
Abstract
Individuals deeply socialized into professional cultures tend to strongly resist breaking from their professions’ core cultural tenets. When these individuals face external pressure (e.g., via new technology or regulation), they typically turn to peers for guidance in such involuntary reinventions of their work. But it is unclear how some professionals may voluntarily break from deeply ingrained views. Through our study of French anesthesiologists who practice hypnosis, we aim to better understand this little-explored phenomenon. Adopting hypnosis, a technique that many anesthesiologists consider subjective and even magical, contradicted a core tenet of their profession: the need to only use techniques validated by rigorous scientific-based research. Drawing on interviews and observations, we analyze how these anesthesiologists were able to change their views and reinvent their work. We find that turning inward to oneself (focusing on their own direct experiences of clients) and turning outward to clients (relying on relations with clients) played critical roles in anesthesiologists’ ability to shift their views and adopt hypnosis. Through this process, these anesthesiologists embarked on a voluntary internal transformation, or reboot, whereby they profoundly reassessed their work, onboarded people in adjacent professions to accept their own reinvention, and countered isolation from their peers. Overall, we show a pathway to such reinvention that entails turning inward and outward (rather than to peers), a result that diverges significantly from prior understandings of professionals’ transformations.
Keywords
Scholars have well established that belonging to a profession and being socialized in its core cultural tenets can powerfully shape individuals’ thinking and actions (e.g., Van Maanen and Barley, 1984; Abbott, 1988; Trice, 1993; Bechky, 2011). Professional membership has been shown to impact individuals’ perceptions of what they consider legitimate (Fine, 1996; Knorr-Cetina, 1999; Sandefur, 2001; Eyal, 2013) and acceptable conduct (DiBenigno and Kellogg, 2014; Christin, 2018; Ranganathan, 2021). As people become strongly attached to their profession, they try to hold on to these core tenets and protect themselves from alternate worldviews. This attachment can even lead professionals to act in unexpected ways, including opposing managerial demands (Turco, 2012), voluntarily performing scut work (Huising, 2015), and making immense personal sacrifices (Bunderson and Thompson, 2009).
Unsurprisingly, because professionals have “deeply held” beliefs (Kellogg, 2014: 24), they tend to strongly resist practices that may conflict with their profession’s core tenets (Kellogg, 2019; Wiedner, Nigam, and da Silva, 2020; Anthony, 2021). Past literature has highlighted that strong external pressure is often needed—but not always sufficient—for people to accept practices that are antithetical to these core tenets. For instance, scholars have documented that new technology, regulations, or encroachments from other professional groups can lead people (generally begrudgingly) to accept ways of working that may significantly differ from their past beliefs. When external pressure forces professionals to reassess their work, they mainly turn to peers in their profession for guidance in navigating their work reinventions (e.g., Barley, 1986; Timmermans, 2002; Cohen, 2013; Mazmanian, Orlikowski, and Yates, 2013; Nelson and Irwin, 2014; Kahl, King, and Liegel, 2016; Bechky, 2020; DiBenigno, 2020).
Yet, there is growing evidence that in the absence of external pressure, some professionals (not an entire profession) may voluntarily reinvent their work. These include district attorneys who shift their priorities from incarcerating criminals to decriminalization and community action (Schoenfeld, 2016; Davis, 2019) and soldiers who change their work goals from waging wars to building states (Koonings and Kruijt, 2002). Scholars have devoted much less attention to exploring how these and other professionals may voluntarily adopt practices that break with their professions’ core tenets. The scant empirical work documenting this phenomenon has generally focused on the consequences to the profession overall (Galperin, 2020) or how professionals, already having decided to reinvent their work because of established personal beliefs, convince peers to accept the reinvention (Howard-Grenville et al., 2017: 525). We therefore still know little about how some professionals may voluntarily reinvent their work before they potentially try to reshape their entire profession.
In this article, we identify a pathway to such reinvention. The study’s setting is French anesthesiologists who voluntarily adopt the practice of hypnosis in the operating room (OR). In France, anesthesiologists have been at the forefront of introducing hypnosis to surgical settings in which it can replace the use of general anesthesia during various procedures. Adopting a practice that most anesthesiologists considered subjective and almost magical necessitated a shift in a core professional tenet of these anesthesiologists: the idea that evidence of their tools’ and techniques’ efficacy had been validated by rigorous scientific studies (i.e., evidence-based medicine). Drawing on interviews and observations, we analyze how some anesthesiologists voluntarily reinvent, or reboot, their work, which we define as voluntarily adopting, alongside older practices, one or more newer ones that are perceived to be antithetical to the core tenets of one’s profession.
Our findings reveal how turning inward to oneself (i.e., focusing on one’s own direct experiences of clients) and turning outward to clients (i.e., relying on relations with those outside the profession, namely clients) played a critical role in this process. Turning inward, by directly experiencing benefits to patients that went well beyond what these anesthesiologists were accustomed to, convinced the anesthesiologists and allowed them to convince “adjacent professions” (Halpern, 1992: 994) (in this case, surgeons) of the new practice’s efficacy. Turning outward, by relying on patient relations, words, and feedback, allowed these anesthesiologists to believe in and convince surgeons of the practice’s necessity and to protect themselves from their peers’ pushback. By turning inward and outward in these ways, they were able to justify both to themselves and others the need for the transformation, reframe their profession’s core tenet regarding what constituted legitimate evidence, and adjust the behaviors of those around them to accept the new practice. Overall, we show a pathway to a voluntary reinvention that entails turning inward and outward rather than to professional peers.
Our study contributes to the literature on professions in at least two main ways. First, we reveal how some people who are deeply embedded in their professions may voluntarily adopt practices that they perceive to be antithetical to their profession’s core tenets. This finding helps explain the puzzle of reinventing one’s work in the context of no or little external pressure to do so. It also clarifies how some members of a profession can individually stray from the norm before they potentially try to change the entire profession. Second, our study spotlights the critical roles of direct experiences with clients and relying on client relations in professionals’ reinvention. Past studies have suggested that the dynamics of reinventions primarily remain within a profession’s realm through people turning to peers to navigate externally imposed changes or, in rare cases, peers convincing peers when changes come from within a profession. Yet, these views do little to capture the complexity of the internal and external dynamics that can underpin a rebooting of one’s work. By contrast, our model of turning inward and outward accounts for such complexity and suggests an individual professional reinvention that is partly decoupled from the profession as a whole.
The Puzzle of Professionals’ Individual Reinvention
The Shaping Power of Professions
Belonging to a profession is a powerful experience (Anteby, Chan, and DiBenigno, 2016). The process of how professional norms can transform individuals as they learn to belong to a group and “embrace the beliefs and ideologies of that community as their own” (Bunderson and Thompson, 2009: 39) has been repeatedly documented across settings. These include medical residents transformed during their residency as they learn to care for patients but remain emotionally detached (Becker et al., 1961; Konner, 1988; Bosk, 2003; Pratt, Rockmann, and Kaufmann, 2006) and engineers socialized to believe that technical innovation originates only within their professional community (Lifshitz-Assaf, 2018) or that being promoted up signals incompetence (Cardador, 2017).
Professional cultures often shape individuals’ perceptions of what is worthy of their time and efforts (Heimer and Staffen, 1998; Cahill, 1999; Margolis and Molinsky, 2008; Koppman, Mattarelli, and Gupta, 2016; Fayard, Stigliani, and Bechky, 2017; Chown, 2020; Evans, 2021). For instance, nurses consider showing affection to patients to be inappropriate, while patient care technicians view it as crucial to doing a good job (DiBenigno and Kellogg, 2014). These expectations can be so deeply internalized that people carry them even when they change jobs and evolve in their careers (Dokko, Wilk, and Rothbard, 2008; Battilana and Dorado, 2010; Almandoz, 2014; Bourmault and Anteby, 2020).
When new practices and ways of working conflict with core professional tenets, it can be quite challenging for professionals to accept them. Many studies show that because professionals have deeply held values and identities, they tend to strongly resist practices that clash with their professions’ key tenets (Edmondson, Bohmer, and Pisano, 2001; Hallett, 2010; Kellogg, 2019; Sandholtz, Chung, and Waisberg, 2019; Wiedner, Nigam, and da Silva, 2020). For example, a policy change in hospitals failed because doctors refused to do work, specifically asking patients about social problems that lead to health issues, that did not align with their professional norm of caring solely for medical needs (Kellogg, 2014). Likewise, when robotic surgery emerged, numerous residents struggled to gain expertise because it involved breaking from established ways of learning in their profession (Beane, 2019).
Peers as a Main Source of Guidance in Involuntary Reinventions
Strong external pressure is the most documented driver forcing professionals to accept ways of working that may differ significantly from their profession’s core tenets. Such pressure, which includes new technologies, new regulations, and encroachment from other professional groups, compels professionals to adapt. They reassess their work because they have limited choice in the matter, and they generally turn to their peers to navigate their reinventions. Past scholarship has highlighted three main pathways, which all entail turning to professional peers, to explain how professionals reinvent under such external pressure (Howard-Grenville et al., 2017). Professionals may (a) anchor on their professional associations to negotiate reinventions, (b) collectively craft revised tenets to align with imposed changes, and (c) improvise daily practices with other members of their profession that eventually become established patterns of work.
First, when faced with direct external pressure, people may anchor on their professional associations to negotiate and manage reinventions. People enlist these gatekeepers of their profession to assert power and control over aspects such as educational standards, accreditation, and other relevant policies. Sometimes they lean on these associations to try to minimize reinventions of work (Freidson, 1983; Abbott, 1988; Timmermans, 2002). For instance, some doctors turned to their professional associations to limit changes to their core professional ideals (advancement of science) in light of new regulations and pressure from other professionals, such as public health workers whose ideal was to promote care (Dunn and Jones, 2010). Other times, professionals may turn to these associations to push for expansion of their jurisdictional boundaries, and they may take on new practices in their reinventions of work (Zetka, 2001; Anteby, 2010; Bechky, 2011; Karunakaran, 2019). For example, to reinvent themselves when the new technology of computers forced them to reassess their work, production planners anchored on their professional association, which successfully “added new tasks and redefined existing tasks” of these planners (Kahl, King, and Liegel, 2016: 1091).
Second, when strong external pressure initiates changes, people often unite with others in their profession to revise and adjust core tenets (Dobbin and Sutton, 1998; Kalev, Dobbin, and Kelly, 2006; Lifshitz-Assaf, 2018; Stice-Lusvardi, Hinds, and Valentine, 2023). Instead of using power and control to negotiate reinventions, this pathway involves professionals collectively reframing tenets to persevere in their new environment, often building on “the occupation’s history and normative roots” (Howard-Grenville et al., 2017: 527). For instance, the norm of working long hours was a central professional tenet for surgeons. After the introduction of a new regulation shortening the number of hours that interns could work, some surgeons came together and revised the tenet to reflect that well-trained surgeons should be “efficient” as opposed to “iron-men” who needed to handle long hours (Kellogg, 2009: 675, 681). Similarly, when internet search tools were introduced, librarians who were initially quite resistant eventually turned to one another in the face of a technology that posed a threat to their jobs. They reframed their core tenet to be “connectors of people and information,” as opposed to professionals who controlled “how information should be organized and searched for” (Nelson and Irwin, 2014: 904).
Third, when facing external pressure, individuals have turned to professional peers to improvise their daily practices and best figure out how to reconfigure their work. This path to reinvention tends to be less organized and planned than the two mentioned above, but it still involves individuals relying on and working within the profession to conceptualize, judge, and justify new work patterns that eventually become institutionalized (Bailey, Leonardi, and Barley, 2012; Cohen, 2013; Pine and Mazmanian, 2017; Barley, 2020; Kellogg, Valentine, and Christin, 2020: 391; Vaughan, 2021; Koppman, Bechky, and Cohen, 2022). For instance, when CT scans were introduced in hospitals, some radiologists collaborated to reconfigure their work patterns and master the novel technology (Barley, 1986). Likewise, toxicologists worked together to judge the necessity and efficacy of adopting new practices when the rise of DNA testing in forensic biology pressured them to reassess the ways they presented the drugs and poison found in bodies (Bechky, 2020).
