, and resources among individuals with different housing trajectories, using the most negative trajectory (low to moderate or moderate to low housing stability) as the reference group. Using an ecological perspective, we conceptualized resources at three different levels—individual, interpersonal, and community.
The pattern of trajectories emerging from our analyses proved to be similar to previous research on trajectories of housing stability. In particular, previous studies have found (1) trajectories of consistently low housing stability and consistently high housing stability over time (Adair et al. 2017; Brown et al. 2017; Tevendale, Comulada, and Lightfoot 2011) and (2) trajectories with delayed outcomes, either among individuals who establish housing stability over time or among individuals who show diminished housing stability after having achieved early housing stability (Adair et al. 2017; Brown et al. 2017; Tevendale, Comulada, and Lightfoot 2011).
Interestingly, our findings regarding the trajectories of individuals in the two groups with the lowest proportion of time in stable housing showed improvements over the last 18 months of the study. As well, the trajectories of people in these two groups who showed negative outcomes over time did not show a complete loss of housing stability. An examination of the positive trajectories in the two groups (improving high housing stability over time [class 2] and high sustained housing stability [class 4]) indicate that about two-thirds of the sample in each group (i.e., homeless group [67 percent]; vulnerably housed group [69 percent]) achieve sustained housing stability by the end of the four-year period of the study.
Among demographic characteristics, differences on gender emerge between most of the classes and the reference group for both the homeless and vulnerably housed groups. Individuals in the reference groups showing the lowest housing stability are more likely to be men in comparison to all of the other trajectory classes with the exception of the moderate rise followed by the fall in housing stability participants in the homeless group. The RRR of these differences ranged from 2.17 to 5.88, suggesting a reasonably large association. These findings are similar to previous research that showed women being disproportionately represented in trajectories showing successful sustained exits from homelessness (Adair et al. 2017; Brown et al. 2017). Likewise, previous cluster analysis research has shown men to be overrepresented in episodic and chronic clusters in Ottawa and Toronto (Aubry et al. 2013).
Only two predictors showed associations between trajectory classes and the reference group for homeless participants at study entry. Specifically, individuals in all of the trajectory classes of the homeless group reported a higher number of chronic health conditions than individuals with a low housing stability trajectory. These findings appear counterintuitive and are at odds with our hypothesis regarding risk factors. It is possible that prioritization of individuals with chronic physical health problems for housing plays a role in these differences. Another plausible explanation is that individuals with chronic health conditions receive social benefits that are higher than the public assistance for those without disabilities. For vulnerably housed participants, no risk factors differentiated the reference group from the other trajectory groups.
Mental health functioning also showed a significant association between two trajectory classes (i.e., moderate rise followed by a fall in housing stability and moderate to high sustained housing stability) and the reference group among homeless participants. However, again the association was in the opposite direction of our hypothesis with the low to moderate housing stability class reporting a higher level of mental health functioning than these two trajectory classes in the homeless group. The association is very small in nature (RRR 0.96 and 0.97). It is also important to highlight our finding that level of substance use was not predictive of trajectory class. Overall, our results suggest that risk factors other than chronic physical health conditions play an inconsequential role in determining the trajectory classes.
Subsidized housing shows an association between all trajectory groups and the reference groups for both homeless and vulnerably housed participants in line with our hypothesis that having greater resources will be related to more positive housing trajectory outcomes. The finding is consistent with extensive previous observational and intervention research that shows rental subsidies as a critical resource to leaving homelessness (Aubry et al. 2016; Gubits et al. 2018; Pankratz, Nelson, and Morrison 2017; Zlotnick, Robertson, and Lahiff 1999).
Research has well established that individuals who are homeless live in extreme poverty and this poverty is the major driver behind their homelessness (Shinn 2010; Shinn and Khadduri 2020). Poverty combined with a shrinking affordable housing market in major Canadian cities have contributed to the growth in number of people who experience homelessness over the past three decades (Gaetz 2010). Our findings, which show the important association of an economic resource like housing subsidies in trajectories leading to housing stability combined with the lack of association of risk factors, support the notion that homelessness is foremost a poverty problem that needs to be targeted to ultimately end homelessness.
Our study has a number of strengths that include the longitudinal design in which we followed participants over four years, the collection of data in three cities, the large sample size, the inclusion of homeless and vulnerably housed populations, the study’s tracking of homelessness beyond simply shelter use, the high retention rate, and the use of validated measures with a history of successful use with this population.
The study also has a number of limitations, notably the lack of sampling of homeless individuals who do not use shelters, drop-in centers, or meal programs and difficulties encountered in the sampling of vulnerably housed individuals, risking some sampling biases toward less marginalized individuals. At the same time, that the sampling strategy did not select people who were newly homeless led to participants more likely to have chronic histories of homelessness. This chronic history may have restricted the range of the severity of risk factors and limited the utility of interpersonal resources for them. We were not able to confirm the housing status of individuals recruited at drop-in centers and meal programs. Finally, the reliance on self-report measures can result in underreporting of health problems and substance use.
