
Abstract
This paper develops grounded theory to understand how and when experts in lower-power peripheral roles can develop influential relationships with higher-power line managers in core functions to regularly elicit their cooperation. I use data from an ethnographic study of experts in peripheral roles—mental health professionals hired by the U.S. Army to provide rehabilitative services to active-duty soldiers suffering from conditions such as post-traumatic stress disorder (PTSD)—and the line managers in core functions they depended on for their soldier-care recommendations to be followed—their soldiers’ direct commanders. I analyze relational histories of 56 commander–provider dyads and detail a three-phase process model I refer to as “rapid relationality.” Through the process of rapid relationality, mental health professionals capitalized on short windows of opportunity to quickly develop influential relationships with commanders, despite lacking formal authority over them, before a series of minor conflicts or a major conflict threatened their burgeoning influence. My analysis suggests it is not only what peripheral experts do that allows them to elicit cooperation from line managers but also when and how quickly they do it that matters. Speed and taking early action are important because experts cannot predict when conflict will occur and hence may have short initial windows of opportunity for establishing an influential relationship. I further find that some experts have fewer tactics available to them or must use more time-consuming and energy-intensive tactics than others to achieve the same relational influence based on their personal characteristics (e.g., gender). As a result, it may be harder for some experts to achieve relational influence before their window of opportunity closes.
Keywords
In this age of experts, organizations regularly hire professionals with specialized expertise to solve pressing problems, ranging from improving sustainability to increasing diversity and workplace safety, that they cannot solve internally with their core workforce (Barley and Tolbert, 1991; Brint, 1996; Gorman and Sandefur, 2011; Kellogg, 2014). Even when organizational leaders support their work, however, these experts’ effectiveness often depends on gaining cooperation from line managers in core functions of the organization who may ignore or resist their recommendations with relative impunity (e.g., Kalev, Dobbin, and Kelly, 2006; Heinze and Weber, 2015; Huising, 2015; Valentine, 2018). Such experts typically occupy peripheral roles in the organization rather than core roles considered central to the organization’s primary mission (Mintzberg, 1979; Sapir, Drori, and Ellis, 2016). Line managers may perceive experts’ attempts to change their behavior as impeding their ability to achieve the core goals on which their performance is evaluated—hence threatening their autonomy (e.g., Meyer, 1968). These experts also generally lack formal authority over line managers and cannot simply issue orders, because they typically do not control key resources such as line managers’ budgets or performance evaluations (e.g., Weber, 1924, 1946; Dalton, 1950).
While the challenges facing peripheral experts are well documented (e.g., Dalton, 1950; Allen, 1955; Browne and Golembiewski, 1974; Edelman et al., 1991; Perlow and Kelly, 2014), there is surprisingly little scholarship on when and how they can successfully gain line managers’ support. Existing work addressing the general problem of low-power influence, however, suggests possible solutions. Organizational behavior scholars have examined how lower-power people, typically middle managers, sell issues such as gender equity and sustainability to top managers by using their insiders’ understanding of their organizational contexts to implement strategic issue-selling moves (e.g., Ashford et al., 1998; Dutton et al., 2001; Howard-Grenville, 2007). Occupational sociologists find that lower-power occupational groups such as technicians can sometimes elicit cooperation from higher-power groups such as physicians by making the higher-power group dependent on them, for instance by developing superior technical knowledge of the work (e.g., Pfeffer, 1992; Black, Carlile, and Repenning, 2004; Kellogg, 2018). And industrial-organizational psychologists have identified strategic tactics subordinates use to engage in upward influence with supervisors or peers at work, such as ingratiation, consultation, or rational persuasion (e.g., Schilit and Locke, 1982; Yukl and Falbe, 1990).
This scholarship provides compelling insights into how low-power groups can exert influence, but expert occupational groups in peripheral roles in organizations may face additional barriers and require a novel set of tactics and processes to overcome them. Peripheral experts often lack a relational foundation for influence with line managers—a foundation based on access, knowledge, and trust. Unlike most of the low-power influencers studied in the existing literature, peripheral experts may not have access to line managers because of their peripheral position in the organization’s social and work network, such that line managers may ignore or rebuff efforts even to contact them (e.g., Allen, 1955). Because peripheral experts do not perform the core work of the organization, they may lack knowledge of line managers’ work and values, which is necessary for strategically selling issues and developing dependency relations with them (e.g., Barley, 1986; Bansal, 2003; Sonenshein, 2006; Howard-Grenville, 2007). And they may have difficulty establishing trust with line managers because their expertise is not valued, their recommendations may provoke conflict by threatening line managers’ authority and autonomy (e.g., Meyer, 1968), and they often lack shared demographic characteristics with line managers (e.g., Dalton, 1950; DiBenigno and Kellogg, 2014).
Scholarship on experts in peripheral or staff roles in organizations has extensively documented the resistance they face from line managers and has largely accepted the inevitability of conflict that is often managed in suboptimal ways, such as when experts are ignored or coopted by line managers (e.g., Dalton, 1950; Edelman et al., 1991; Briscoe, Maxwell, and Temin, 2005). Meyer (1968) proposed raising the status of peripheral experts so they are not dominated by line managers (i.e., “strategic HR”), but this strategy often fails in practice (Sandholtz, Chung, and Waisberg, 2019), as line managers refuse to treat experts in peripheral roles as equals (Sandholtz and Burrows, 2016). Given the rise of professional groups working in organizations (e.g., Anteby, Chan, and DiBenigno, 2016), it is imperative to determine how peripheral experts can elicit cooperation from line managers so organizations can benefit from their expertise.
Using data from an ethnographic study of two groups—mental health professionals (experts in peripheral roles) hired by the U.S. Army to provide rehabilitative services to active-duty soldiers, and those soldiers’ direct commanders (line managers)—I employ one of the first dyadic-level, ethnographic datasets of expert–line manager pairs that attends to the same experts working with multiple line managers to examine how and when experts in lower-power peripheral roles can develop influential relationships with higher-power line managers to regularly elicit their cooperation. This paper aims to enhance our understanding of expert occupational groups working in organizations, influence and issue-selling by low-power groups, and relationality in organizations.
Influence by Low-power Groups in Organizations
While researchers have not yet identified how peripheral experts can elicit cooperation from higher-power line managers, scholarship on low-power groups in organizations may provide some guidance. First, research on issue-selling in organizations demonstrates how lower-power people, typically middle managers, can use their insiders’ understanding of their organizational context to strategically sell issues to top managers when the conditions are favorable and pose minimal threat to their reputation and image (e.g., Ashford et al., 1998; Dutton et al., 2001; Dutton et al., 2002; Edmondson, 2003; Ashford and Barton, 2007; Detert and Edmondson, 2011). When issue sellers assess the context as favorable, they can use three types of moves to gain the attention and support of their higher-power targets: “packaging moves” to strategically shape their target’s impression of the issue content (e.g., strategic framing); “involvement moves” to strategically select who to involve and target in issue-selling efforts; and “process moves” to adjust the formality of the tactics used, such as first informally raising an issue before using more formal channels (Dutton and Ashford, 1993; Dutton et al., 2001). Of particular importance is issue sellers’ understanding of their organizational context so they can craft issues and use moves that resonate with the dominant schemas, values, and meaning systems of their higher-power targets, even when influencers privately hold alternative motives for supporting an issue (e.g., Howard-Grenville and Hoffman, 2003; Sonenshein, 2006; Howard-Grenville, 2007). Peripheral experts, however, may not have knowledge of their targeted line managers’ work and values because these experts are removed from the organization’s core work. And while the issue-selling literature finds that supportive organizational contexts are important for selling issues, peripheral experts often have no choice but to sell issues in an unfavorable context since their full-time job is to represent these issues.
Second, scholars of work and occupations have found that lower-power occupational groups in organizations (e.g., nurses) can sometimes elicit cooperation from higher-power groups (e.g., physicians) by making the high-power groups dependent on them (Emerson, 1962; Mechanic, 1962; Pfeffer, 1992; Kellogg, 2018), such as by becoming more central to the workflow (Allen, 1997), developing superior skills or knowledge (Hughes, 1988; Barley and Bechky, 1994; Black, Carlile, and Repenning, 2004), or controlling objects key for work completion (Crozier, 1964; Bechky, 2003; Zuzul, 2018). In all these cases, however, low-power occupational group members were also part of the core line function of the organization (unlike peripheral experts) and were able to use their proximity to the core to gain access to and knowledge of their influence targets. Low-power groups were also able to gain trust by establishing an exchange relationship in which they used their superior centrality/knowledge/control in relation to core work to exert greater influence.
Finally, extensive scholarship in industrial-organizational psychology has identified factors affecting the success of upward influence attempts (e.g., Mowday, Steers, and Porter, 1979; Schilit and Locke, 1982), finding that “soft tactics” such as ingratiation or eliciting reciprocity are generally more effective for those with low power than “hard tactics” such as upward appeals to supervisors, assertiveness, and coalition building (e.g., Kipnis, Schmidt, and Wilkinson, 1980; Ansari and Kapoor, 1987; Yukl and Falbe, 1990; Bruins, 1999). Subordinates in these studies, however, generally had access to and knowledge of their targets since their targets were their direct supervisors or colleagues, and they generally had the opportunity to gain their targets’ trust by proving themselves in everyday work.
The low-power groups examined in prior research share certain barriers to influence facing peripheral experts: lacking formal authority over their influence targets and advocating for issues or changes that the targets may find unimportant or threatening to their authority or agendas. But peripheral experts often face additional barriers from lacking a relational foundation for influence that may require a distinctive set of tactics to overcome. Extant scholarship has largely assumed that lower-power influencers and their higher-power targets have a basic level of relationality such that influencers have access to their targets, knowledge of them, and a way to establish trust with them. Prior work has primarily focused on cases in which the two parties already have an existing relationship or can fairly easily establish one—those studied are typically organizational insiders with social network connections to their targets as in the case of middle manager issue-sellers (e.g., Dutton et al., 2001), they are members of the same core function in the case of low-power occupational groups (e.g., Barley, 1986), or they are part of the same organizational function in supervisor–subordinate or peer relations (e.g., Yukl, Guinan, and Sottolano, 1995). Such relationships are important resources for influence (e.g., Dutton et al., 2001; Casciaro and Lobo, 2008). For example, Howard-Grenville (2007) found that members of a lower-power internal environmental group were successful at influencing the higher-power core technology group only after new members joined the environmental experts’ group who were former members of the technology group and had existing relationships they could leverage for influence. A baseline relational foundation may be an important precondition for influence that facilitates influencers’ success at strategically deploying issue-selling moves, creating a dependency relation of reciprocity from regular contact during daily core work encounters, or choosing from a series of influence tactics to deploy.