Limited Understanding of Voluntary Professional Reinventions
While professionals engage in the involuntary transformations described above, growing evidence suggests that some professionals (not an entire profession) may voluntarily adopt practices that may conflict with their core professional tenets. For instance, scholars have written about AIDS doctors shifting their professional mandate from “curing” to “caring” (Bayer and Oppenheimer, 2002: 36). Other inquiries into voluntary reinventions include atomic scientists attempting to use science to preserve peace rather than wage war (Gusterson, 1999); nanotechnologists instilling practices that account for not only the technical but also the environmental and biological implications of their work (McCarthy and Kelty, 2010); individual physicians collaborating with retailers despite their profession’s opposition to such connections (Galperin, 2020); and chemists initiating and spreading the use of green chemistry within their professional group (Howard-Grenville et al., 2017).
Yet, research exploring how some professionals stray from the norm and voluntarily adopt practices antithetical to core professional tenets remains relatively scant. For example, prior studies have documented individuals who voluntarily deviate from their profession, such as rank-and-file members not adhering to the collective positions set by elite members of their profession (Freidson, 1984; Hafferty and Light, 1995; Leicht and Fennell, 1997; Galperin, 2020). But these studies tend to explore how the collective is defended or the consequences of such deviance to the profession overall rather than how individuals go about their own reinventions. Moreover, the limited research that does focus on people who voluntarily reinvent work tends to assume that a key driver is the individuals’ established personal beliefs. Nanotechnologists said to have a “calling” or take a “principled stand” about upholding biological and environmental safety (McCarthy and Kelty, 2010: 416, 417) and chemists depicted as wanting to “do good” by advocating for green chemistry (Howard-Grenville et al., 2017: 550) illustrate this assumption. Consequently, the main enigma and research focus in these cases is the process of how professionals who have already decided to reinvent convince their peers to do so as well.
These studies do suggest that the journey can be quite different from those in which strong external pressure is the impetus for reinvention. Generally, instead of coming together to deal with external pressure, professionals must find alternative ways to justify changes. For example, Howard-Grenville et al. (2017) showed how chemists used pluralistic frames (i.e., normalizing, moralizing, and pragmatizing arguments) to convince fellow chemists to make changes to the chemicals they traditionally used in their work. Yet, apart from the advocates who held established beliefs (those who voluntarily reinvented work), the other chemists reinvented due to direct pressure—a “visionary change effort”—led by their peers (Howard-Grenville et al., 2017: 530). Thus, while this body of research offers some insight into how people who have established personal beliefs and voluntarily reinvent try to convince others in their profession to change, the journey of how these professionals reinvent before they potentially try to change their profession remains unclear. We turn, next, to insights from research that explores sources of guidance other than peers in how professionals conceptualize and enact their work.
Clients’ Varied Roles in Professionals’ Work
While past research exploring voluntary reinventions has not strongly focused on the role of clients, the literature on professions has increasingly explored how clients shape the ways in which professionals understand and perform their work. We conceptually distinguish two such configurations: (a) professionals’ own direct experiences of clients and (b) the relations that professionals have with clients. In the former, clients play a relatively passive role whereby the main dynamics lie in a professional’s own direct experiences of clients (e.g., directly seeing or feeling how clients react to a practice). In the latter, clients have a more active role in how professionals understand their work, whereby the relations between professionals and clients are key; for example, professionals rely on clients’ opinions or enlist clients in their work in other manners.
First, focusing on direct experiences with clients can influence how professionals perform and understand their work practices. For example, career coaches “got chills” when they directly witnessed clients become motivated by their discourse about finding passion rather than chasing paychecks; thus, the coaches interpreted such discourse as a legitimate practice (Sheehan, 2022: 1166). Similarly, Craciun (2018) showed how some professionals relied on their emotional reactions to clients to adjust their practices. This research suggests that directly seeing, feeling, and performing a practice involving clients may influence professionals’ beliefs about the practice itself. While research has generally focused on the shaping power of experiences when professional tenets are not deeply embedded (i.e., when one is new to the job), we posit that professionals’ powerful, direct experiences of clients may also play a role in loosening deeply embedded tenets.
Second, relying on relations with people outside of one’s profession has increasingly been shown to shape professional work. Recent studies have highlighted how professionals have adjusted, adopted, or rejected work practices based on their interactions with clients (Turco, 2012; Sandefur, 2015; Sandholtz, Chung, and Waisberg, 2019; Anteby and Holm, 2021; DiBenigno, 2022; Chan and Hedden, 2023). Professionals have also enlisted clients to help the professionals maintain and even construct their expertise (Wynne, 1989; Epstein, 1995; Mol, 2008; Kline, 2010; Barker and Galardi, 2011). For example, physicians engaged parents to help them fulfill their professional mandate of diagnosing autistic children (Eyal, 2013). While this work has mostly unpacked how professionals adapt their work to (or with) clients so that they can uphold their professional mandates, we suggest that such client interactions can play an even deeper role by prompting some professionals to profoundly reevaluate their outlook. Building on these insights, we turn to the case of French anesthesiologists who adopt the practice of hypnosis to better understand how some professionals can reboot their work.
Setting, Data, and Methods
Setting
In France, anesthesiologists have been at the forefront of introducing hypnosis in the operating room. Although the first documentation of hypnosis used during surgery dates to the 1830s, the practice disappeared from the OR for over a century (Wobst, 2007; Lleu et al., 2009). Belgian anesthesiologist Dr. Faymonville developed the technique as a replacement for pharmaceutical anesthesia in the 1990s, and it has slowly spread throughout Europe (Musellec, 2010). In 2005, the French professional association of anesthesiologists (Société Française d’Anesthésie et de Réanimation, or SFAR) recognized hypnosis as an official anesthesia technique, and it has become more prominent since that time (Cuvillon et al., 2020). Table 1 provides more details on the history of medical hypnosis in France.
History of Medical Hypnosis and Anesthesiology in France*
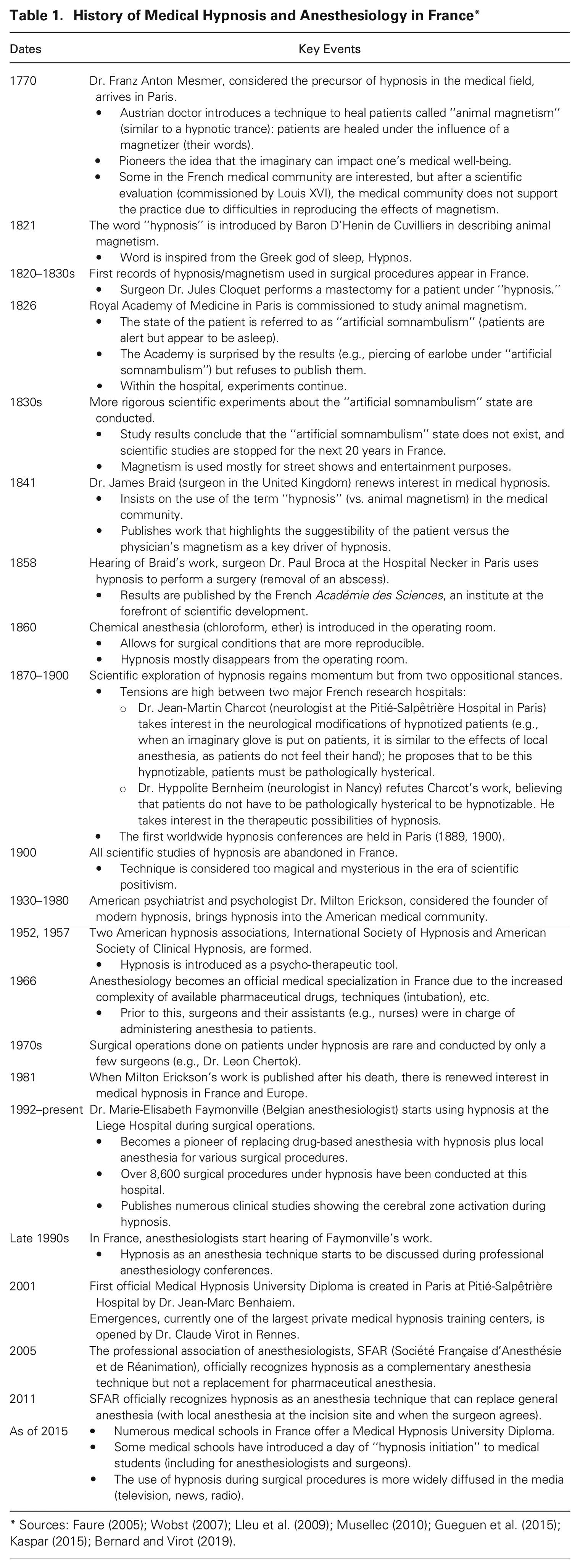
The anesthesiologists in France who first started to use the technique, in the early 2000s, explained that SFAR approached them as the association heard more discussions about the use of hypnosis in the OR (in Belgium and France). After numerous presentations and discussions about its use, benefits, and the limited scientific studies (including ones using MRIs to show which parts of the brain are activated during hypnosis), SFAR eventually approved the technique, at first as a complementary tool and eventually as a replacement for general anesthesia. While SFAR has officially accepted hypnosis and its popularity has slowly grown, it is not yet a mainstream anesthesia technique or even widely accepted by anesthesiologists. As of 2015, only approximately 10 percent of all anesthesiologists in France, or 1,000 individuals, had completed a hypnosis certificate (Gueguen et al., 2015). 1 Those who want to learn hypnosis usually undergo a training program of approximately 12 days spread out over a year. This is not part of their medical school training. 2 Hypnosis trainings are offered by private centers specializing in hypnosis (for medical professionals) or select medical schools that deliver a specialized continuing education diploma.
Formal hypnosis involves a person being in a state of modified consciousness, during which the person is still conscious but mentally disassociated from their actual physical surroundings (Cuvillon et al., 2020). 3 A classic example of modified consciousness entails a person being asked to read an entire written page and not knowing what they have just read because their mind is elsewhere. In contrast to surgery in which a patient is unconscious via pharmaceutical anesthesia, during surgery under hypnosis the patient is in a hypnotic trance, with usually only an injection of local anesthesia at the incision site. Hypnosis can replace the use of general anesthesia during a surgical procedure and can be used in a multitude of cases, including thyroidectomies and mastectomies, as well as cataract and carotid surgeries.
The main tasks of anesthesiologists are quite different during surgery under general anesthesia and surgery using hypnosis. During procedures using pharmaceuticals, they (generally assisted by a nurse) are mainly responsible for choosing the dosage and type of drugs, administering them (through an IV or mask, or regionally directly through the nerves), intubating the patient, monitoring all vital functions, and reacting if any complications arise. Their interactions with the patient are limited; they see patients minutes before the surgery and rarely interact with them after they are awake. In France, anesthesiologists are usually in charge of two to three ORs at the same time, so they are not necessarily present during the entire surgery. The nurse stays throughout.
By contrast, when anesthesiologists use hypnosis, their main role is to guide the patient to a hypnotic state and keep them there during the procedure. With their voice as their main tool, they sit next to the patient and invoke the imaginary state. Putting patients in a hypnotic state generally involves mentally taking them to one of their favorite places. Thus, anesthesiologists often describe the sounds, sights, smells, and tactile sensations of walking on the beach, climbing a mountain, or picking flowers from a garden. Unless there is an emergency, the anesthesiologists do not use their technical and pharmaceutical expertise.