Nevertheless, our findings underline the critical importance that economic resources play in assisting individuals in achieving housing stability. Assisting individuals with rent subsidies either through rent supplements for use in the private rental market or through lowered rents in public housing have been found in numerous studies to be associated with ending homelessness (Aubry et al. 2016; Gubits et al. 2018; Pankratz, Nelson, and Morrison 2017; Stojanovic et al. 1999; Zlotnick, Robertson, and Lahiff 1999). Almost 80 percent of our study participants had incomes lower than $1,500 CDN per month. Rent for housing for single individuals in Canadian cities has required a disproportionate amount of income tied to social benefit programs over the past two decades (Gaetz 2010).
Ultimately, our study provides further evidence that homelessness is an economic problem requiring interventions targeting the “housing affordability problem” that the segment of the population living in extreme poverty face. The required policy response needs to address this affordability problem to end homelessness. The problem can be addressed through a variety of strategies that include raising income support, significantly increasing the availability of rent supplements, and developing affordable private market and social housing (Shinn and Khadduri 2020). These solutions can be combined with support when needed through evidence-based interventions, such as Critical Time Intervention and Housing First (Padgett, Henwood, and Tsemberis 2016). Program and policy interventions exist to end homelessness, but they need to be implemented at a scale that matches the size of the problem.
Supplemental Material
sj-docx-1-ann-10.1177_0002716220987203 – Supplemental material for Housing Trajectories, Risk Factors, and Resources among Individuals Who Are Homeless or Precariously Housed
Supplemental material, sj-docx-1-ann-10.1177_0002716220987203 for Housing Trajectories, Risk Factors, and Resources among Individuals Who Are Homeless or Precariously Housed by Barrett A. Lee, Marybeth Shinn, Dennis P. Culhane, Tim Aubry, Ayda Agha, Cilia Mejia-Lancheros, James Lachaud, Ri Wang, Rosane Nisenbaum, Anita Palepu and Stephen W. Hwang in The ANNALS of the American Academy of Political and Social Science
Footnotes
Note: This project was supported by an operating grant (MOP-86765) and an Interdisciplinary Capacity Enhancement Grant on Homelessness, Housing and Health (HOA-80066) from the Canadian Institutes of Health Research. The MAP Centre for Research on Urban Solutions at St. Michael’s Hospital gratefully acknowledges the support of the Ontario Ministry of Health and Long-Term Care. The authors thank Ying Di for her expert programming and analyses. We would like to acknowledge the following individuals from our community partner organizations: Laura Cowan, Liz Evans, Sarah Evans, Stephanie Gee, Clare Haskel, Erika Khandor, and Wendy Muckle. The authors also thank the shelter, drop-in, and municipal and provincial staff for their assistance with participant recruitment and follow-up.
Tim Aubry is a full professor in the School of Psychology and a senior researcher at the Centre for Research on Educational and Community Services at the University of Ottawa.
Ayda Agha is a community health researcher working at the Centre for Research on Educational and Community Services at the University of Ottawa. She is currently a doctoral student in the School of Psychology at the University of Ottawa.
Cilia Mejia-Lancheros is a public health researcher and social epidemiologist working as a postdoctoral research fellow at MAP Centre for Urban Health Solutions, St. Michael’s Hospital in Toronto.
James Lachaud is a demographer with research interests in population and public health. He is currently a postdoctoral research fellow at MAP Centre for Urban Health Solutions, St. Michael’s Hospital in Toronto, and holds a CIHR-IPPH/CMHC fellowship award in research and knowledge translation on urban housing and health.
Ri Wang is a statistician working at MAP Centre for Urban Health Solutions, St. Michael’s Hospital in Toronto.
Rosane Nisenbaum is a biostatistician and associate scientist with MAP Centre for Urban Health Solutions and the Applied Health Research Centre in the Li Ka Shing Knowledge Institute of St. Michael’s Hospital and an assistant professor in the University of Toronto’s Division of Biostatistics at the Dalla Lana School of Public Health.
Anita Palepu is a professor of medicine, general internal medicine at the University of British Columbia (UBC). She is the Eric W. Hamber Chair and head of the Department of Medicine at UBC and Providence Health Care in Vancouver.
Stephen W. Hwang is a professor of medicine at the University of Toronto and general internist at St. Michael’s Hospital in Toronto. He is the director of MAP Centre for Urban Health Solutions and holds the Chair in Homelessness, Housing, and Health at the University of Toronto and St. Michael’s Hospital.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.