But a relational foundation for influence may not come easily for peripheral experts. Given their location outside line managers’ social and work networks, peripheral experts may struggle even to gain access to line managers, who may simply ignore the experts’ attempts to contact them. Peripheral experts’ assignment to functions removed from core work may impede the development of contextualized knowledge of line managers and their work that prior scholars have found necessary for strategically crafting and framing successful influence attempts and developing dependency relations (e.g., Bansal, 2003; Black, Carlile, and Repenning, 2004; Howard-Grenville, 2007). And peripheral experts may find it more difficult to establish trust with line managers because they cannot prove their worth to their targets through the superior execution of core work. Experts’ skills are often not valued or understood by line managers, and they may be seen as interfering with line managers’ ability to achieve core goals. In addition, trust building may be hampered if peripheral experts lack similarities with line managers in terms of department affiliations, gender, or age, for example; without such similarities, it is more difficult to establish liking and trust (e.g., Dalton, 1950; DiBenigno and Kellogg, 2014). For peripheral experts, cultivating a basic level of relationality with line managers may be difficult to accomplish and require a novel set of tactics. To understand how peripheral experts might build a relational foundation on which to influence higher-power line managers, I turn to insights from the literatures on relationality and temporal dynamics.
Relationality and Temporality in Organizations
Management research and the social sciences more broadly have taken a relational turn in recent decades, understanding individual action as embedded in a web of social relations (e.g., Emirbayer, 1997; Bradbury and Lichtenstein, 2000; Huising and Silbey, 2011) and recognizing one’s relational or social capital as an important source of power and determinant of success in organizational life (e.g., Granovetter, 1973; Coleman, 1988; Fernandez, Castilla, and Moore, 2000; Reagans, Zuckerman, and McEvily, 2004). Although we understand what characterizes relationships, such as rapport and trust (e.g., Kramer and Tyler, 1996), we know much less about the process through which relationships are formed in organizations, especially strategic or instrumental work relationships. Extensive research on social networks has identified numerous variables that affect the likelihood of relationship or tie formation, such as demographic similarity, cultural matching, proximity, and liking (e.g., McPherson, Smith-Lovin, and Cook, 2001; Rivera, Soderstrom, and Uzzi, 2010; Rivera, 2012; Casciaro et al., 2015). And management research has made strides toward understanding the importance of relationships for achieving positive organizational outcomes (Casciaro and Lobo, 2008; Canales and Greenberg, 2015) such as relational coordination (Gittell, 2001, 2006). This work has unearthed important indicators of relationship quality, such as mutual respect and frequent communication, but it has not detailed the process through which beneficial relationships are formed. Scholarship on high-quality connections has taken a more process-based view of relationship formation at work (e.g., Dutton and Ragins, 2017) but has primarily examined relationships in which a relational foundation already exists (e.g., managers and their subordinates), unlike the case of peripheral experts.
One notable exception is work by Huising (2015), who found that experts can use “relational authority” with organizational members resistant to their recommendations by entering their workspaces and performing lower-status scut work (e.g., Ph.D.s changing lightbulbs in scientific laboratories). But even though Huising’s low-power experts formed relationships with line managers, this study did not explore how such relationships were built and maintained given the power asymmetry between them. And to my knowledge, no one has studied dyadic relationships between peripheral experts and line managers. Typically, only one group is studied (e.g., safety officers in Daudigeos, 2013; health physicists in Huising, 2015) because of the difficulty of securing dyadic data that attend to the point of view of both the line managers and peripheral experts and map their relations over time. Without data from both sides of the relationship, it is not possible to understand both which tactics influencers use and which tactics influence targets. And without mapping relations over time, it is not possible to understand timing and sequencing effects.
Temporality scholars remind us of the value of temporal sequencing: it may not only be what you do that matters, but when you do it (e.g., Perlow, 1999; Ancona, Okhuysen, and Perlow, 2001; Okhuysen and Bechky, 2009; Fisher, Pillemer, and Amabile, 2018). One temporal dimension that may be particularly important in the context of peripheral-expert relationship building is that of “windows of opportunity” (e.g., Tyre and Orlikowski, 1994). Temporality scholars have noted that critical windows of opportunity exist in many organizational domains, such as teamwork processes and technology adoptions. There is often a short initial period of time in which experimentation and multiple options for action are available, after which the window closes as interaction patterns solidify and become difficult to change (Weick, 1990; Gersick, 1994; Tyre and Orlikowski, 1994; Albert, 2013). Because peripheral experts often begin their encounters with line managers as discredited, and their recommendations are often viewed as provoking conflict, they may have a limited window of time to build a relational foundation to influence line managers before inevitable conflicts occur and doom the relationship. This literature also highlights the importance of taking early action since first impressions are quick to form and hard to change (e.g., Higgins, Rholes, and Jones, 1977).
Methods
Research Context
During the wars in Iraq and Afghanistan, the U.S. Army encountered an unexpected increase in soldiers’ mental health problems, especially suicide and post-traumatic stress disorder (Department of Defense Task Force on Mental Health, 2007; Tanielian and Jaycox, 2008; de Rond and Lok, 2016). Between 2001 and 2011, mental health diagnoses across the military increased 65 percent (U.S. Armed Forces Surveillance Report, 2012). Of all the branches of the military, the army suffered the greatest increase in suicides and other mental health problems (Institute of Medicine, 2014). In response, Congress and the American public demanded the “invisible wounds” of mental illness be treated the same as physical injuries—by providing rehabilitative care services.
Prior to these wars, army mental health services were limited, and many soldiers hid their problems until they broke down and were then discharged from the army rather than sent to professional care to be rehabilitated and retained. Mental healthcare usage was strongly stigmatized as a sign of weakness in a hyper-masculine context in which soldiers are regularly evaluated on their physical and mental toughness (e.g., Vogt, 2011). In contrast, active-duty U.S. soldiers are now offered some of the most extensive rehabilitative mental healthcare services in the world, such as same-day walk-in access to mental health specialists, and they have the opportunity to recover from a mental health problem while remaining in the army just as if they had a physical injury, such as a broken bone. Billions of dollars have been invested into providing these services, including to hire hundreds of mental health professionals to provide this care to soldiers (Hoge et al., 2015; Srinivasan, DiBenigno, and Carroll, 2017).
To deliver these rehabilitative clinical care services, the army built a dedicated outpatient mental health clinic for every brigade, and in some brigades it assigned a mental health provider to serve soldiers in one or two units exclusively, working with ~6–12 commanders and their subunits. Online Appendix A (http://journals.sagepub.com/doi/suppl/10.1177/0001839219827006) provides a visual representation of this structure. Army posts generally comprise three to six brigades located in different geographic areas, with approximately 3,600 soldiers in each brigade. Units within brigades comprise approximately 600 soldiers and are further broken into subunits of approximately 100 soldiers, each led by a different commander.
For soldiers to fully benefit from these extensive new services, they required the support of their direct supervisor—their subunit or unit commander (referred to simply as “commander” hereafter). Commanders could override and reject duty-limiting treatment recommendations made by mental health providers in support of their soldiers’ recoveries, such as recommendations to sit out a training exercise or deployment, restrict access to weapons, escort a soldier to an appointment, or adjust a soldier’s work schedule or duties.
Data Collection
I collected data between 2012 and 2015. For the first 12 months I did preliminary fieldwork, acquainting myself with the army context by serving as a research assistant on an interdisciplinary research team that conducted over 130 formal and informal interviews and dozens of focus groups with mental health providers, commanders, soldiers, chaplains, and other medical and command stakeholders at seven U.S. Army posts. I spent the next 18 months examining how mental health professionals—as members of the lower-power peripheral medical function of the organization—regularly elicited support from the commander line managers in the core war-fighting function of the organization, whose cooperation they needed to ensure their soldiers could recover from the mental health conditions they were receiving treatment for. I focused data collection on 18 mental health clinics and the 18 brigades they served across four U.S. Army posts.
As predicted by the literature, given their peripherality and lack of authority, the majority of mental health providers failed to build influential relationships with commanders. In 10 of the 18 clinics studied, both providers and commanders reported that commanders regularly did not follow providers’ recommendations for soldiers’ care. But I was surprised to discover that some providers were regularly building highly influential relationships with commanders in the other eight clinics. Given the empirical and theoretical puzzle posed by this unlikely success, I focused my analysis on data from these eight clinics, where I spent over 600 hours total on site and conducted an additional 183 in-depth interviews. These formal interviews were supplemented with observation, informal interviews, and participation in social gatherings.
Providers in these eight clinics were assigned to work exclusively with a small set of commanders and their subunits (~6–12 commanders). In the other ten clinics, providers were not assigned to specific commanders and worked with dozens of commanders, so they had few opportunities to develop familiarity, let alone influential relationships. In prior work, I showed how the organizational structure of assigning providers to specific commanders while working surrounded by each group’s professional colleagues helped alleviate intergroup goal and identity conflict by enabling personalized relationships between groups while preventing cooptation. But even within the more successful clinic structures with dyadic pairings of providers and commanders that promoted such “anchored personalization” (DiBenigno, 2018), there was variation in the extent to which providers developed influential relationships with commanders and got them to regularly follow their recommendations. This is because although assigning providers to specific commanders provided the opportunity for a personalized relationship to form, it did not guarantee it. In this paper, I analyze variation between providers who were able to build influential relationships with commanders and those who were not despite having similar clinic-level opportunity structures for such a relationship to form.