Data and Methods
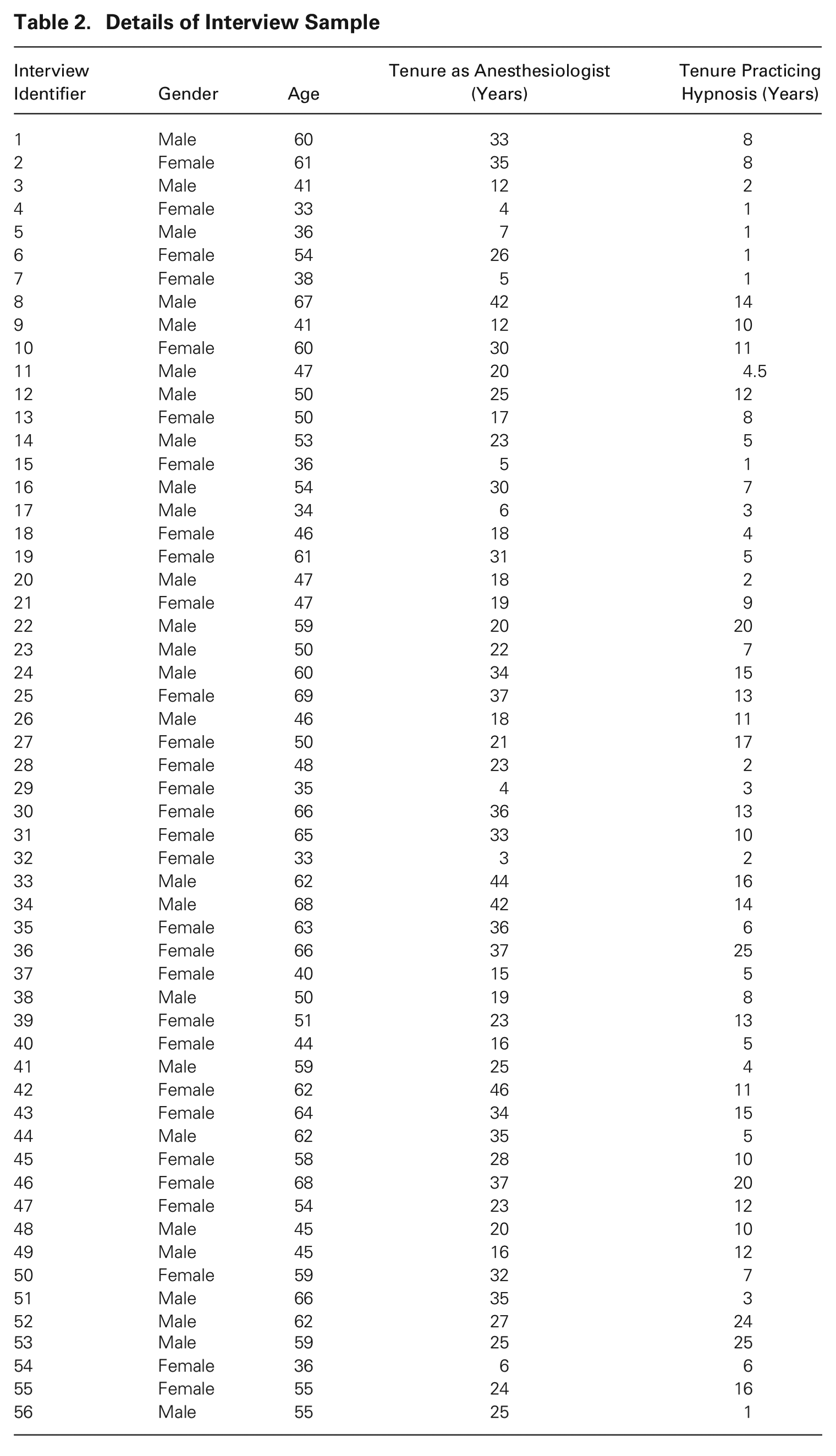
To understand how some anesthesiologists voluntarily adopted a practice that they perceived to clash with a core tenet of their profession, we analyzed 63 interviews and 125 observation hours. After we conducted a few pilot interviews in 2019, the bulk of our data collection took place from 2020 to 2021. We conducted 56 open-ended interviews with French anesthesiologists who practice formal hypnosis in the OR. To obtain a richer contextual understanding, we also interviewed seven other individuals: one doctor who founded a main medical hypnosis training center, one surgeon, one patient, three anesthesiology nurses who practice hypnosis, and one anesthesiologist who does not.
We constructed our interview sample primarily by contacting anesthesiologists who were listed as trainers on the websites of the main hypnosis training centers in France. We received additional snowball contacts through the people we interviewed. On average, interviewees were 53 years old, had been anesthesiologists for 24 years, and had been practicing hypnosis for nine years. Fifty-four percent of interviewees were women (see Table 2 for details on interviewees).
Details of Interview Sample
Interviewees generally attended a hypnosis training program out of boredom and curiosity, not knowing much about the practice beforehand. These courses (and many others) could be used to fulfill credit requirements of their continuing medical education. Some even chose hypnosis trainings because they coincided with non-work motivations, such as location in a city they wanted to visit or timing that allowed them to attend with friends, rather than a particular interest in the practice. Overall, before attending the training, most interviewees were not convinced they would even use the technique. The frequency with which they practiced hypnosis for procedures ranged from multiple times per week to once per month. Thus, all interviewees conducted both traditional anesthesia (using drugs) and hypnosis (no/limited drugs).
Interviews lasted approximately one hour and were digitally recorded and transcribed. We followed an open-ended interview protocol with general questions about the interviewees’ career paths and their journeys with the technique of hypnosis. In general, we allowed the interviewees to guide us to the subjects that were important to them, specifying that we wanted to understand their job and the role of hypnosis in it. All quotes from interviews used in this article have been translated from French into English by the co-authors.
In addition, we observed and participated in hypnosis training programs that medical professionals attended at hospitals and private centers in Paris (three times two-day weekends and two weekdays, amounting to 67 hours). We also observed a biennial medical hypnosis professional conference (three days, amounting to 24 hours). Finally, we had the opportunity to directly observe anesthesiologists with patients in hospitals (31 cases, amounting to 34 hours). In all instances, we drafted field notes within 24 hours of each observation.
After our initial interviews, each author separately read selected transcribed interviews, highlighting recurring and salient topics. A common theme was that these anesthesiologists perceived the practice of hypnosis as quite divergent from their traditional tools and how they were trained. For a first step, we wanted to get a good grasp of why this was, and so our first round of interviews and coding focused on understanding what made it so different in their eyes. We began by coding the dimensions along which hypnosis changed their work.
We quickly realized that in addition to changing their work tasks, the anesthesiologists also considered hypnosis to differ on a more profound level from their past socialization. Therefore, we also coded how they conceptualized their traditional methods versus hypnosis. For instance, anesthesiologists systematically used terms such as “evidence-based medicine” and “randomized double-blind trials” when describing the traditional training and mindset of their profession. We coded these concepts as “legitimate evidence in traditional profession” (from their point of view) and ultimately as a perceived core tenet of their profession.
Once we established that they perceived hypnosis as a practice that conflicted with their profession’s core tenet, we focused on gaining deeper understanding of how these anesthesiologists adopted a seemingly antithetical practice. We identified three systematic challenges that this reinvention entailed: justifying to oneself the use of a seemingly antithetical practice, convincing surgeons to accept one’s own reinvention, and shielding from pushback by peers. We also identified various themes regarding how anesthesiologists overcame these different challenges. As interviews and our analysis progressed, we were surprised by how little they talked about their professional associations (which had validated hypnosis as an official anesthesia tool) or their hypnosis-practicing anesthesiologist peers, in their overall journey. We initially thought that anchoring on these two elements would play an important part. We were instead struck by the persistent theme of patients and direct experiences in how these anesthesiologists reassessed their work. At this point, we also went back to the literature to identify what was most unusual in relation to existing theory. We realized that our data seemed to be challenging existing literature on how professional reinventions may happen. As this phenomenon seemed counterintuitive and most promising for novel theory development, we decided to center our analysis and coding on it. 4
The puzzle that we constantly revisited centered on how professionals could so fundamentally reinvent their work when they faced no obvious pressure to do so. Given our focus on theory elaboration, after we had identified the main puzzle we each separately reanalyzed the transcriptions to identify themes within the general notion of reinventing one’s work, wrote memos to document themes that emerged, and met to discuss and compare. We then went back to our data and used these themes as coding categories, such as building on one’s own experiences to believe in the practice’s efficacy. For example, the salient topic of “showing surgeons how their patients calm down with hypnosis” became the broader theme “showing surgeons direct impact to their work with hypnosis,” which became the coding category “leveraging adjacent professionals’ own experiences of clients to convince them of new practice.” When new themes that contributed to the reinvention emerged (such as strengthening connections to outsiders to buffer pushback from peers), we added them.
The data analysis process was iterative, and we constantly went back and forth between our individual transcription analyses, memos, and discussions (Charmaz, 2006; Golden-Biddle and Locke, 2007). We continued this process until we had identified clear, consistent themes regarding voluntary reinvention both across and within interviews, keeping in mind how these themes could contribute to existing theory. Once we had reached a saturation point at which no new themes emerged in our data, we each coded all the interviews to deepen our understanding of our main puzzle. We then compared our coding and discussed discrepancies in how we had coded certain passages until we reached agreement.
Findings
The Voluntary Reinvention of Anesthesiologists’ Work
During medical school and through their residencies, anesthesiologists were deeply socialized in a profession in which science and evidence-based medicine formed their knowledge and legitimized the tools they used, such as drugs and epidurals. Their medical training centered on “a deep scientific foundation” (Interview 9) that shaped the basis of their expertise: “How do we make the drugs? What dosage? What are the complications? The risks? It’s very scientific” (7). They explained how scientifically sound evidence was critical in validating their tools: “The most dangerous medicine of pharmacology is in the hands of anesthesiologists, and we are able to do many things by correctly using these medications” because of “scientific proof” (21). 5 As an anesthesiologist during our observations explained, in the hierarchy of evidence, evidence from randomized control trials was the gold standard in their profession, and they often depended on such evidence to gauge the efficacy of their tools: “This drug 30 percent of the time will diminish certain things, and this dosage will do this, with these side effects” (54).
As a result of their training, a perceived core tenet of their profession was that legitimate evidence was gathered by rigorous scientific research, namely evidence-based medicine (e.g., double-blind randomized studies, before-and-after studies, replicable average effects); this evidence validated the efficacy of the traditional tools in their repertoire. Anesthesiologists also often considered themselves to be very Cartesian and rational. The scientific mindset was the quality they considered imperative to doing their jobs: “When we finish our anesthesiology training, we are inevitably very, very scientific . . . I remain scientific because if not I can’t put my patients to sleep . . . it’s the basis [of my work]” (6).
Anesthesiologists also stated, however, that hypnosis was a technique that “encourages vagueness” (14) by “using the imaginary” (43). They explained that over the past 15 years, a great deal of progress had been made with scientific studies of hypnosis; they also acknowledged that they did not yet completely understand how hypnosis functions. While it was common to not fully know the mechanisms of how new drugs and therapies in the medical field worked, they believed that sound evidence gathered by randomized control trials (or other rigorous methods when trials were not possible) still provided the most valid scientific proof of the effects of new techniques.
Yet, they considered the existing research-based evidence of the hypnosis technique to be on the lower end of their hierarchy of evidence. For instance, an anesthesiologist during our observations who was active in research on both traditional tools and hypnosis recounted that current scientific studies of the effects of hypnosis were at the very beginning stages in terms of what was considered rigorous evidence in their field; thus, it was something he hoped to develop. Similarly, another stated that it was “very difficult for it to be validated by evidence-based medicine because it is a subjective technique . . . first of all it’s absolutely impossible to do double-blind studies with hypnosis” (2). Others recounted that replicating the effects of hypnosis for scientific studies was also a challenge, as variability based on individual patients and practitioners existed and aspects such as trust between the two played a critical role.
Consequently, they considered adopting hypnosis as quite different from using pharmaceutical drugs, whose efficacy was very rigorously validated by scientific proof. In short, in their eyes, hypnosis “was not as scientific as when I inject a drug” (6). During the training sessions we observed, instructors (doctors who practice hypnosis) described hypnosis as requiring “set[ting] aside pure logic and hard science.” For this reason, at first, several attendees had mixed feelings and were a bit skeptical because they had the image of something “a little magical” (15), not in fact based on science. As one, who initially described himself as pretty recalcitrant to hypnosis, explained, “I didn’t believe in it at all (laughing) . . . well I was shaped by medical school. For me it was largely alternative medicine . . . a grandmother’s remedy or witchcraft” (11). Because the anesthesiologists perceived hypnosis to be in conflict with one of their profession’s core tenets, embracing it entailed a reinvention of their work: “The mold of all our medical training is this [rigorous science], so it means that you must, well succeed in getting out of it, changing things. Changing habits. That’s the most difficult” (11).
The reinvention of work was not merely a change in mindset but also manifested in several key behavioral aspects of the anesthesiologists’ work. When they used hypnosis rather than traditional drugs, their work flipped from focusing on the technical to the human aspect of medicine, from following procedures to improvising, and from being a fleeting and invisible to a fully present and memorable figure to patients. Together, these shifts fundamentally changed the anesthesiologists’ work.
Focusing on technical versus human aspects of medicine
During surgical procedures without hypnosis, anesthesiologists described their jobs as technical and drug-related. They mainly dealt with aspects such as managing intubation, ventilation equipment, ultrasounds used to place anesthesia directly in nerves, and pharmacology—choosing the type of medication and dosage to put patients to sleep. In fact, many were drawn to the specialization because of “the very technical side of anesthesiology, where you need to be quick, where you need to perfuse or you need to put tubes everywhere” (4). Their focus was mainly on patients’ physical and medical health. Talking to patients or taking into account aspects such as patients’ emotional states was largely out of their domain of expertise: The job of an anesthesiologist is to be ready for anything, do something very technical. We assure that everything is done in security . . . but we don’t learn to bring this security to people with care, with kindness . . . they teach us to do everything that is really, very technical, without making mistakes. It has to work each time. We have to be sure. And if for some reason it doesn’t work, we need to know what to do . . . we take care of the patient, but we don’t really take care of their wellbeing and what they may feel. (15)
In stark contrast, during procedures under hypnosis, anesthesiologists did their job “without the whole technical part . . . we don’t need tools in hypnosis. We just need, well, us, our voice . . . it allows me to do anesthesia and alleviate people’s [pain] without anything” (15). Hypnosis required them to use their voice and imagination to establish a bond with the patient, sometimes just minutes before the operation. One described the critical role of this relationship in hypnosis: “It’s the direct relationship with the patient . . . he is here, I am here, and he is concentrated on what I say . . . it’s the power of the imaginary and the mind vis-à-vis all the aggressions in the OR” (5).
Thus, anesthesiologists’ focus shifted suddenly to consider the “human side” (9) of the patient in order to create a connection with them; this bond allows patients to trust anesthesiologists enough to guide them to a hypnotic state. In several training exercises we observed, instructors asked participants to move their chairs to stay closer to the patient. As a participant noted, this was the opposite of using pharmaceutical drugs: “You inject a drug, it’s over. [But] here you must create a relationship and through this relationship, you must detach the patient from the context of the OR” (8). Anesthesiologists repeatedly highlighted that “you can’t do hypnosis without having empathy [for the patient]” (14). Consequently, this required them to pay close attention to patients’ state of stress, fears, and other emotions. (See Table A1 in the Online Appendix for additional evidence of behavioral changes.)
Following procedures versus improvising
Anesthesiologists also emphasized that following rigid procedures was a major part of their jobs, ingrained in them since their medical training: “We are trained to apply protocols. For problem X there is solution Y that gives a good result” (11). They applied procedures to their work to determine which dosages and medications to use; which steps to take to prepare the patient before, during, and after a procedure; and what to do in emergencies (e.g., unexpected reactions to medications). Mastering and rigorously applying these strict protocols were crucial to help guarantee the patient’s safety: We have the lives of people in our hands . . . we can’t afford to make a mistake. It’s very difficult to have no room for mistakes. When we are anesthesiologists, and it’s the case for everyone that I know, we are all very exact. The way we work, we are very Cartesian . . . procedures all the time. You must compare it to an airplane pilot. We often make that comparison . . . meaning we have a lot of procedures; we know them. (6)
In contrast, using hypnosis required anesthesiologists to adapt to each patient’s unique experience; they perceived it as difficult to follow their usual strict protocols: “[With hypnosis] there is no recipe . . . it depends on the patient, but that’s what changes” (7). An anesthesiologist described this contrast: “Before this operation [using pharmaceutical anesthesia] you must do this, must do that, an EKG, a blood test. Starting at this age you do that, at this age you put them to sleep with this. Well hypnosis doesn’t fit in these checkboxes” (2).
Indeed, when using hypnosis, they viewed their work as markedly less standardized in terms of process and procedure: “in the OR, I am able to improvise” (6), summed up one person. Another participant illustrated this need to improvise, describing an operation with an elderly patient with breast cancer who was too weak to undergo general anesthesia and was having a mastectomy: The night before, since I was worried, I went to see her [in her hospital room] and we did a [hypnosis] session together, and she went in a deep trance . . . and so the next day, she goes into the OR, we install her and . . . she wanted to go walk in the forest, so I told her we were going to return to the forest. She looks at me and says “Young lady, yesterday we were lying in my room. It was okay, but today I don’t know if you realize, but they are going to remove my breast, we are in the OR . . . and you want me to go back to the forest? No way!” . . . At that moment the surgeon was ready; everyone was ready. So I said, “You are completely right, we can’t go back to the forest.” So, we started on something else. I said, “Look at the surgical light,” because she was lying down. Then I started describing it, all the mirrors pointing in different directions, the colors, and she went into a trance like that . . . you must know how to bounce back. (2)
Being a fleeting and invisible versus a fully present and memorable figure
Finally, anesthesiologists were often fleeting figures in the OR, “ghosts” (23) in patients’ experience. As they were generally in charge of two rooms at the same time, they were ephemeral. 6 While their expertise was vital for the patient to undergo the procedure, they were mostly needed only for certain key moments (e.g., putting the patient to sleep, waking them up); thus, they had a transient role with the patient if everything went smoothly: “snap–snap–snap . . . hello–goodbye, I inject” (9). Patients often did not know who they were or even all that they did since during most of their time with anesthesiologists, they were unconscious: “In the end we have very little interaction with patients . . . most of the time, people know very well who performed the operation but absolutely not who put them to sleep” (15). In patients’ eyes, unless something goes wrong with the anesthesia, “we are nobody” (7).
When using hypnosis, however, the anesthesiologists’ role flipped to being fully present in the OR and memorable to patients: “It’s less easy than injecting medicine, because it requires a much bigger personal investment. When I do chemical anesthesia, we inject drugs; once the patient is asleep, we can do what we want. But during hypnosis, we must always be present, concentrated, attentive” (12).
Keeping the patient in the trance during the entire procedure meant “a permanent presence and . . . lots of energy” (13) for anesthesiologists. They described sitting next to the patient, their head against the patient’s head, and talking about the place the patient wanted to go to. They had to fully concentrate on patient movements to gauge whether they were comfortable and on what the surgeon was doing to incorporate such gestures into the hypnotic trance. An anesthesiologist illustrated how his full presence was required during an egg retrieval procedure for in-vitro fertilization under hypnosis (normally done under general anesthesia). The patient wanted to go to the beach: I asked her to take a deep breath and . . . observe the air that was entering her nostrils and that warmed her body; and this warmth maybe reminded her of the warmth of the beach, where you are. You are on the beach, and so I accompany her on the beach . . . I ask her “Do you feel the sand on your hands” for example . . . mostly I talk but sometimes I ask a question to make sure the patient is where I think she is . . . and I have a signal to tell the surgeon, “Okay we are well installed, we can start” . . . and maybe you will feel a little coolness of the sea that is next to you. It suggests for example that we are going to prepare the skin . . . the product that we put is a little cold, so it allows me to create a link between what is happening in the OR and a sensation she may feel on the beach . . . [but] if I feel that the patient is not very comfortable, [before starting] I establish with her what we call a signaling, so that she gives me her hand or that she does a little movement to tell me that the comfort is not enough. If this happens, I tell the surgeon to stop for a moment, and I deepen the hypnotic trance. Or I inject a little medicine to ease the moment. But, I am always in relation with the patient. It’s important that she doesn’t feel abandoned. (9)
Because the anesthesiologists were fully present in the patients’ experiences, their patients remembered them. An anesthesiologist noted the contrast of feeling invisible versus memorable: “[Being] ‘shadow figures,’ it doesn’t bother me but [with hypnosis] all of a sudden we emerge a little from the fog and we say to ourselves, we did something good,” adding, “Now, the patient knows us. I am not looking for recognition [but] now they [past patients] say: ‘Ah I would like you to put me to sleep’” (23).
As detailed above, anesthesiologists’ use of hypnosis entailed a reinvention of their work both in terms of mindset and behaviors. To adopt this antithetical practice, they had to justify the reinvention to themselves and to surgeons and counter professional pushback from fellow anesthesiologists. Next, we analyze how turning inward to oneself and outward to clients (here, patients) prompted them to reframe their core tenet, convince surgeons to accept the practice, and counter pushback from peers.
Pathway to a Voluntary Reinvention
Embarking on an internal transformation
To justify to themselves the adoption of an antithetical practice, these anesthesiologists had to first reconcile the clash between the practice and their core professional tenet, to which they exclusively and strongly adhered during a significant part of their careers (on average 15 years). What justified reframing their tenet was their direct experience of the benefits of a powerful antithetical practice on their patients—benefits beyond what they were used to. This convinced them of its efficacy and called into question their profession’s core tenet. At the same time, in assessing hypnosis, they turned to patients, which transformed their professional outlook and convinced them of the necessity of the practice in their repertoire.
Building on one’s own direct experiences of clients to believe in the new practice’s efficacy
It was usually during their hypnosis training that anesthesiologists became fully convinced of the technique’s efficacy, when they began directly experiencing the benefits of the practice with patients. A large part of their training required them to practice hypnosis among themselves and, after class sessions, on their patients (not yet completely replacing hypnosis with pharmaceutical anesthesia but practicing hypnotic inductions before administering the drugs). Although doubtful at first, many anesthesiologists started to see immediate and tangible benefits in their work: “Everything that I did became a lot easier for the patients. The patients had a much better experience. For example, doing an epidural for a woman in labor, when we use hypnosis techniques, it went so much better for the patient” (25).
Another anesthesiologist illustrated how seeing the effects of hypnosis on the patient and the undeniable benefits she experienced was a key turning point for her. To do an epidural, she had placed a patient giving birth to twins in a hypnotic state. When one of the babies’ heart stopped beating, they had to do an urgent cesarean: It was really a foundational event . . . sometimes, when it happens like this . . . you need to fight against the women. Because I inject the anesthesia product, but everything happens so quickly that the anesthesia product doesn’t even have time to completely work, so the women feel and if they feel, they start panicking. If they panic, some start screaming and it’s appalling. Whereas for her, it was easy for the surgeon . . . the surgeon made the incision, took out the baby who was alive and doing very well . . . and so it ended well. Two hours later, her bed was being pushed out of the OR to go to her room, and I will always remember, the door of the OR opened, and she was in front of me. She waved her hand with a big smile, and she said to me: “It was wonderful the trip to the Maldives [where patient went during hypnosis]” . . . it was a transforming experience. I became a believer. (43)
Similarly, in our training session observations, a participant confided over lunch early on that hypnosis seemed too “fuzzy” and “out there” for her, as it differed too much from the medical theory that she was used to. She even complained that she would really like to see more scientific discussions during class. While instructors mentioned various scientific studies on voice (e.g., how a deep, monotonous, slow-paced voice was ideal) and the effects of hypnosis on pain and anxiety, a much larger part of the training centered around sharing patients’ stories, showing videos of patients in the OR, and doing practice exercises. However, at the beginning of the second session (more than a month later), this same participant, eyes wide with astonishment, shared with the class how she tested hypnosis with a patient and directly saw and felt how the patient calmed down and that it was an incredible tool.