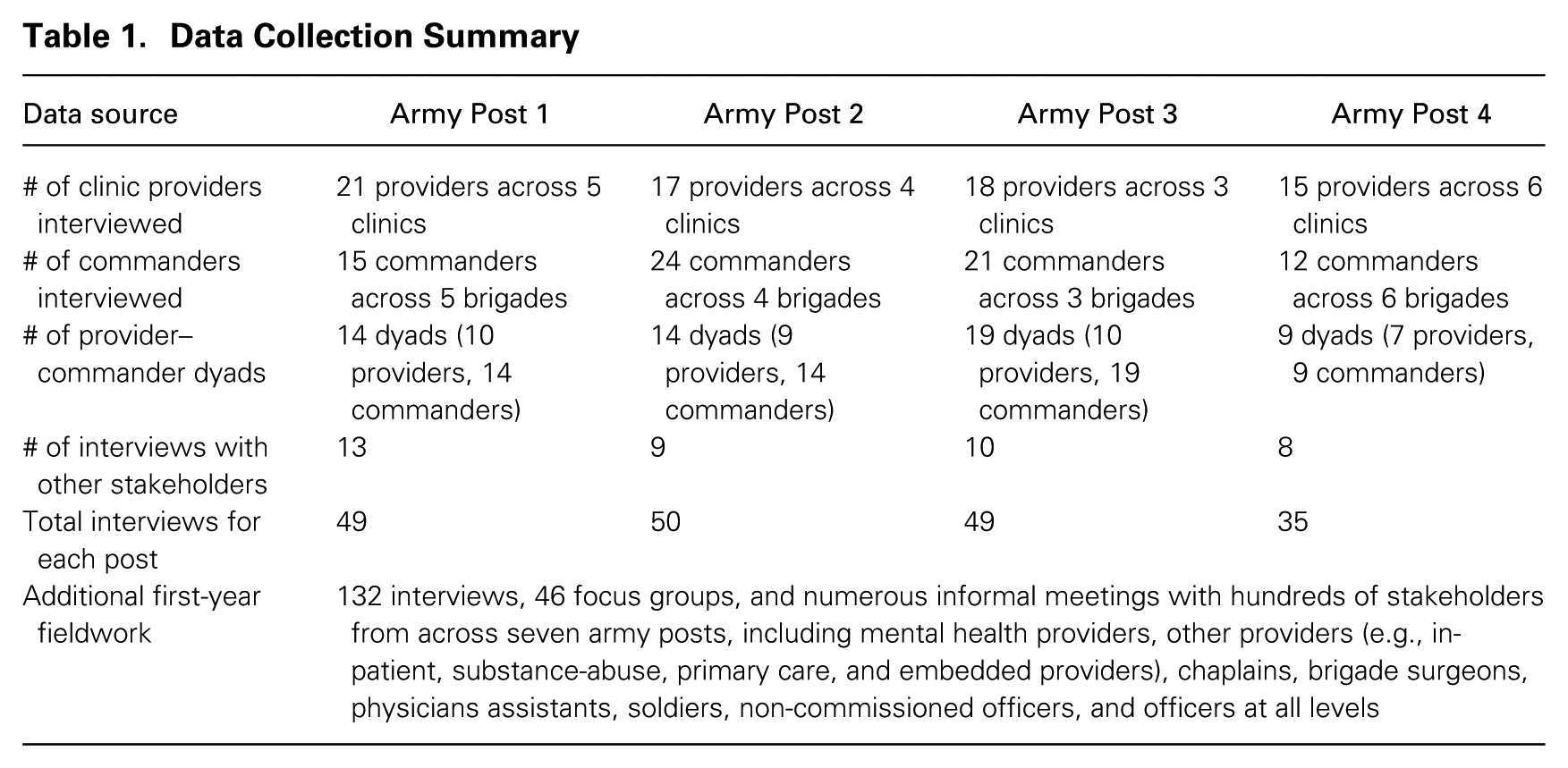
My sampling strategy involved interviewing mental health providers from a variety of backgrounds (Small, 2009) in all eight clinics―uniformed and civilian, psychologists and social workers, male and female, assigned to combat and to sustainment units, prior combat experience and no combat experience―as well as one to three commanders assigned to work with each of the providers in these clinics, so that I had data on pairs of providers and commanders. By interviewing both members of the dyad, I could then triangulate their accounts of the same situations and relational dynamics, as well as triangulate these accounts with those from other members of their clinic and brigade. In three cases, I did not interview both members of the dyad, but I was able to corroborate details of their relationship and whether the provider’s recommendations were followed or not by relying on another clinic team member or source. In total, I collected detailed data on 56 provider–commander dyads, as summarized in table 1. These semi-structured interviews spanned between one and three hours, with most lasting an hour. I recorded and transcribed all interviews when permission was granted; when it was not, I took extensive notes and typed them up within 24–48 hours. Interviews focused on four main areas: the interviewee’s background; the relational history of each provider–commander dyad; when conflict situations occurred and how they were addressed; and tactics and strategies providers used to build relationships with commanders and commanders’ reception of these tactics. I generally interviewed commanders first so that providers then focused their responses on their experiences with those specific commanders.
Data Collection Summary
Inductive Dyadic Data Analysis
I employed an inductive analysis approach (Glaser and Strauss, 1967), which consisted of reading and re-reading field and interview notes and writing analytical memos about relations between mental health providers and commanders. My analysis proceeded in three broad stages. In the first stage, I analyzed interview transcripts and field notes from my first 12 months of preliminary fieldwork. This analysis revealed the widespread theme of mental health providers facing challenges in eliciting cooperation―willingness to support and follow their treatment recommendations―from the commanders of the soldiers they were treating.
In the second stage, I focused on understanding how, despite these barriers, many providers developed highly influential relationships with commanders. I first coded provider and commander data separately and then coded them by provider–commander dyad for all dyads that had worked together for at least three months. I analyzed the relational history of the dyad from their first encounter through their most recent interactions, which included detailed accounts of conflicts and disagreements. Through this coding process, I identified numerous tactics providers used to try to build influential relationships with commanders. I noted a specific sequencing of these tactics: providers used some tactics immediately upon being assigned to a commander, some shortly afterward, and some during the remainder of the relationship. I also noted that some tactics seemed more effective than others. I coded each of the 56 dyads according to whether it was an example of a successful or failed influential relationship: a successful dyad was one in which both the provider and the commander reported that the commander regularly followed the provider’s recommendations. I noted a puzzling pattern: providers used many tactics in successful relationships that they also used in failed relationships.
In the third stage of analysis, I sought to understand why and paid special attention to the 63 percent of dyads for which I had data on the same provider working with multiple commanders. To do this, I mapped out the relational history of each of the 56 provider–commander dyads temporally to identify when providers used each tactic and whether the tactic was successful, according to both the provider and the commander, in building an influential relationship in which the commander regularly followed the provider’s recommendations. I found that there were three phases associated with a provider building an influential relationship: (1) gaining access to and knowledge of the commander, (2) gaining the commander’s trust, and (3) gaining and maintaining influence over the commander. I also noticed that particular tactics were useful in particular phases. Finally, by analyzing the relational history of the dyad, I noted that providers had short windows of opportunity in which to cultivate relationships with commanders. Early conflicts or the provider’s inability or unwillingness to use the phased tactics were associated with failure to build an influential relationship. I used these findings to create a process model of building influential relationships with line managers as a peripheral expert.
Findings
Peripheral Experts Lacked Formal Authority over Line Managers
Despite the army leadership’s support for and investment in mental health services, I observed that soldiers could not fully benefit from them when their direct commanders did not follow mental health providers’ treatment recommendations. As members of the medical support function, mental health providers lacked authority over the line commanders responsible for the soldiers they treated. This meant commanders could override their recommendations. Most providers quickly learned they were dependent on commanders for their soldier-care recommendations to be followed. One provider explained, “One of the things that I maybe didn’t realize until I got involved in doing this a little bit more is when I make a recommendation to the commander, that’s all that is, it’s a recommendation. The commander can choose whether or not they want to follow that recommendation.” Another provider noted the difficulty of getting in touch with commanders and getting them to follow his recommendations:
They’re hard to get ahold of, and when you get ahold of them, they either immediately agree to everything you say but then don’t follow through, or they tell you, “It’s not an issue. . . . The soldier’s lying to you. . . . He’s a stellar performer. . . . He’s the best we have. I don’t support the treatment. I don’t think he needs treatment.” So we have the overly agreeable who then don’t follow through and the ones that are just totally unsupportive.
Yet as all providers noted, commanders’ support for their recommendations was critical for soldiers’ recoveries. One provider explained, “I can say to the patient, ‘You need to get 8 hours of sleep’ and tell command that too. But if command puts you on a mission where you’re only getting 5 hours a night or are pulling 24-hour staff duty, there’s no way you’ll get the sleep you need to recover.”
Peripheral Experts’ Expertise Not Valued by Line Managers and Provoked Conflict
Providers’ mental health expertise and credentials were largely not valued by commanders, and their soldier-care recommendations regularly provoked conflict. With the exception of three commanders who were all receiving treatment for their own mental health problems, commanders started out with a negative view of the army’s mental health services. One provider explained, “Building credibility was absolutely the challenge, and we had none. In fact, we were in the negative. We were Mental Health. You are not to be trusted.” Providers were members of the lowest-status department in the medical organization as those who treated invisible rather than physical wounds. Providers were aware their expertise was not highly regarded. As one noted, “There’s also a negative perception of Mental Health. On the food chain of MEDCOM (the medical department), the lowest life form is Mental Health.”
Commanders generally viewed providers’ expertise and recommendations as interfering with their core line work of training mission-ready units and as threatening control over how they ran their units. One commander explained this frustration, turning red as he recalled a heated interaction with his assigned provider:
Do not try to threaten me by using big medical words. . . . The social worker told me how many days leave this guy needs! . . . I challenged it and said, “No,” and the social worker said he must have those days off or he will deteriorate. I’m like, “Let me do my job!” Granting leave is my decision.
The negative impression commanders had of providers and their recommendations was kept salient through an ongoing series of conflicts that regularly occurred between nearly all mental health providers and commanders. Given the nature of their work, providers regularly and inevitably made decisions and recommendations that commanders said inconvenienced or had a negative impact on their subunits. Providers primarily contacted commanders in four circumstances: (1) when a soldier’s mental health condition was serious enough to warrant a recommendation of a work modification or reduction, such as sitting out a stressful training exercise, deployment, or other duties; (2) when a soldier’s condition required the additional support and resources of the unit, such as escorts to appointments, restricted access to weapons, and additional supervision; (3) when requesting that a soldier not be punished for minor or major disciplinary infractions related to an underlying mental health condition; and (4) when a soldier’s mental health condition was serious enough to qualify them for a medical retirement or medical discharge from the army.