Interviewees repeatedly noted that seeing patients wake up so much better, being able to calm screaming patients who had panicked without a sedative, and observing anxious patients remain motionless when they saw the eight-centimeter needle that would be injected into their nerves allowed them to trust that, as an anesthesiologist put it, “the power of words could be as beneficial as a medication” (17). As anesthesiologists experienced these benefits with patients, which went beyond what they were used to, their profession’s core tenet—that legitimate evidence of a technique’s efficacy could be gathered only by rigorous scientific studies—began to loosen. As one interviewee observed, “We must use different tools to validate this technique . . . different than what we have at this time. Evidence-based medicine, it’s not enough” (2).
Directly experiencing the benefits of the antithetical practice with patients was critical to convince anesthesiologists of its efficacy and, consequently, to allow them to start questioning the canon of their profession. In contrast to their process of accepting new drugs, for which reading journal articles or even hearing how colleagues used the tool could be convincing, anesthesiologists were rarely persuaded before they tried hypnosis and saw its direct effect on their patients. Similarly, trainers during our observations noted that it was imperative to start using hypnosis techniques on patients (in addition to drugs) just after the first training session. A main reason, they stated, that some anesthesiologists received training but did not end up using hypnosis in their work was that they never directly experienced its benefits; they did not have the confidence to try it on patients right away. 7 As a trainer explained, “if we don’t put it into practice right away, we never will” (36).
Turning to clients to believe in the new practice’s necessity
While anesthesiologists became convinced of the practice’s efficacy, to willingly go through the challenges of adopting a somewhat contested practice, they also had to profoundly believe in the necessity of the antithetical tool. As many mentioned, their pharmaceutical tools were already quite sufficient for them to do their jobs well: “Our technique has become so sure, it’s so 100 percent. Almost. We say that anesthesia is a medical technique that is surer in terms of security, in terms of mortality and injury, than air transportation, that is known as the most secure” (34). However, by turning to patients’ words, they saw hypnosis as an essential added tool for them to be good anesthesiologists.
Having a distant relationship with patients was strongly embedded in their socialization and reinforced in their work when using traditional anesthesia: “The relationship with the patient . . . it’s something we never learn in medicine” (7). Consequently, deeply interacting with patients was traditionally not strongly valued in their profession. As one interviewee noted, it was easy to discount the “relational” aspect of their work because “people are asleep” (26). By contrast, hypnosis was a practice that required making a connection, having empathy, and crafting a personalized relationship with patients. When anesthesiologists first opted for hypnosis and experienced a “more privileged relationship” (29) with patients, what struck them was patients’ feedback. An anesthesiologist recalled the moment when she first decided to use hypnosis and how her patient’s feedback moved her: “The first time it was here, with a cancer patient that was really stressed and was crying. So I started . . . and she [patient] was really, really happy . . . and she thanked me. And that touched me” (13). Another one vividly remembered her first hypnosis experience and how the words of her patient, who had to undergo an abortion [under local anesthesia], profoundly marked her: I said to myself: Okay I am going to try, we’ll see . . . I had the idea: in any case they have nothing so it’s not a big deal if it doesn’t work . . . and she went directly [in a trance] . . . and after they told me: it’s finished. So I brought her back . . . all the same I remember a moment, she started crying because well, an abortion, it’s not always easy. . . . So I brought her back and she said to me, “I cried but felt good. Thanks to your voice, I was somewhere else.” . . . I will remember [this] my whole life. She told me: “I don’t know how I would have managed without you.” (28)
As they continued experimenting with the practice, many anesthesiologists recalled patients’ feedback that deeply touched them: “This woman [undergoing a hernia operation using hypnosis] point blank, asked me ‘please hold my hand, I need you.’ So she squeezed my hand and after, she thanked me. It was really powerful for her and really rewarding for me” (14). Another interviewee stated, “As soon as he heard my voice [after the procedure when he went to see his patient], he had a huge smile . . . He even took my hands. It was really nice” (12). Other patients’ words, thanking them, telling them it was superb or perfect, prompted these anesthesiologists to reassess what they should (or should not) be doing. They started to question whether having a distant relationship with patients was indeed sufficient for them to be good anesthesiologists, which was a big revelation: When I had my first contact with hypnosis, I discovered a universe. We discover that we really need to communicate to do well our profession and practice anesthesiology. . . . I started to realize that patients in fact thanked me [when first using hypnosis]. They thanked me after an anesthesia when I went to see them, and that had never happened to me. In general doctors have one particularity, which is that they are sure to know everything. And, as a doctor it’s really difficult, well I had to deeply question the way I worked. It’s really difficult. As an anesthesiologist you say to yourself “I am good, I know my interventions, I know what to do” . . . but it [hypnosis] calls [this] into question. (23)
Guided by patient feedback, they began to view this personalized connection as something that helped them do their jobs better. Beyond just allowing the surgeon to operate on a patient, which is a main objective of their traditional expertise, they felt they could now also make patients happier, more comfortable, and less stressed because they knew patients better and were “more in contact with the patients . . . a tool, sometimes stronger than morphine” (6). They typically explained their sentiments from this patient feedback as follows: “I take better care of people since using hypnosis” (7), and “We really have the feeling that we make a difference for them. It’s really gratifying, to help people like we do” (15).
In a remarkable reordering of what most anesthesiologists typically believed, they gradually viewed having a deeper relationship with patients as necessary to being a good anesthesiologist. With regard to traditional distant patient connections, they now described their past job as dehumanizing or even an assembly-line job. Patient relationships also became a strong source of gratification to them: “I rediscovered my anesthesiology job. Meaning I appreciate it in a new light, because of the improvement in the relationship with patients . . . it energized me” (13). One summed up the profound transformation in her outlook: The heart of the job, it’s the relational. It’s to be completely attentive to the patient and to go as far as possible to respect the patient’s wishes . . . and that I discovered . . . I didn’t know that before hypnosis. I discovered it with hypnosis, and that is how I learned to really love my job. (43)
Thus, these anesthesiologists now considered this previously antithetical practice as strongly aligned with their newly discovered professional outlook and a necessary part of their repertoire: To be completely honest I think it is indispensable. I think it’s a tremendous asset, very positive, in how to speak to people. All the young people I see, I strongly encourage them to get trained. It will be almost as essential as knowing how to do locoregional [anesthesia] for the young generation. That’s for sure. On top of that it brings back a human dimension. We are going too far into a practice of medicine that is too scientific. We are too much in the technique . . . here we rediscover the art of medicine and we rediscover the whole patient dimension. It’s not just an arm, a part of a body. It’s a whole person. (31)
Reframing one’s professional core tenet to align with the new practice
Convinced of both the efficacy and necessity of hypnosis in their toolkit, these anesthesiologists saw a justified reason to reframe their tenet to align with the practice. They thus expanded their profession’s core tenet for themselves by enlarging their notion of legitimate evidence: “We don’t necessarily have to rely on evidence-based medicine, to be able to justify that it is something efficient and useful . . . there is not only this truth of evidence-based medicine” (9).
Evidence could mean rigorous scientific proof but now also their firsthand experience and input from patients. For instance, an anesthesiologist explained, “I used hypnosis and I saw that it was efficient and very interesting. I am convinced. Experience is another way to know . . . what matters is the effect that I see on the patients” (12). Similarly, one instructor during a training session we observed even turned bright red and raised his voice as he expressed his frustration with relying solely on scientific proof: “I am so tired of people telling us we need scientific studies to prove it [hypnosis] works.” He referred to the COVID crisis as an analogy, saying that for a century, people had used a certain medication for patients who were suffocating, but the medication was not authorized for COVID patients until double-blind scientific studies were done with these patients (the medication was eventually approved). He condemned health authorities for letting people die because of the former’s obsession with scientific studies and emphasized the legitimacy of empiricism and observing results with patients.
While these anesthesiologists reframed a core tenet, they did not completely abandon it. They still believed that rigorous scientific evidence was important; it was just no longer the only legitimate evidence for them: “I am still [Cartesian] that doesn’t change. But let’s say it like this: there are more curves around the edges” (14). For instance, they viewed the scientific neurological research exploring hypnosis as extremely important because it brought some credibility to the technique. However, many viewed it as confirmation of what they already saw in their patients: “it simply shows that there is a neurological phenomenon during hypnosis . . . but we [already] see it” with patients (8). The patient inputs and reactions they observed became the real evidence for them: “We are obligated to do [scientific studies] because if not, we lose legitimacy. If we don’t do these studies they will say that indeed it’s magic . . . but for us, if the patient is happy, that’s it, we have the result” (9).
These anesthesiologists voluntarily embarked on a journey of reassessing their work. They largely drew on their own experiences of clients, but they also relied on relations with clients (patients) in their reevaluation. In doing so, they underwent an internal transformation whereby they changed their professional outlook and reframed their profession’s core tenet. They had no idea beforehand that learning hypnosis would result in this change.
Many anesthesiologists decided to attend a training not really knowing what to expect, often after hearing about the technique at a professional conference or through colleagues. As one explained, “There is a kind of routine in the [traditional] technique, a certain moment that we are a little used to what we do. I said to myself in any case it would at least bring me something to see, and, it brought me more than that” (1). Others who attended training did not foresee that they would ever use the practice; one participant recalled that they had fulfilled a “dare” from a colleague because “he never thought I would do it; I am really the opposite of that” (14), and others attended because the training was in a city they wanted to visit: “I said to myself, it’s folkloric. It will be interesting, funny . . . I didn’t think I would use hypnosis one day. It really wasn’t my objective . . . in the end, this training was a big turning point in my life” (26).
Undeniably, these anesthesiologists were open to learning something new and were tired of their daily work’s repetitiveness. But the vast majority turned to hypnosis not because they thought it was an efficient or necessary tool for their repertoire or because they already strongly questioned their profession’s core tenets and outlook: “I didn’t know this technique at all. I didn’t know that I was missing something. At the beginning it was really ‘what is it,’ it was curiosity” (13). 8 As shown above, these beliefs generally developed afterward as they underwent a transformation. Ultimately, the antithetical practice no longer seemed antithetical to them. In fact, they now saw the practice as harmonious with their new professional outlook and, thus, were willing to leave their comfort zone and conquer the stress and fear of plunging into “a new technique that no one around you really masters” (15). (See Online Appendix Table A2 for additional quotes illustrating the pathway to voluntary reinvention.)
Onboarding adjacent professionals 9
When anesthesiologists accepted hypnosis as a legitimate tool and wanted to use it to replace general anesthesia, surgeons also needed to accept the technique; if the surgeon did not agree to do the surgery with the patient under hypnosis, little could be done. Given that hypnosis was viewed as a very subjective technique, it was a challenge to convince surgeons since they were generally as scientific as the anesthesiologists were and thus were often skeptical: “They don’t believe it will work, they don’t see the utility” (21), and they believed “it’s going to be longer, it’s going to bother me because I’ll be afraid to hurt the patient” (17).
In addition, procedures using hypnosis often required surgeons to modify their behavior. For instance, using hypnosis meant that the OR needed to be as calm and silent as possible: “She [the surgeon] can’t answer the phone, she can’t talk about other things because it needs to be a little silent” (10). This was the opposite of an OR atmosphere during general anesthesia, which one participant described as a “train station” (27): “Without hypnosis, it’s a little brutal in fact. We will put you to sleep, and everyone will speak, and everyone will talk about their weekend and all that” (6). Similarly, surgeons had to be more attentive in their techniques when anesthesiologists used hypnosis: “It requires some modifications on their part . . . to take out a breast tumor, under general anesthesia it’s I cut, I pull apart, and I take out, whereas here you have to do it more gently. You have to do a local anesthesia, you have to pull apart more delicately. You can’t grumble about the material. You can’t say: ‘Shit it doesn’t work’” (26).
To convince surgeons to accept their own reinvention, anesthesiologists largely relied on means that were important to their own transformation: direct experiences of and relations with clients. Doing so helped anesthesiologists convince certain surgeons of the technique’s efficacy in a non-confrontational manner. 10 As one explained, “We succeeded in awakening curiosity. And then interest, and then rounds [of procedures under hypnosis], in this order. And then it took off right after, very quickly” (31). They were able to do so while avoiding status or power struggles that often arise when interprofessional work configurations shift.
Leveraging adjacent professionals’ direct experiences of clients to convince them of the new practice’s efficacy
To successfully pique the curiosity of surgeons in a manner that did not feel imposed, anesthesiologists ensured that surgeons could experience for themselves the benefits the practice could bring to their work and to patients, before asking the surgeons to change their habits. The most common path to first showing surgeons these benefits was by performing hypnosis in moments when anesthesiologists did not need the surgeon’s consent and that required no modification to the surgeon’s work: “I started little by little, mostly to accompany patients, without modifying the organization . . . and then after surgeons started to see a bit, some started to become interested” (28). For example, anesthesiologists would put patients in a hypnotic trance before administering general anesthesia, particularly for those who were very anxious, so that surgeons could observe the difference: When we manage extremely stressful situations, just with words, it astonishes everyone. Because before in anesthesia, when people are very, very stressed, we give them a sedative and the patient stops his fit. But [with hypnosis] without injecting anything, to be able to calm people that are almost standing up, ready to leave, it convinces people. It astonishes them. Sometimes, there are patients that wake up and are in an enormous state of stress, that have a panic attack and when I arrive and they tell me “he is in pain, we tried everything but he is still in pain” and just with words, people calm down and in the end aren’t in pain anymore, it astonishes them . . . they say “Ah okay she knows how to do something that everyone can’t.” It’s more this that convinced people. It’s like an oil stain [spreading slowly]. (18)
Similarly, anesthesiologists used the technique during procedures not done under general anesthesia (e.g., those using locoregional anesthesia) so that surgeons could directly see the technique’s effect on patients but not have to do anything differently: “I said to the surgeon, ‘I am going to use hypnosis, you do as usual’” (19). In these moments, anesthesiologists often noted that surgeons were taken aback and intrigued as they began to experience differences to their own work: “they clearly tell you that when people are under hypnosis, they see the difference . . . they see that the patient’s muscles don’t react, don’t stretch” (34); “‘But you put him to sleep it’s not possible’ . . . he [the surgeon] was persuaded that I had completely put him to sleep. I said ‘Not at all’ . . . because his abdomen was completely elastic . . . it wasn’t resistant at all” (23).
Anesthesiologists also showcased the technique with patients they could not put to sleep due to medical reasons or in unexpected moments: I changed the view of the [surgical] teams. One day, you know kids that have cystic fibrosis, it’s a horrible disease. It’s kids that have diseased lungs. When they are close to the end of life, we put what’s called a port, something beneath the skin to do infusions through the skin . . . and so, we are doing it using local anesthesia . . . except these patients, when they are at this stage, they can’t lie flat, because it is so difficult for them to breathe in a normal position that they are afraid to lie down . . . and he [the surgeon] installs the patient, and the moment he is going to administer the local anesthesia, he says, “Okay I am going to lay him down.” Except, he lays him down brutally. Panic attack. He says to me: “You need to put him to sleep.” I say “No. I will not put him to sleep because he didn’t have the pre-anesthesia consultation [a legal obligation in France] and it is a severe illness, I will not put him to sleep. If you like, we will try something” . . . I tell the kid “Do you want to do a little exercise that will help you get through this moment” . . . and he went on an extraordinary trip. . . . And he lay down, without a panic attack, without suffocating, without anything . . . and we operated without local anesthesia, and it went really well. He [this surgeon] became my biggest promotor of hypnosis in the hospital. I did so much of it with him, because in a way I tamed him. I led him to understand what hypnosis could bring to him and his patients. (33)
Anesthesiologists highlighted that each chance to show patients’ reactions to surgeons and allow them to directly experience the benefits of hypnosis was vital in persuading the surgeons of the technique’s efficacy: “Each case was a demonstration . . . and it started with one . . . and then it gave ideas to others, and it happened progressively” (20). Much like anesthesiologists, surgeons were convinced by their experiences. By contrast, when surgeons did not directly experience the benefits of the practice on their patients, it was very difficult to convince them of the practice’s efficacy. Trying to show them scientific publications validating the use of hypnosis for pain and anxiety or even trying to persuade them with discourse proved ineffective and tiresome: “Sometimes we exhaust ourselves in explanations, and it’s showing that is efficient” (18). One anesthesiologist explained that for 15 years she had unsuccessfully tried to convince the head of surgery by recounting her experiences and the technique’s advantages. His outlook changed only after he experienced it with his patients: When I started doing this [hypnosis], I went to see the head of surgery at the hospital. It was terrible. He couldn’t stand that I told him what I was doing, it didn’t interest him. Let’s just say, it didn’t go well between me and him. Last year, he asked me to do hypnosis on one of his patients . . . because many people on his team, nurse aides, we had trained them [for hypnosis] and they helped him a lot during his consultations because he is an ear, nose, throat surgeon. So they conduct exams in the upper airway, so in the nose, in the mouth, with people that want to vomit, that can’t stand keeping their mouth open for a long time, that we look at their vocal cords. He could see how it [hypnosis] made his work easier and that he didn’t have to fight against the patients. (43)
Turning to clients to convince adjacent professionals of the new practice’s necessity
To convince surgeons of the need to operate under hypnosis, anesthesiologists also heavily enlisted clients. Patients’ words were often more influential, they explained, than those of anesthesiologists: “Above all what convinced them was the feedback from patients, who were very happy. So what really allowed it to develop, was the really positive feedback” (26). Many anesthesiologists realized that pushing surgeons, from one medical expert to another, to believe in the need for the practice did not work: “At first, I tried to proselytize [like a missionary] and I realized that it was counterproductive . . . on the contrary, it caused conflict, annoyance. It’s useless” (43). Instead, many relied on patients and refrained from pushing surgeons too much themselves: “We explained to them [surgeons] that you’ll see . . . you’ll have feedback [from patients]. But we didn’t say more” (31).
For example, an anesthesiologist who started to use hypnosis during cesarean procedures for women who were extremely stressed explained that she let patients do most of the persuading: “It’s when they [surgeons] go see them in their room and see to what extent they [the patients] are happy, and they are calm. They thank them a lot. So they [surgeons] are happy . . . more supportive to let us do it” (31). Similarly, when anesthesiologists began using hypnosis before administering drugs, sometimes surgeons arrived after the patient was fully asleep, so they did not even see the patient in a hypnotic trance. Instead of trying to promote hypnosis and tell surgeons about its benefits (which many had unsuccessfully tried at first), anesthesiologists would let patients share their satisfaction of having a good experience in the OR during post-op meetings. Surgeons would therefore come to anesthesiologists of their own accord: “We didn’t tell the surgeon. We started like that, and after it was patients that spoke to their surgeons. So the surgeons came to see us. ‘What are you doing? The patients keep telling us that it was great in the OR. It was terrific. We don’t understand’” (27).
Anesthesiologists also heavily relied on patients in getting surgeons to take the big step of first trying to operate under hypnosis without general anesthesia. For instance, when anesthesiologists saw that patients were very anxious about anesthesia during the consultation or that for medical reasons, general anesthesia would be risky, they would approach surgeons. Even though surgeons sometimes “raised their eyes to the sky” (24) at the thought of operating under hypnosis, when anesthesiologists anchored on specific patients’ fears, medical issues, or desires, surgeons were more likely to see the necessity and acquiesce: I remember a patient that had heart disease . . . we needed to remove his thyroid, and the side effects after the general anesthesia were complicated and I said “It’s a shame that we had to put him to sleep for a surgery that could be done under hypnosis and local anesthesia and it would go well.” . . . So they [surgeons] started saying “yeah, maybe.” And then one day there was a patient [during the consultation] who said, “I’m afraid to be put to sleep.” And the surgeon took the opportunity, and we went for it. (17)
Then, patients would tell surgeons that they had a very good memory of their procedure: “And after, when many patients tell them, it’s done, they let us [anesthesiologists] do it” (22). Ultimately, those anesthesiologists who were relatively successful in convincing surgeons were extremely aware that being subtle and taking the “lower position” (52) were crucial in the onboarding.
Adjusting adjacent professionals’ behaviors to allow the new practice
Once surgeons believed in the technique, anesthesiologists were able to change surgeons’ behavior without a battle. During operations under hypnosis, anesthesiologists could become, as one put it, the “conductor of the orchestra” (38) in the room. Anesthesiologists guided surgeons to modify their behavior in order to create a calmer atmosphere in the OR: “I said [to the surgeon] not to directly address the patient, he needed to speak to me if he had something to say to him [the patient] . . . and I would tell him, don’t intervene in the conversation. Everyone stays on their own side” (6).
Another interviewee illustrated how she had to steer the surgeon during an operation: “Once, the surgeon he started talking, saying ‘Ah! Did you feel? I am going to start. I am going to make the incision.’ Well, that’s for sure not going to work. So I said to him ‘You need to be quiet, and I will tell the patient that it will start’” (7). Sometimes they guided surgeons to adapt their techniques and the rhythm with which they worked: “Perhaps you must tell the surgeon from time to time ‘you take a little break’ . . . we restore the comfort [of the patient] and then we continue” (9); “we tell the surgeon, ‘stop what you are doing, try another way’” (15).
As surgeons became motivated to see positive outcomes for their patients and felt proud to succeed at operating under hypnosis, anesthesiologists noted, in the words of one participant, “they play the game well” (31). They adapted their behaviors and accepted the anesthesiologists’ reinvention: “there isn’t a sound in the room . . . everything happens calmly, and it has changed the manner we work . . . the heart surgeon comes, doesn’t say a word . . . surreal” (17). This was a stark contrast to the traditional practice.
Buffering oneself from traditionalist peers’ pushback
Finally, alongside transforming themselves and getting surgeons on board, anesthesiologists practicing hypnosis also had to overcome feelings of isolation and pushback from some of their fellow anesthesiologists. Even though they mostly did the same job as other anesthesiologists (administer pharmaceutical anesthesia), those practicing hypnosis often felt they had a target on their backs marked “hypnosis.” They were generally the first or second anesthesiologist in their division or hospital to adopt the technique and were in the minority by far.
As the technique was outside of the rigorous evidence-based world and for many still carried a connotation of magic, they faced pushback from certain colleagues who found hypnosis “a little ridiculous” (12). They were sometimes teased and categorized as “witches” (6) and “quacks” (14) rather than real doctors: “My colleagues scoffed, they said [Dr. X] is an artist, not a real doctor” (24). While a few noted that some fellow anesthesiologists not interested in practicing hypnosis still respected their choice to adopt the practice, many others adopted an us-versus-them mentality that felt very condescending. 11
Strengthening connections to clients
Strengthening their relational connections to patients was a large part of what helped hypnosis-practicing anesthesiologists to persevere, which also resulted in loosening their connections to others in their profession, particularly their mocking peers. Acknowledging that they now held a different professional outlook, they no longer wanted to belong to the same category as anti-hypnosis colleagues. Instead, they anchored on people outside their profession, which allowed them to effectively shield themselves from pushback they received from their peers.