Commanders often resisted providers’ recommendations because they made it more difficult for them to meet their mission-readiness training targets when soldiers were taken “out of the fight” by missing work to attend appointments, sitting out trainings, or using resources from the unit that detracted from preparing for the mission. Commanders unable to meet their targets, which they were assessed on monthly, were relieved of command or not promoted. Providers were generally aware of the conflict and resistance their recommendations provoked. One provider shared, “They get upset. I think that sometimes that drives a wedge between command and the provider. Because command is looking at it as a mission thing. The provider is saying, ‘Hey, you have to do this, you have to do that.’ And they don’t like being told what to do.”
Peripheral Experts Seen as Outsiders Who Lacked Knowledge of Core Work
Providers were also disadvantaged by their peripheral position in the organization, far outside the social network of commanders in combat units. The mental health professionals―a mix of psychologists, licensed clinical social workers, and psychiatrists―were members of the support function of the army belonging to the Medical Department and reporting up to the army surgeon general. Their clinics were located close to the brigades they served, but given their high patient loads, providers had little time in their schedules to leave their clinics to see their soldiers or commanders in action at work. Given their peripherality, even providers with military backgrounds often lacked access that would help them understand the specific missions and daily work of the multiple commanders they worked with. Hence providers were often viewed as out-of-touch outsiders who did not understand the missions of their units or the army and thus were a threat to those missions. In part because of this lack of trust in providers’ understanding of military life, many commanders said they believed Mental Health was full of “shammers” and that the majority of soldiers seeking help were faking sick to get out of work or angling for an undeserved medical retirement and pension by duping what commanders considered naïve “Berkeley hippie” civilian providers. One noted:
Some guy got 80-percent benefits for lying his way through Mental Health, and it sickens me. It just sickens me. But what can you do? Can I hook them up to a polygraph? . . . If the guy comes in there and describes a made-up scene from a Hollywood movie to a civilian provider, the civilian provider is nodding her head saying, “I’m so sorry, honey.”
Peripheral Experts Shared Few Characteristics with Line Managers
Finally, mental health providers also faced barriers to eliciting cooperation from commanders because they had many characteristics that were devalued in this context and differed from those of most commanders, who were men under age 35. Online Appendix B provides a detailed demographic comparison. First, the majority of providers army-wide (~80 percent) were civilians rather than uniformed, active-duty providers (referred to as “green suiters”). In this context, civilians were considered untrustworthy outsiders. Even providers with prior military experience were not held in high regard if they had not deployed to a combat zone, which was the case for the majority of providers. One uniformed provider explained, “There is definitely a green suiter prejudice here. They talk about three levels of trust. You trust a green suiter with the patch [indicating they’ve deployed], then one without a patch, then a civilian.” Second, slightly over half of mental health providers were women in the male-dominated army in which femininity was demeaned as the polar opposite of the masculine warrior ideal. One commander explained the negative impression of his unit’s female uniformed provider who had not deployed: “You can read a uniform. She’s a green suiter, but she has not deployed, and she’s a female. She doesn’t have a lot going for her even though she wears the uniform. . . . And to make matters worse, when she started, she was pregnant.” While all providers were considered low status given their association with Mental Health, they varied on also being civilians and/or female. One female civilian provider noted, “I think you have a disadvantage when you’re a civilian and you’re a female and you’re Mental Health. Those are kind of three strikes against you. . . . I’m sort of so low on their totem pole it’s not even funny.”
Rapid Relationality Increased Peripheral Experts’ Influence over Line Managers
Nearly all providers started off “in the red” with their assigned commanders given the aforementioned barriers. With few exceptions, my interviews with provider–commander dyads corroborated that their relationships started off rocky given commanders’ initial low receptiveness to providers’ recommendations. Over time, however, most providers who had the opportunity to form relationships with their specific assigned commanders were able to achieve high levels of influence such that commanders regularly complied with their recommendations. Of the 56 provider–commander dyads analyzed, 64 percent of commanders regularly followed their assigned providers’ recommendations, as corroborated by both the commander and provider within the dyad. To understand this surprisingly high rate of success, I examined the tactics that led to success or failure across dyads in building these influential relationships, as well as their timing and sequencing. I call this process “rapid relationality.”
How peripheral experts use rapid relationality to develop a foundation for influence.
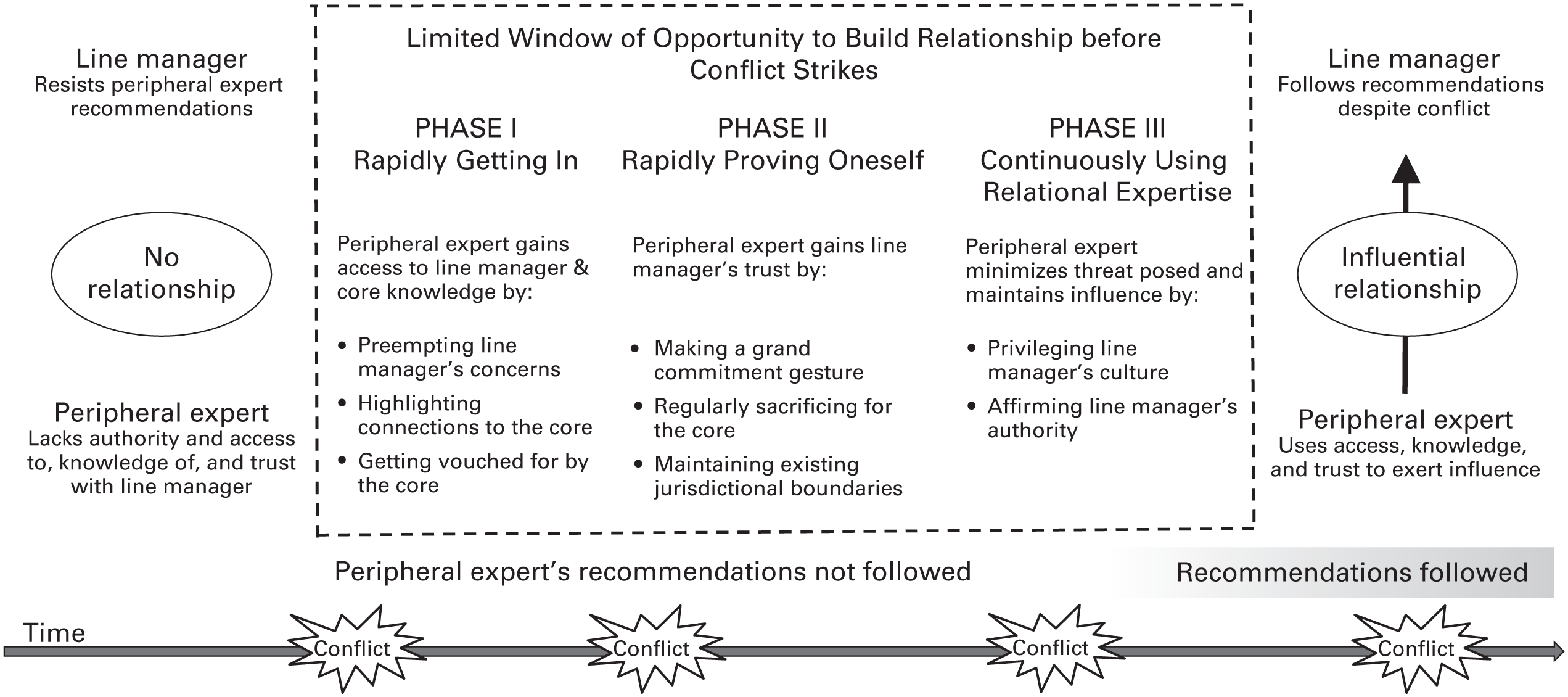
Through this rapid relationality process, a provider, despite lacking formal authority over the assigned commander, took advantage of a short initial window of opportunity to cultivate an influential relationship with the commander before conflict destroyed the chance for influence. As shown in figure 1, in the first phase, the provider used “rapidly getting in” tactics to gain access to and knowledge of the commander (or not). In the second phase, the provider used “rapidly proving oneself” tactics to gain the trust of the commander (or not). In the third phase, the provider continuously used “relational expertise” tactics to gain and maintain influence over the commander (or not) by minimizing the threat their recommendations posed. The first two phases occurred sequentially: a provider was unable to successfully use “rapidly proving oneself” tactics to gain the commander’s trust unless the provider had first used “rapidly getting in” tactics to gain access to and knowledge of the commander. In contrast, the third phase occurred continuously throughout the relationship. I have positioned it sequentially as the third phase because using “relational expertise” tactics in Phases I and II was insufficient for gaining access to, knowledge of, and trust with the commander, but not using these tactics after completing Phases I and II led to failure. The tactics listed in each phase in figure 1 are the most common ones providers successfully used to influence commanders, as corroborated by both providers and commanders and illustrated in table 2. Providers did not need to use all eight tactics across the three phases, but to be successful, they did need to use at least one tactic within each phase to achieve rapid relationality.
Rapid Relationality Tactics by Phase
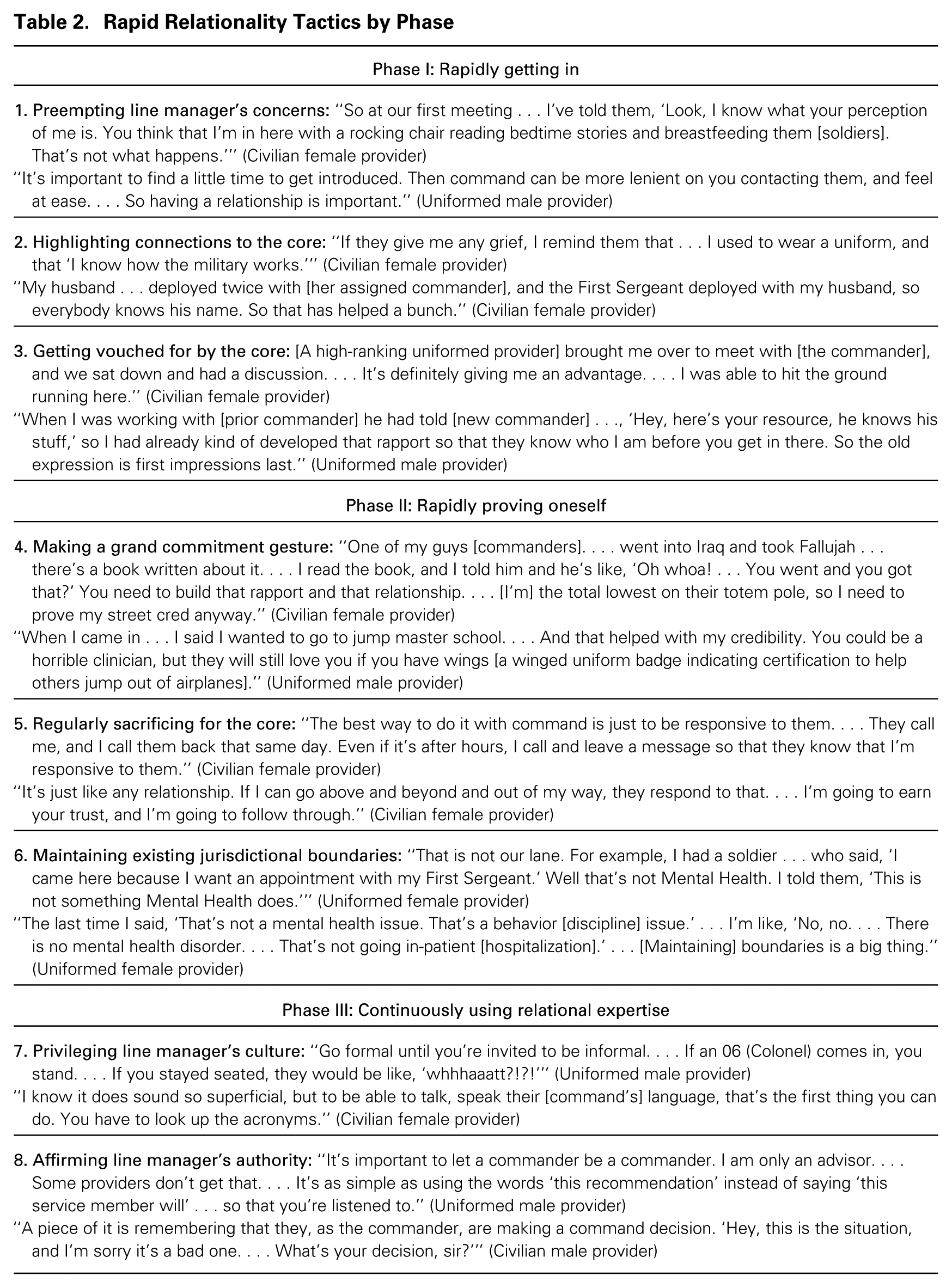
Phase I: Rapidly Getting In
Providers were generally conscious of their lack of power and peripherality relative to the commanders whose soldiers they treated. Thus providers often attempted to “get in” with their assigned commanders in hopes of gaining regular access to and relational knowledge about them to gain commanders’ compliance with their recommendations. As depicted in table 3, in Phase I, providers in 79 percent of the provider–commander dyads successfully gained access to and knowledge of commanders, while providers in 21 percent of the dyads failed to do so. The providers in the successful dyads used three main tactics in Phase I: preempting a line manager’s concerns, highlighting connections to the core, and getting vouched for by the core. Providers in the Phase I failed dyads either did not have time to use these tactics before the first major conflict hit, typically within the first few weeks of working with the commander (58 percent of the Phase I failed dyads), or they were unable or unwilling to use these “getting in” tactics at all (42 percent of the Phase I failed dyads).
Success and Failure of Rapid Relationality Tactic Usage by Provider Type*
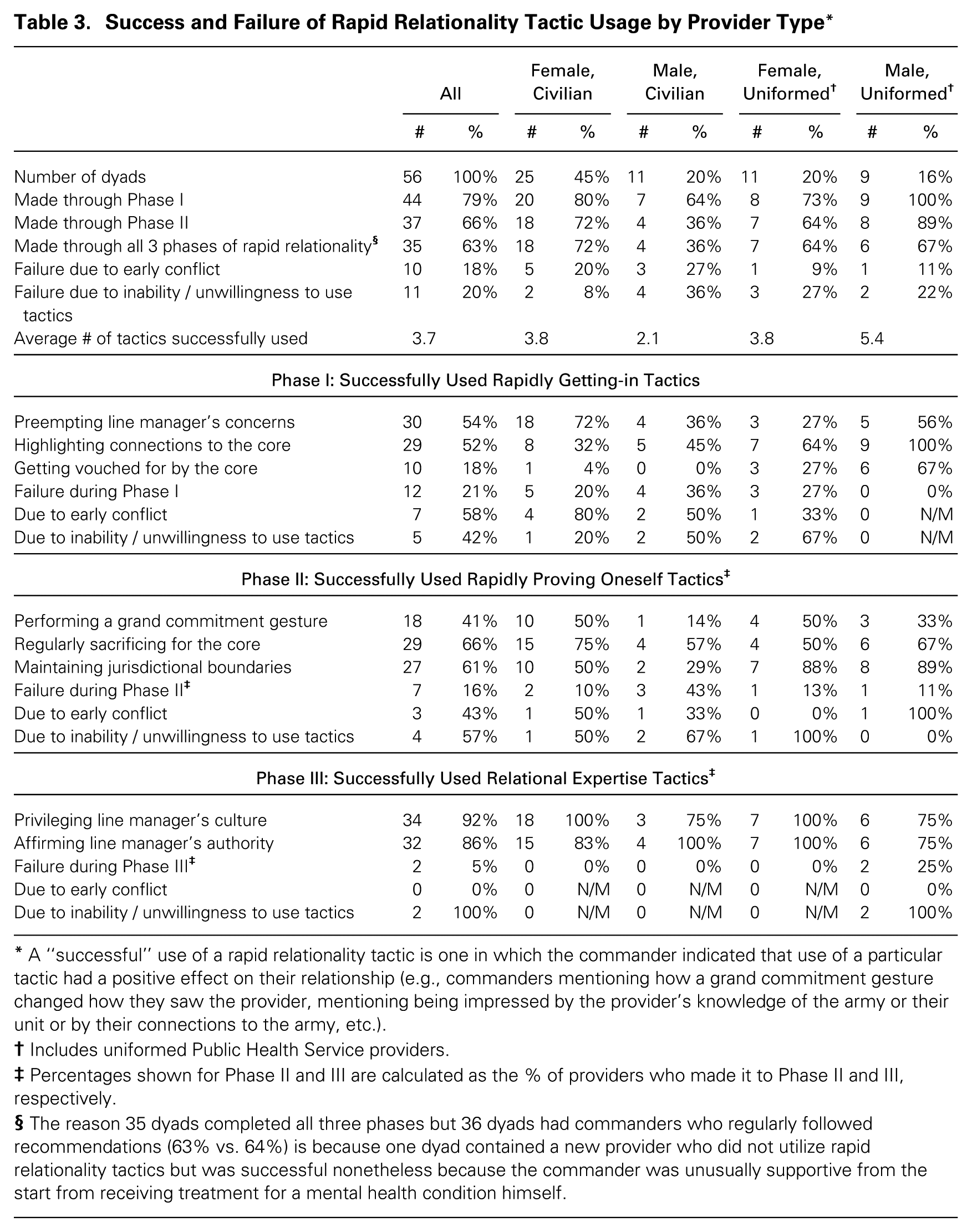
A “successful” use of a rapid relationality tactic is one in which the commander indicated that use of a particular tactic had a positive effect on their relationship (e.g., commanders mentioning how a grand commitment gesture changed how they saw the provider, mentioning being impressed by the provider’s knowledge of the army or their unit or by their connections to the army, etc.).
Includes uniformed Public Health Service providers.
Percentages shown for Phase II and III are calculated as the % of providers who made it to Phase II and III, respectively.
The reason 35 dyads completed all three phases but 36 dyads had commanders who regularly followed recommendations (63% vs. 64%) is because one dyad contained a new provider who did not utilize rapid relationality tactics but was successful nonetheless because the commander was unusually supportive from the start from receiving treatment for a mental health condition himself.
Preempting a line manager’s concerns
The first tactic encompassed providers’ efforts to proactively reveal and address commanders’ negative preconceptions about Mental Health and themselves as providers. It included ensuring that during their initial interaction, the provider asked little or nothing of the commander, focusing instead on what the provider could offer. One provider explained this tactic of preemptively addressing commanders’ concerns upfront:
I try to address it right away upfront by saying, “Hey! I’m [first name], and here’s what you’re probably thinking, that I’m a female civilian in medical command with no combat experience. ‘What the hell can you tell me?!’ Well, here’s what I can offer.” I tell them, “That’s what you were thinking,” and that seems to go over well.
Other providers described the importance of setting up one-on-one time with commanders to dispel concerns early on and attempt to overcome some of their disadvantaging characteristics. One provider explained how she regularly invited new commanders to her office at the clinic to do a “meet and greet,” in part so they could see her collection of military books to counteract the stereotype that she did not understand the army as a civilian woman:
In the beginning, I’d send out those messages to try to meet with them, to get that kind of individualized time with them. If they can come here to [the clinic], I think it helps because they see where their soldiers come . . . [and] they’ll see my books! . . . They’re seeing that I’m reading books on combat, on killing, and military psychology.
One challenge to preempting concerns was the difficulty of getting a meeting with a commander who did not return calls or e-mails. In these cases, some providers simply showed up unannounced at commanders’ offices to introduce themselves.