These anesthesiologists began to strongly distinguish themselves from their anti-hypnosis colleagues vis-à-vis patients: “Amongst anesthesiologists, there are two categories. There are those that are into the technical side and that don’t want at all to speak about humanity. Basically, the faster the patient is asleep, the faster they are in peace. And so it bothers them to see the human side” (24). As they now prioritized aspects such as patient comfort and patient satisfaction and better assisting patients “who didn’t want to be put to sleep, who were scared” (10) or for whom it was extremely complex to administer drugs because of medical reasons, they no longer fully identified with the other side, nor did they want to. For instance, they noted that unlike themselves, some of their colleagues did not care about patients’ comfort, beyond just assuring the patient was not in pain, and that was too bad. Others echoed this, stating they now looked down on their anti-hypnosis colleagues, who “protect themselves behind a scientific shield” (24) and who were not willing to see the real benefits that hypnosis could offer patients.
Similarly, interviewees strongly relied on patients as they redefined what it meant to be a doctor. With this ideal in mind, they considered their anti-hypnosis colleagues as not real doctors: “Our role as a doctor is to have a relationship with the patient and foster the human side [of care]; it’s not just the technical side” (9). Thus, they believed that their colleagues who were skeptical of hypnosis, the ones who preferred to “push drugs” (7), were partially missing out on a key part of being a doctor: “They have forgotten the whole relational aspect. They love the technique, they love machines. They have left behind a large part of who they are, meaning doctors. They aren’t interested in the patient” (8). To them, their anti-hypnosis colleagues became technicians of medicine who were not centered on the patient, which was the opposite of how they considered themselves as hypnosis practitioners: “I feel much more a doctor now [since practicing hypnosis] than ever before” (25).
Distancing from traditionalist peers
Even though their anti-hypnosis colleagues belonged to the same profession, when the anesthesiologists saw them as quite distant from themselves, their pushback (and mockery) became less legitimate in their eyes. Colleagues’ acceptance became less necessary, and their non-acceptance had little impact: “I have nothing left to prove” (6); “I knew that I was in the right . . . in my head, I was saying: ‘Fuck off!’” (24); “I take care of my patients like I want and you do like you want” (43). Patients’ approval took precedent over peers’ approval: “The patients liked it so, I really don’t care what they [anti-hypnosis colleagues] thought. The patients were happy” (25). By focusing on the fact that their patients were very satisfied when undergoing a procedure with hypnosis and “smiling ear to ear” (20) in the recovery room, these anesthesiologists helped protect themselves from mockery: “The others don’t exist anymore. There is only the patient” (22).
When anesthesiologists did not turn outward toward patients (and away from their peers), it became very difficult for them to protect themselves from pushback. For instance, at first many hypnosis-practicing anesthesiologists wanted to believe that everyone in their profession should share the same professional outlook. As one described, when she first learned hypnosis, enchanted by the technique, she went back to her hospital and told her anesthesiologist colleagues, “you need to get trained in hypnosis to become human,” with the goal to convert the skeptics. She quickly gave up on this mindset as major hostilities arose: “The other colleagues were shocked and said, ‘You do not have the monopoly over humanity because you practice hypnosis.’” Instead, she mentally separated herself from these peers and shifted her anchor to patients: “We [anesthesiologist colleagues] each have our priorities. My priority now, is to be there for the patient” (43).
Discussion
These anesthesiologists who practiced hypnosis were deeply socialized in a scientific, evidence-based world. However, they voluntarily adopted a seemingly antithetical practice, which had profound implications for their work. They had no strong external pressure to adopt it, and thus they could not anchor on such pressure to justify to themselves and others a shift in their core professional tenets and work. These anesthesiologists also generally did not turn to peers in their profession as their main source of guidance in this reinvention. Even though hypnosis had been recognized as a valid anesthesia technique by their professional association, the professionals with whom they interacted on a daily basis (other anesthesiologists and surgeons) generally did not embrace its use. What largely helped these anesthesiologists in this reinvention was turning inward to oneself—focusing on their own direct experiences of clients—as well as turning outward to clients—relying on relations with those outside their profession. By doing so, they underwent an internal transformation in which they saw a justified reason to reframe their professional core tenet (for themselves), convinced people in adjacent professions to accept their reinventions, and buffered themselves from the pushback of traditionalist peers. Figure 1 summarizes this pathway of voluntarily reinventing one’s work.
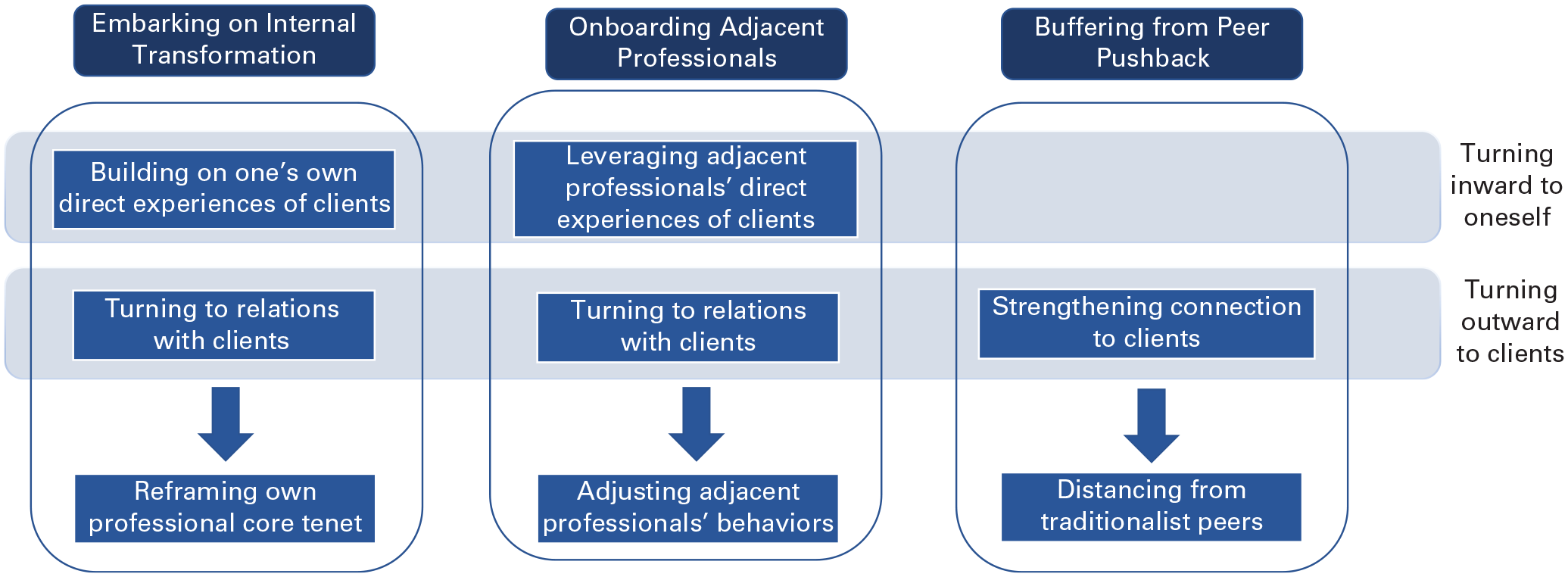
Pathway to a Voluntary Reinvention of One’s Professional Work
Professionals’ Reinventions
First, our study contributes to the literature on professional reinventions by unpacking how some individuals who are deeply embedded in their professional cultures may voluntarily reinvent their work. Given the tremendous difficulty that professionals face in changing their practices, most scholarship has focused on how involuntary reinventions occur when external pressure is the chief impetus for such changes. In these cases, the main pathways to reinventions involve turning to peers in the profession to navigate these changes, including justifying shifts in core tenets, getting others on board, and dealing with resistance (e.g., Barley, 1986; Kalev, Dobbin, and Kelly, 2006; Kellogg, 2009; Cohen, 2013; Nelson and Irwin, 2014; Kahl, King, and Liegel, 2016; Bechky, 2020). We identify an alternate pathway in the absence of external pressure, in which some professionals turn inward to themselves and outward to clients to navigate their reinvention. We argue that this combination of direct experiences and connection to clients constitutes a powerful engine of such reinvention.
Our study spotlights how this reinvention can occur even when individuals do not a priori hold strong preordained personal beliefs about the reinvention. The limited empirical research that has explored how voluntary reinventions occur has tended to assume that people reinvent their work because they already feel strongly about the need to change (McCarthy and Kelty, 2010; Howard-Grenville et al., 2017). In other words, past research would likely predict that these anesthesiologists would not reinvent because they did not already feel strongly about the need for hypnosis in their repertoire or strongly question their profession’s core tenets, and they faced no strong pressure (neither external nor from peers) to adopt the practice. Here, we show a pathway to professional reinvention even in the apparent absence of initial deeply held beliefs.
We suspect that the dynamics of turning inward and outward can help to explain other voluntary reinventions in which people did not appear to have a strong desire to reinvent. For instance, army officers who shifted their work from waging wars to building states perhaps underwent a transformation when they directly experienced the effects of warfare on citizens of war-stricken countries and turned to citizens in their assessments of how to best help them. Similarly, some district attorneys who shifted their work from incarcerating criminals to decriminalization might have changed their outlook when they directly experienced the impact of trials on criminals and focused on criminals’ feedback. Future research could explore the extent to which turning inward and/or outward might fuel other professional reinventions and the relative weight of these two mechanisms in these processes.
Second, our findings also show how only some members of a profession can undertake such a reinvention before potentially trying to change the entire profession. While studies on voluntary reinventions have focused on the moments in which those who have chosen to voluntarily reinvent decide to convince peers of the change (McCarthy and Kelty, 2010; Howard-Grenville et al., 2017) and to institutionalize it (Muzio, Brock, and Suddaby, 2013), our study offers insight into a moment before these things may happen. The challenge is not (potentially yet) to convince peers but, rather, to have the courage to reinvent one’s own work when the reinvention is not widely accepted in the field as well as to shield oneself from peers’ pushback. Turning inward and outward allowed professionals to distance themselves from peers who did not support their reinvention and to no longer need or care about their acceptance. Without such shielding, it was extremely difficult for these professionals to persevere. For instance, one anesthesiologist who actively sought acceptance from her anti-hypnosis peers ended up leaving her hospital. That said, future research could explore the problem of too much distancing from peers. For example, if a professional can completely distance from peers and forge their own pathway to change, this could result in the fractioning of a profession whereby break lines appear and uniform standards disappear (Strauss, 1975; Abbott, 2001; Fisk, 2016).
Our study therefore highlights the pacing and sequencing of changes within professions by opening up the possibility that, alongside a more collective (social movement) pathway to change (McInerney, 2014; Munir, Ansari, and Brown, 2021), there could also be more individual paths to reinvention. 12 In these cases, reinventions may happen in a more piecemeal manner whereby some but not all professionals reframe core tenets, as opposed to a sweeping change across a profession. The extent to which hypnosis will become mainstream in the anesthesiology profession or how much (or even whether) hypnosis-practicing anesthesiologists will actively try to make it so is still unclear. For the moment, however, this does not seem to be their main goal.
Third, our findings also reveal how professionals may onboard adjacent professionals to accept their reinventions, without the expected jurisdictional battles. We highlight that building on adjacent professionals’ own experience of clients and relying on their client relations might help to avoid potential conflicts. Numerous studies have shown that changes in the status quo often result in heated interprofessional battles that sometimes hinder or significantly prolong the adoption of new ways of working. This is particularly prevalent when professional groups’ status and power are at play (e.g., Abbott, 1988; Karunakaran, 2022). In our study, practicing hypnosis brought anesthesiologists on a more equal footing to surgeons, who have the highest status in the OR team hierarchy; anesthesiologists took a more central role during procedures and were considered more significant figures in the eyes of patients. For the most part, conflicts remained civil. Many surgeons eventually accepted these anesthesiologists’ reinvention and worked collaboratively with a technique that brought anesthesiologists into their spotlight. Building on aspects that surgeons valued (their experiences and their patients) perhaps made this change feel less like a battle for status or power. Future research could explore how more heavily building on direct experiences of clients and/or enlisting clients’ help in shifting the status quo may dampen conflicts across various settings, such as those between firefighters and policeman (Karunakaran, 2019) or doctors and lawyers (Kellogg, 2014).
Our analysis also suggests that one way for professionals to gain new standing vis-à-vis adjacent professionals may be through the gradual inclusion of new tasks into their jurisdictional portfolio (Cohen, 2013). As we explained, anesthesiologists often gradually added hypnosis to their portfolio, testing it first alone with a patient, then perhaps in the presence of a nurse, and finally with surgeons. In addition, anesthesiologists could blend this new practice into their portfolio since they could revert, if needed, to using pharmaceutical anesthesia. Over time, proponents of medical hypnosis have given increasing jurisdictional prominence (Chown, 2020) to this task relative to others in their portfolios. This strategy has allowed them to increase their standing vis-à-vis surgeons gradually but surely, while preempting extremely forceful pushback from them. By selectively dialing up and down the frequency of tasks deemed too novel, they illustrate a little-explored way of non-confrontationally gaining standing.
The Role of Clients in Professionals’ Reinventions
Our study also contributes in at least two ways to research on the varied role of clients in professional work. First, our findings demonstrate that clients can profoundly impact how professionals conceptualize and navigate their work. The professions literature has traditionally assumed that the pillar of what guides professional work comes largely from within the profession (Freidson, 1986; Abbott, 1988); clients have generally been conceptualized as a far cry from being key relational partners to professionals, and the most prestigious professions look down upon client interactions, hive off this lower-status population, and consider client assessments of their competence to be untrustworthy (Hughes, 1958; Abbott, 1988; Huising, 2015). However, more-recent scholarship has noted the role of non-peers in shaping professionals’ work (Wynne, 1989; Epstein, 1996; Mol, 2008; Turco, 2012; Eyal, 2013; Huising, 2015; Galperin, 2020; DiBenigno, 2022; Chan and Hedden, 2023). This research shows how professionals adapt their work based on clients so they can uphold their professional mandate; in these cases, client interactions do not lead people to reassess their professional mandate and outlook. We thus add to this research by showing that clients can not only shape but also profoundly transform professionals’ work.
A key dynamic in these anesthesiologists’ reinvention lay outside the professional realm. While they had the support of other hypnosis-practicing anesthesiologists (via trainings and medical hypnosis conferences), to overcome the daily challenges of their reinvention they did not turn to these peers for the most part. Instead, turning to the words and feedback of patients in part allowed them to redefine their outlook of what constituted a good anesthesiologist (i.e., one who connected with patients). While not all professions involve regular interaction with clients, most professionals do have this relational aspect to their work (Barley, 2020). Future research could further unpack other reinventions that do not involve clients.
Second, our findings highlight the role of direct experiences with clients in loosening deeply embedded norms. Most past research has explored how direct experiences can shape how people conceptualize work practices when they are new to the job or in settings in which strong norms do not yet exist (e.g., de Rond, Lok, and Marrison, 2022; Sheehan, 2022); in other words, this research demonstrates how direct experiences instill deeply set beliefs and norms. Here, we show how direct experiences with clients can also help to loosen the hold of deeply embedded norms. These anesthesiologists began to question a core tenet of the profession, rigorous evidence-based medicine as the only legitimate evidence, after experiencing benefits with patients beyond what they were accustomed to. Future studies could further explore which types of direct experiences may be more likely to loosen deeply embedded professional norms. Perhaps direct experiences with clients that invoke a professional’s latent values or idealized notions (DiBenigno, 2022) may be particularly powerful.
Boundary Conditions and Limitations
We recognize various boundary conditions to our findings of turning inward and outward as a pathway to voluntary reinventions. On one hand, certain individual characteristics of professionals likely come into play. 13 Obviously, those who did practice hypnosis might differ from those who did not, but our research design did not seek to explain who did and did not embark on this reinvention. Instead, it sought to uncover how those who did so went about their journey. It is important to note that while experiencing the practice of hypnosis ended up having a profound and transformative impact on how anesthesiologists related to their work, most did not know beforehand that learning hypnosis would result in this reinvention. Our framework therefore likely captures the seeds of a transformation, even among initial non-believers. On the other hand, we would also expect certain characteristics of the novel practice or innovation to shape the likelihood of such voluntary reinventions. Hypnosis was a practice that these anesthesiologists found effective for clients but also one that greatly enhanced the meaning of their work. We would expect that such voluntary reinventions would perhaps be less likely for practices that were judged risky or led to greater alienation from work. For instance, if an AI robot was used to hypnotize the patient while the professional supervised, even if it were equally effective, anesthesiologists’ motivations to reinvent might be dampened.
Finally, certain characteristics of the profession may also facilitate the mechanisms of turning inward and outward. We would expect such dynamics to be particularly powerful in professions that involve contact with and direct feedback from clients, customers, or other audiences. As these anesthesiologists belonged to a profession in which they were constantly in contact with their patients, they had ample opportunities to directly experience patient benefits and receive patient feedback. (Surgeons also belonged to a profession with these characteristics, which we suspect helped to get them on board via turning inward and outward.) Moreover, perhaps another key characteristic of the profession regarding the adjacent profession whose agreement was crucial to these anesthesiologists’ reinvention was that the anesthesiologists’ jurisdiction did not overlap with those of surgeons. While this reinvention did shift some of the power dynamics between surgeons and anesthesiologists, it did not shift surgeons’ jurisdictions. We would expect such voluntary reinventions requiring the acceptance of adjacent professions to be more successful when there is minimal overlap in jurisdictions.
A limitation to any study relying primarily on interviews is the potential risk of retrospective bias; some of these anesthesiologists were reflecting on motivations and interpretations from years ago, so their accounts could be somewhat distorted. 14 However, we suspect the likelihood of such bias to be minimal. Indeed, the anesthesiologists’ initial encounters with the practice were moments that profoundly marked them, and many vividly recalled specific details (e.g., where they took their first patients during hypnosis, their patients’ words and reactions). Thus, they were not recalling fuzzy memories. In addition, even though the broader perception of hypnosis in the field has changed over time, the journeys of those who adopted hypnosis years ago versus those who did so more recently (including the ones we observed during training sessions) were quite similar; both strongly anchored on their own direct experiences of and relations with patients. 15
Conclusion
Recent debates on professionals’ roles in solving societal problems (Nichols, 2017; Eyal, 2019; Gorman and Vallas, 2020) have spotlighted the need for some professions to reinvent their work to address increasingly critical social issues, such as climate change, social justice issues, and more. While our framework of turning inward to oneself and outward to clients does not guarantee a change to a profession as a whole, it does explain how some professionals can voluntarily embark on a reinvention of work and potentially seed movements for broader change. In that sense, it helps to account for how momentum can begin and how individual professionals’ rebooting can emerge. Without a clear grasp of these initial dynamics, our knowledge of how change happens in professions—among the most robust institutions—will remain at best incomplete.
Supplemental Material
sj-pdf-1-asq-10.1177_00018392231190300 – Supplemental material for Rebooting One’s Professional Work: The Case of French Anesthesiologists Using Hypnosis
Supplemental material, sj-pdf-1-asq-10.1177_00018392231190300 for Rebooting One’s Professional Work: The Case of French Anesthesiologists Using Hypnosis by Nishani Bourmault and Michel Anteby in Administrative Science Quarterly
Footnotes
Acknowledgements
We thank all the anesthesiologists and other medical professionals who generously shared their time with us. We are particularly grateful to Doctors Jean-Marc Benhaiem, Franck Bernard, Emmanuel Boselli, Michael Deyaert, and Delphine Provost for their trust and support. We also thank Damon Phillips and our reviewers for their constructive guidance as well as Ashleigh Imus and Joan Friedman for their expert editing work. Finally, we acknowledge Curtis Chan, Julia DiBenigno, Leroy Gonsalves, and Audrey Holm for their valuable feedback on this manuscript, as well as seminar and conference participants at AOM, EGOS, Harvard’s Culture & Social Analysis Workshop, NEOMA, Transitions Research Group, UBC’s Sauder School of Business, and Wharton’s People & Organizations Conference for their insights.
1
Note that not all anesthesiologists who are trained end up practicing hypnosis.
2
Anesthesiologists in France go through 11 to 13 years of medical training.
3
Another type of hypnosis is conversational hypnosis, whereby the patient is not fully disassociated from their current environment.
4
We therefore conducted a theory elaboration exercise in which we used past literature as a springboard to direct our data collection “in the service of discovering” new and, we hoped, broader theory (Strauss, 1987: 306). We analyzed our data from an abductive perspective (Timmermans and Tavory, 2012). Abductive approaches aim to develop theory based on surprising findings in light of existing literature.
5
Examples of dangerous drugs include pentothal and the muscle relaxant vecuronium, also used as a drug cocktail in the execution of some prisoners on death row in the United States.
6
If the anesthesiologist leaves the room, a nurse specialized in anesthesiology remains there.
7
A head anesthesiologist trainer at one of the main medical hypnosis training centers estimated that approximately 70 percent of anesthesiologists who went through the program incorporated some hypnosis into their work (based on surveys the center conducted over a year after attendees completed the program).
8
A few younger anesthesiologists we interviewed attended the training with a more purposeful intent of wanting to adopt the practice. They had been directly exposed to the technique during their residency while working alongside senior colleagues who practiced hypnosis. Most participants were more seasoned and took these courses as part of their requirements to complete continuing medical education credits, which they could obtain by taking a wide range of course offerings.
9
We use “onboard” to convey the idea of bringing someone along on a journey, as our discussion in this section implies. Surgeons not only had to be convinced of hypnosis as a practice, but they also had to adjust their own behaviors to allow anesthesiologists to practice hypnosis on patients during surgery. “Onboard” in our context thus does not necessarily mean that adjacent professionals themselves fully adopted the practice of hypnosis.
10
Anesthesiologists generally noted that they did not try to indiscriminately onboard all surgeons. Instead, they focused on surgeons who they felt were more centered on the patient and whose behavior in the OR was compatible with formal hypnosis (e.g., surgeons who did not yell).
11
When anesthesiologists want to practice hypnosis, they need the consent only of surgeons (when hypnosis replaces pharmaceutical anesthesia) and not of fellow anesthesiologists. Thus, interviewees noted they did not really try convincing other anesthesiologists to adopt the practice.
12
Unlike the job-crafting literature (Wrzesniewski and Dutton, 2001) that explores how individuals voluntarily make changes to their work practices without significantly challenging professionals’ core cultural tenets, our study focuses on how individuals voluntarily embrace practices that fundamentally change and expand professionals' core beliefs.
13
The anesthesiologists who enrolled in hypnosis training were generally bored in their current routine and, at a minimum, curious about the technique, so they were likely open to a change (albeit not convinced). Thus, we suspect that such voluntary reinventions might prove more likely for professionals who are somewhat weary of their current tasks and open to some novelty.
14
For insightful discussions on biases associated with interviews, see Jerolmack and Khan (2014), Lamont and Swidler (2014), Winchester and Green (2019), and ![]() : 209).
: 209).
15
The main difference we identified was that the degree of the challenges they encountered (e.g., believing in the practice, reluctance of surgeons, mockery from their anesthesiologist peers) was somewhat stronger for those who started practicing hypnosis years ago, as it was even more esoteric a practice than it is today. However, the mechanisms they used to overcome these challenges and reinvent their work remained consistent.
Authors’ Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.