Highlighting connections to the core
The second tactic providers used to “get in” with commanders was calling out any possible personal connection they had to the core army war-fighting function. For civilian providers, this included bringing up whether a spouse or family member had served in the military. Providers who had prior military experience themselves would bring it up immediately, even if they had never deployed. One former active-duty uniformed army psychologist who was now a civilian provider explained:
I bring up that I was active duty right away. . . . I think this job would be so much harder if I hadn’t been in active duty. Whether this is fair or not, they may respect me on a little bit different level because they’re like, “Okay, she was one of us” even though I wasn’t really one of them, I wasn’t in combat arms. They oftentimes will say, “Well you get it, you were active duty” and I’m like, “Yeah.” Even if I don’t, I’ll say, “Yeah, I do get it.”
In one case, a civilian provider who had never served in the military prominently displayed photos in his office of himself with a two-star general who was his friend. In another case, a former active-duty civilian provider hung his old uniform on the inside of his office door to remind commanders and other visitors of his prior high rank and connection to the core.
Active-duty uniformed providers’ connection to the core was immediately visible, and they were largely considered insiders, especially if they had deployed and wore a combat patch. Nearly all commanders assigned to providers in uniform or who had prior military experience commented on this as a positive attribute. One commander recalled first meeting his assigned civilian provider who had prior military experience: “When we were first introduced, he said he was in the navy, so that told me he had military experience and could relate somewhat. . . . [Since] he’s a civilian. . . . I thought it was pretty cool.”
Getting vouched for by the core
Preempting concerns and highlighting connections to the core assumes that commanders made time to meet with providers or return their calls or e-mails. This did not always happen. Some providers employed an alternative route to getting in: getting vouched for by someone who was already “in” with a core member. In some instances, outgoing commanders vouched for their providers to the new commanders, such as by inviting the provider to the command staff transition meeting. A provider explained how much she perceived this personal vouching helped with getting in: “[The commander] came here and included us in [the transition staff meeting], where the outgoing and incoming [command] could meet, so they knew who we were, and they were like, ‘You need her. She’s your friend.’ That helped us get off on the right foot.” Another way of getting vouched for was being introduced by a uniformed provider who already had strong relationships with commanders, especially if they were high-ranking and had deployed.
Using at least one of the three tactics described above resulted in providers attaining the relational resources of access to and knowledge of the commander and their subunit. From the commander’s perspective, this meant that when their provider contacted them, they knew who the provider was and returned their calls or e-mails, and they felt their provider had enough knowledge about them to understand what they cared about most―their subunit’s specific mission. After one provider used the two tactics of highlighting connections to the core and preempting concerns, her commander noted that she “gets it. Her husband is in [name of another unit on post], so she knows about the military, more than you’d think. . . . I admit I was skeptical when she first showed up here [in his office]. She’s a wispy little thing—a light breeze could blow her over! [Laughs] . . . But that first meeting helped. I liked that she came over here and got to know more about what we do. . . . [Now] we are always going back and forth on e-mail or phone.”
Failure at getting in due to early conflict
While most providers were successful at deploying one or more of these getting-in tactics, some failed. Failure generally occurred when too many minor conflicts or a major conflict occurred before a provider had successfully gotten in, closing the provider’s window of opportunity to establish an influential relationship. This often happened when a dyad’s first encounter was in response to a conflict, as providers were expected to prioritize patient care, making it easy to delay meeting their assigned commanders. New providers were also more likely to fail if they had not yet learned the importance of quickly getting in with their commanders. One male uniformed provider explained how early conflict contributed to failed relationships: “I think what ends up happening oftentimes is that the first interactions that people have with the [commanders] are when there is a problem. . . . Or when I tell the soldier to do something and the command says no. That’s going to lead to conflict.” A female civilian provider noted how early conflict made it difficult to establish a cooperative working relationship when she had not gotten in quickly enough with a commander:
You might have a problem on day one, before you have that relationship. I have experienced that, and I think for me it’s almost like it puts a bad taste in my mouth, and for the commander, puts a bad taste in the commander’s mouth. So that working relationship is definitely strained moving forward from that point.
In these situations, providers often used less effective tactics of last resort that resulted in limited long-term cooperation, in hopes of waiting it out until they could start fresh with a replacement commander, since commanders rotated out or deployed about every one to two years. One provider explained how early conflict jeopardized her relationship with a commander:
I wrote a profile [a written work restriction recommendation] that he [a soldier] not go [to an important training] . . . so after that, command did not consult me as much. . . . . Or they may ignore you . . . or you can do everything you can, and command will still not work with you. So in those situations, you just wait it out and there will be a new command.
The most commonly used tactics of last resort included upward appeal (going to the commander’s boss), coalitions (using another messenger), appeals to one’s expertise, and assertiveness (ultimatums), which corresponded with tactics identified in the literature on upward influence as sometimes being effective in one-off influence attempts (e.g., Kipnis, Schmidt, and Wilkinson, 1980). Using these more assertive tactics often exacerbated relations and made future attempts to get in even more difficult, because they were perceived as inappropriate and they cemented commanders’ negative impression of Mental Health. Yet providers said they had little choice but to turn to harder tactics since it was nearly impossible to repair the relationship and use the softer tactics of rapid relationality after early conflict closed their window of opportunity to establish an influential relationship.
I observed failure to get in not only among new providers but also among well-seasoned providers who had highly influential relationships with their other assigned commanders. They failed to get in with these other commanders before conflict occurred and their window of opportunity closed. For example, Provider71 had a highly influential relationship with Commander72, who corroborated regularly following her recommendations, but failed to get in quickly enough with―and thus lacked influence over―Commander74. Provider71 took quick action to get in with most of her assigned commanders by inviting them to visit her in the clinic at an open house to dispel myths about what she did. Provider71 explained, “Commanders need to know your [assigned] provider . . . right away. . . . So I wrote an e-mail to them all to take a tour . . . so they could see that we’re not scary.” This tactic was effective at giving her greater access to Commander72 and greater knowledge of the best way to prove herself to him, as I describe in the next section.
Although Provider71’s efforts were generally effective, they did not always work if a major conflict occurred before she could get in. Commander74 was unable to attend her clinic open house, and soon after, their first encounter was over a major conflict. Provider71 made a recommendation with which he strongly disagreed: to medically retire a soldier who was caught doing drugs—an offense that typically results in a dishonorable discharge—because she believed the drug use was linked to the soldier’s underlying mental health problem related to his prior deployment. Commander74 challenged her recommendation and pursued what is known as a “dual track” chapter in which the disciplinary action was pursued in concert with the medical retirement. He believed the soldier was faking sick to avoid punishment. He told me, “Mental Health is not savvy to abuse. . . . We had a huge file of misconduct. . . . Some of it doesn’t make sense.” Provider71 noted that she had been unable to rebound and get in with this commander after this major conflict, so she had trouble getting him to respond to her e-mails and phone calls on other soldiers’ cases. This same dynamic played out in other dyads, summarized in table C1 in Online Appendix C, which maps the relational histories of all 56 provider–commander dyads I analyzed, and illustrated with an additional dyadic example in table C2. It should be noted that on two occasions later on in their relationship, Provider71 made similar recommendations to Commander72 about medically retiring soldiers who had committed misconduct. Her recommendations provoked conflict, but her influence endured because this occurred after she had already gone through all three phases of rapid relationality.
Phase II: Rapidly Proving Oneself
Once providers had gained regular access to and knowledge of their assigned commanders, they deployed “proving oneself” tactics to gain their commanders’ trust. Providers in 84 percent (37 of 44) of the dyads who successfully made it through the first phase of developing an influential relationship also made it through the second phase. Providers in these successful Phase II dyads used three main tactics to gain trust: making a grand commitment gesture, regularly sacrificing for the core, and maintaining existing jurisdictional boundaries. Providers in the Phase II failed dyads either did not have time to use these tactics before the first major conflict hit (43 percent of the Phase II failed dyads) or were unable or unwilling to use such tactics (57 percent of the Phase II failed dyads).
Making a grand commitment gesture
The first tactic included leveraging knowledge of what the commander valued to quickly prove oneself through engaging in a grand commitment gesture showing one’s allegiance to the unit. Typically these gestures had little to do with the provider’s professional expertise as a clinician and were received as an unexpected show of dedication to the commander and unit. For instance, a female civilian provider assigned to a cavalry unit used her access to and knowledge of her assigned commander to request joining and partially participating in their “spur ride”—in which soldiers endure challenging tests to earn their “spurs”—as a way to prove her commitment to the commander in a way that was meaningful to him:
One of the first things I asked [the commander] . . . was if I could participate in their spur ride. And so I was out in the field for 72 hours. And that gave me a whole lot more credibility. . . . I’m probably a little soft in the head, but having not served . . . it gave me a true credit with them. . . . so I definitely got this increased credibility.
A female civilian provider of a field artillery unit learned during her first getting-in meeting with the commander how much pride he and his soldiers took in the cannons his unit operated. She requested a demo at this first meeting, which the unit later enthusiastically put on for her.
In another case, a civilian female provider invited herself to an offsite field training and slept on the floor of a medical Humvee. The commander involved described this gesture as a turning point in their relationship, noting it “was an ‘ah-ha’ moment for me. Some soldiers are more open to it [Mental Health] than others, and it helps having them out there with us so they could see them and put a face to a name. And we could really develop that rapport.” Other providers showed up at their units’ morning physical training sessions and did pushups or ran with their units early in their time working together. One civilian female provider made a grand gesture by buying pizza for her unit and making it known she was paying out of pocket.
Regularly sacrificing for the core
The second common tactic providers used to rapidly prove themselves was to show how they were routinely sacrificing something for the commander’s unit. Sacrifices were generally of a smaller scale and performed more regularly than grand commitment gestures, which were typically one-off actions of special significance. Regular sacrifices included practices such as routinely giving up one’s lunch hour or staying late (unpaid) to see a patient a commander was worried about. Some providers sacrificed by sharing their personal cell phone numbers so commanders could regularly call them outside their official work day. Most also noted the importance of being extremely responsive early on to commanders’ calls and e-mails. One provider said, “What worked for me was going out of my way. So if they called . . . and said, ‘I have so and so,’ I will say, ‘Send them over at 12 and I will take no lunch to make sure I see them.’” A male uniformed provider explained a similar strategy of being hyper-responsive, noting, “You have to earn that credibility with command to prove yourself, and then they will call your name. . . . If they have a need, your response can’t be, ‘No, I am at lunch.’ You need to jump to it!”
Maintaining existing jurisdictional boundaries
The final tactic providers regularly used to quickly prove themselves involved not automatically assuming that all soldiers who came to them had issues that were the sole purview or jurisdiction of Mental Health right from the start of working together. By maintaining these boundaries, providers minimized commanders’ fears that they were enabling soldiers to fake sick to miss work (known as “skating” or “shamming”), which was a moral affront to most commanders. One provider explained the extra effort she made to assure the commander she was policing these boundaries to not be fooled by soldiers: 1
I have to go above and beyond to prove my abilities, to show that I’m not going to be snowed over by people who come in and want to . . . get out of going to PT [physical training] or want a med board [medical retirement]. . . . That’s one of the reasons too that I want to meet face-to-face with the commanders and say to them, “I’m going to be honest with you about your guys, and if there is someone that really needs something, I’m going to talk to you about it. But, on the other hand, if there is someone who is shamming, I’m going to be honest with you about that too.” I think they appreciate . . . knowing that we screen for that kind of stuff too.
This tactic was especially effective, as one commander noted when describing his assigned provider: “[Name of provider] is a straight shooter, and we’ve really developed mutual trust where he will not let soldiers skate.” A civilian provider likewise noted how he made sure not to overstep commanders’ jurisdiction by “sending back” soldiers with non-clinical issues to commanders for support. He explained a case in which a soldier’s insomnia and anxiety were rooted in financial problems that he believed his commander could better address by providing a loan through an army program:
[S]ometimes when you bring in command, they can also help solve the soldier’s [non-clinical] problem—that’s their job. . . . Once they realize they [soldiers] don’t have to hide it and it won’t be punitive, patients will open up more to their leadership. That’s the number one way I like to lose my patients.
Providers were considered successful at proving themselves when they used at least one Phase II tactic such that they gained the relational resource of trust from their assigned commanders. Providers often described how gaining this trust created a critical turning point in their relationship after which commanders tended to be on board with their recommendations and followed them even when disagreeing with or feeling inconvenienced by them. One provider described such a change after she performed a grand commitment gesture, noting that “since then, they [the commander] haven’t questioned me ever.” Her assigned commander corroborated this account: “If [name of provider] says we shouldn’t take him or [the soldier’s] not clear [to deploy or attend a training exercise], I trust her. I don’t push back. . . . If she goes to bat for you, it, it means you have a legitimate problem in my book.” 2 Another commander shared the trust he had in his assigned provider even when he disagreed with him, because the provider had proven himself in numerous ways by using the tactics of maintaining existing jurisdictional boundaries and regularly sacrificing for the core, such as by being willing to talk to the commander after normal work hours. The commander said about his provider:
So that’s the guy I trust. . . . That relationship is critical. You know, [name of provider] and I will talk at all times of the day . . . and I think [that] really demonstrates what a great partnership we have. . . . [W]e developed a very frank relationship. . . . So, it’s been a very positive relationship. I won’t pretend like there aren’t times where I disagree with the assessment of how a soldier had screwed up, should be punished or not punished, but we developed enough of an understanding of each other and where we’re coming from. We respect each other and so it’s never an adversarial conversation.
Failure to prove oneself before conflict occurs
While most providers quickly proved themselves after getting in, some providers failed when major conflicts occurred before they had a chance to prove themselves and their window of opportunity to establish an influential relationship abruptly closed. For example, Provider80 was a newly trained uniformed male psychologist who had not yet deployed, and he had built many influential relationships with his assigned commanders. As a male in uniform of a similar age as his commanders, Provider80 had an easier time getting in with them than some other providers did: “With the commanders, it wasn’t too bad. . . . most of them are about the same age as me, and we end up having a lot of things in common. I was able to pretty easily build good relationships with most of them.” Provider80 quickly used Phase I tactics to preempt concerns by setting up meetings with his assigned commanders and highlighting connections to the core during his first week to establish common ground before conflicts occurred:
My first interactions with them, with my commanders, it was walking over to their office, knocking on their door, sitting down with them for a half hour saying, “Here is a little bit about me. Tell me about your family,” and just kind of opening up in that way to set some groundwork so that you have some common ground to stand on when conflict does arrive.
Provider80 also described the many things he did to prove himself to these commanders, which included getting out of the clinic and going out to the field and firing range to observe their subunits in action and occasionally showing up at morning physical training (PT) to work out with them. He felt these tactics made a big difference:
I went to the field. I went to the range. I did some of that real army stuff that I don’t know if civilians [providers] either get the opportunity or feel comfortable kind of stepping out of the comforts of the clinic. . . . But there is a lot to benefit from that. You get a lot more buy-in . . . if they see you as being more than just somebody who sits in an office.
Conflicts that came up were resolved such that his recommendations were followed and the relationships endured, even if commanders were not always happy. For example, Commander93 was not happy about a recommendation that pulled one of his top-performing soldiers out of an important training deployment, but the provider’s relationship and influence with Commander93 survived. Provider80 shared, “Usually we address it and work through it and the relationships are good enough to survive it. They may say, ‘I didn’t like what you did’ and then we can move on.” Most of the commanders with whom Provider80 had rapidly built influential relationships followed his recommendations.
The exception was Commander77, with whom a major conflict over a soldier suicide occurred early on, before Provider80 had a chance to prove himself. This commander said about Provider80, “He has no context and doesn’t come here.” Commander77 blamed Provider80 for not alerting him to this soldier’s mental health issue, even though at the time of the suicide, the soldier was not considered a harm to himself, so Provider80 was not obligated to inform his commander. Commander77 put pressure on Provider80 to share information about other soldiers seeking care and, when Provider80 balked, became “furious.” Commander77 explained, “If something is serious, you need to share it, not after it happens. This is why officers get paid, to take these risks. We need the information!” After this major conflict, relations between Provider80 and Commander77 were adversarial. Commander77 refused to follow other recommendations from Provider80, in whom he said he had lost all faith. Provider80 then resorted to more assertive tactics of last resort by directly challenging Commander77. He noted the commander now fought him on everything: “I would recommend a course of action, and he would tell me why I was wrong.”
Other providers who failed to prove themselves were those―often new providers―who felt their clinical expertise as mental health experts should be sufficient for commanders to listen to them. One new civilian provider explained, “I have the subject matter expertise—you can take it or leave it.” This was also the case for a formerly high-ranking retired uniformed provider who was now a civilian provider. Although he quickly got in by sharing his prior military experience, he struggled to prove himself and was frustrated by being unable to simply give orders and have them obeyed as he did before. He explained, “I’m a [former colonel], I’m used to being in charge, and if I say it, that’s how it should be. . . . I don’t know how much longer I can do this for.” His assigned commanders wrote him off and ignored his recommendations, as conflicts arose around his orders and ultimatums without any semblance of a relationship built first.
Phase III: Continuously Utilizing Relational Expertise
Once providers had successfully proven themselves to their assigned commanders, they had key relational resources they could draw on as sources of power and influence: access to their commanders, knowledge of what their commanders valued, and trust. Nearly all commanders assigned to providers who had proven themselves regularly followed their providers’ recommendations. Yet these relationships remained asymmetrical, as providers had to do ongoing relational work to minimize the threat their recommendations posed and maintain their influence. Many providers employed tactics that emphasized their relational expertise, rather than clinical expertise, to address this challenge. Providers in 95 percent of dyads who successfully made it through the first two phases of developing an influential relationship also made it through the third phase. The successful providers used two primary tactics to maintain influence over commanders: privileging line managers’ culture and affirming line managers’ authority. Providers in the Phase III failed dyads did not use these relational-expertise tactics at all.
Privileging a line manager’s culture
The first tactic involved the provider privileging each commander’s cultural meaning system over their own. For example, many providers made an effort to learn and use army terminology, jargon, and preferred speech styles when interacting with commanders. A civilian male provider noted that he minimized use of clinical terminology in this setting: “Psycho babble doesn’t go over well at all ‘cause you lose ‘em. Absolutely lose ‘em. These guys’ jobs are . . . not to know, you know, psychodynamic theory. . . . Docs that try it that way don’t get along with the commanders very well. They come across as pompous.” Providers also demonstrated relational expertise by learning the rank structure of the army, proper terminology for their specific units, and ways to demonstrate respect, such as referring to officers as “Sir” or “Ma’am.” A civilian female provider explained:
I always call them “Sir” and they’re like, “Why are you calling me ‘Sir’? You’re a doctor.” And I said, “Because you’re the [type of unit] commander.” I just feel like that’s important to render them that respect. . . . And the Sergeant Major, knowing not to call the Sergeant Major “Sir” but calling him “Sergeant Major.”
Other providers said they demonstrated deference to the commanders’ culture by knocking before entering commanders’ offices; using formal greetings like handshakes rather than informal hugs; setting meetings at times that worked best with the commander’s schedule; and stocking one’s office with protein bars, rather than with candy, to offer to hungry yet health-conscious commanders.
Affirming a line manager’s authority
Another widely used tactic to demonstrate relational expertise that helped downplay the threat providers’ recommendations posed involved providers acknowledging their lower power relative to commanders. Providers were careful not to overstep their bounds, positioning themselves as advisors or consultants to commanders making recommendations rather than issuing orders. One male civilian provider explained:
I have conflicts with command many times, and I always say, “It’s your call, it’s your decision. I am hired to be your consultant, but I am merely your advisor, and I am advising you this way.” . . . By positioning it this way, I am affirming their positional authority, and I see that as essential because they are the leader, and then they recognize that I know they have responsibility for the decision.
Providers noted the importance of communicating in a way that gave commanders greater choice and control, treating them as the deciders, a role they were accustomed to playing. They often used disclaimers when making recommendations to command by saying things like “it’s obviously up to you” or “this is just a recommendation.” One male uniformed provider explained how he used this tactic: “You have to present things to them like it’s a choice, because it is ultimately their call versus ‘I’m the doc.’ All we make are recommendations. ‘If you do this, this is likely going to happen. I have 20 years of experience, but the choice is up to you.’” Providers used these tactics to downplay the threat their recommendations posed and maintain their influence. For example, after Provider71 got in by inviting Commander72 to an open house at her office to preempt concerns and after proving herself by performing a grand commitment gesture by spending the weekend at an offsite field training, Provider71 regularly utilized relational expertise to maintain her influence: she learned proper army terminology, stocked her office with protein bars to offer to commanders, and took care not to present herself as above commanders:
You don’t act . . . like you are above them. I didn’t grow up in the military, so I have to ask and be respectful. . . . I’m [her first name] in here, I’m here to help rather than, “I’m a licensed clinical social worker who went to [elite university].” [Instead] I say, “Call me [her first name]. Here’s my cell number.”
When major conflicts came up, such as when Provider71 thought a soldier in a vital role was not well enough to attend an important training, Commander72 was receptive to her request. Another conflict involved a soldier who was suicidal in his unit and “very impulsive”; Provider71 believed he should not be around weapons, but Commander72 did not initially believe he had a problem because he was a high performer who was hiding his issues at work. She noted:
They all loved this soldier. So they didn’t want to listen to me that something was wrong. (How did you handle that?) I didn’t get offended. I had [Commander72] come in and said, “Do you want a protein bar?” I got through to them. But I’m not getting in a power struggle. And they have to know I will do anything for them.
As additional conflicts arose, Commander72 explained how their relationship endured: “When something goes wrong, I generally call [Provider71], and we can talk it out and she finds a solution. And I’m angry, I’ll be cursing and yelling . . . and she’ll say in this calm and therapeutic voice, ‘What’s going on, [Commander72]?’ . . . She’s a great American.”
Failure at continuously utilizing relational expertise
The few providers who failed in Phase III got “too comfortable” and felt they could “let their guard down” and “speak freely”; they failed to maintain their influence by not minimizing the threat they posed through employing relational expertise. Instead of giving recommendations, one uniformed Public Health Service provider began to give direct orders. This change occurred after he received a promotion, as he assumed his new rank should result in greater deference from commanders; yet some commanders did not consider the Public Health Service, a special corps that supports public health and disease prevention, to have ranks equivalent to their own. The commander involved noted, “[He] pissed me off. . . . He’s in, what’s it called? Public Health or something? . . . I don’t even know what their ranks mean.”
In other cases, providers were unwilling to defer to the commander’s culture from the start. A clinic team lead who oversaw staffing and clinic operations explained how a provider had to be reassigned to another role because she refused to privilege the commander’s culture, such as by refusing to curse and acting offended by commanders who did curse, even though cursing was a central part of the infantry commanders’ culture: “[T]his one provider . . . did not work well with infantry because she would not say ‘fuck’ or ‘shit,’ and infantry soldiers get offended by that!” Another provider commented on how a new female uniformed provider struggled because she failed to privilege the commander’s culture by not adjusting her demeanor during command interactions: “She had no military bearing or background and would try to hug commanders or not knock before entering command’s office! (He looks mortified by this breach of decorum.) No military bearing at all . . . so it was hard for her.”
The Influence of Providers’ Characteristics on Achieving Rapid Relationality
While all providers faced barriers to developing influential relationships with commanders given their peripherality and lack of authority, providers varied in the baseline level of relational resources they had available to draw on based on their gender and status as uniformed versus civilian providers. These differences affected how long it took providers to go through all phases of rapid relationality before the window of opportunity closed for developing influence with commanders. While all successful providers went through all three phases of rapid relationality, providers with less valued characteristics in this context often faced greater barriers to getting in, proving themselves, and utilizing relational expertise―they had fewer tactics available to them or needed to use more extreme tactics to achieve the same level of influence as others.
Uniformed providers used more getting-in tactics than civilian providers, on average. This may be because civilian providers had fewer of these tactics available to them: many civilian providers had no one to vouch for them or had no connections to the core. Of dyads with female civilian providers, 72 percent successfully used preempting concerns as a tactic for getting in, 32 percent used highlighting connections to the core, and only 4 percent used getting vouched for. In contrast, in dyads with uniformed male providers, 56 percent used preempting concerns, 100 percent used highlighting connections to the core, and 67 percent used getting vouched for as tactics to get in with their assigned commanders. Table 3 summarizes the rapid relationality tactics successfully used by different types of providers.
Many uniformed providers, especially uniformed male providers, breezed through Phase I. As one male uniformed provider with a combat patch said, “As a uniformed provider, I have what we call ascribed credibility. . . . it’s the credibility people give you because you look like them. . . .” Civilian providers often took longer and hence were more often thwarted by conflict occurring before they had established a relationship, since commanders were more likely to ignore their requests for initial meetings given their reluctance to meet with or listen to a civilian. Providers with less valued characteristics exerted greater effort to prove themselves toward building an influential relationship, such as by employing more extreme and time-consuming tactics. Of all the “grand commitment gestures” successfully performed to prove oneself, 78 percent were performed by female providers―with 55 percent by civilian female providers. These gestures were often energy-intensive, required time away from home, or involved physical or mental suffering―for example, doing early morning exercises and pushups with the unit or spending the weekend at a training exercise sleeping on the floor. Fewer uniformed male providers, who had more valued characteristics in this context, employed such extreme gestures to prove themselves.
Different combinations of characteristics intersected to create varying levels of advantage or disadvantage for developing an influential relationship. Although masculinity was more valued in this context, many male civilian providers also faced barriers on account of their gender throughout all phases. Some civilian male providers perceived they were “held to a higher bar” than female civilian providers since they were expected to have mastery over the male-dominated army sphere. Some felt that female civilian providers received more leniency or a “pass” if they initially did not know proper army terminology, while civilian male providers felt penalized more for making the same mistakes. For example, one commander commented on how pleasantly surprised he was when his female civilian provider made an attempt to learn the proper ranks by hanging rank charts on her office wall: “I know she’s trying. I even saw a little printout she had up on her desk. She’s making an effort and it shows.” When civilian male and female providers performed similar grand gestures to prove themselves, those performed by civilian male providers often did not help them prove themselves with their assigned commanders. One commander gushed about how impressed he was by the commitment displayed by his female civilian provider after she showed up and attempted to do a few pushups at his unit’s early morning physical training (PT), noting, “[She] was doing PT with us and that really helps. Pushups and everything! Well, a few anyway! (Laughs) . . . It builds trust and in many ways, it broke down walls. . . . I have her on speed dial.” Few commanders commented on being impressed by their civilian male providers doing the same thing. One commander even commented that it was embarrassing that his male provider was so out of shape. This may help account for why 18 of the 25 dyads (72 percent) with female civilian providers made it through all three phases of rapid relationality but only 4 of the 11 (36 percent) dyads with male civilian providers were similarly successful.
Discussion
Contributions to Our Understanding of Peripheral Experts’ Influence over Line Managers
This paper makes a number of contributions to our understanding of how experts in peripheral roles in organizations can influence line managers to support their work and comply with their recommendations. First, existing research on peripheral experts has primarily focused on documenting the numerous challenges they face (e.g., Dalton, 1950; Allen, 1955; Edelman et al., 1991), not how peripheral experts can successfully influence line managers―a striking gap given the prevalence of professionals working in organizations in this “age of experts” (Barley and Tolbert, 1991; Kellogg, 2014; Lifshitz-Assaf, 2018). The three-phase process model of rapid relationality helps to explain how and when peripheral experts can accomplish this difficult feat, suggesting they may need to cultivate alternative, relational sources of power by using tactics to quickly capitalize on critical windows of opportunity early in interactions with line managers to develop influential relationships with them before conflict strikes. This study also highlights the importance of temporality for cultivating influence, suggesting it is not only what experts do to exert influence over line managers, but also when and how quickly they do it, that matters. Windows of opportunity for building an influential relationship can be unpredictably short.
Second, the existing literature on peripheral experts’ influence has primarily conceptualized the main barriers to influence as rooted in both their lack of formal authority over line managers and the conflict and resistance provoked by their recommendations (e.g., Dalton, 1950; Meyer, 1968). This study suggests another important barrier—the lack of a basic relational foundation for influence between peripheral experts and line managers. Because they are not part of the core organization, peripheral experts do not always have easy access to line managers, accurate knowledge of core line managers’ work, or ways to easily establish trust with them. This lack of a relational foundation is due to peripheral experts’ positions of disadvantage in their organizations as untrusted outsiders with nonvalued expertise who share neither the line managers’ social networks at work nor their organizational culture. Yet relational forms of power may be especially important for peripheral experts to cultivate since other avenues of attaining power and influence are structurally closed off to them. In situations like these, rapid relationality may provide a means for peripheral experts to gain relational resources they can use to influence line managers.
Finally, while scholarship on peripheral experts has noted how a lack of shared characteristics can exacerbate already negative relations with line managers (e.g., Dalton, 1950), no one to my knowledge outside of small-group laboratory studies (e.g., Thomas-Hunt and Phillips, 2004) has examined how variation in individual experts’ characteristics may affect their influence over line managers. By leveraging a unique dataset with dyadic pairings of peripheral experts and line managers, I could discern differences introduced as a result of providers’ varying background characteristics. I found that peripheral experts with characteristics most valued by line managers generally had a greater number of influence tactics available to them and used less time- and energy-intensive tactics than experts without these characteristics. Prior research has examined peripheral experts and line managers as groups rather than in dyadic pairings and hence could not assess how variation in individual relational resources can affect influence. The rapid use of relational tactics may be especially important for experts with disadvantaging characteristics, who need to exert more effort and take faster action than others, since it may take them longer to cultivate relationality.
Contributions to Our Understanding of Influence by Low-power Groups in Organizations
This study also makes a number of contributions to scholarship on influence among low-power groups in organizations. While prior research on issue selling, low-power occupations, and upward influence has detailed a host of tactics and processes for attaining influence in organizations (e.g., Mechanic, 1962; Schilit and Locke, 1982; Ashford et al., 1998; Dutton et al., 2001; Kellogg, 2018), the peripheral experts studied here did not have basic access to, knowledge of, or a means by which to establish trust with line managers in daily work and thus had to employ different tactics focused on achieving these basic relational resources. Prior research has been conducted on influencers and targets who likely already have existing relationships or fairly easy ways to develop them. Middle-manager issue sellers, low-power core occupation members, and subordinates or peers in the same department as their influence targets generally have access to their targets because the influencers are typically already organizational insiders with social network connections to their targets. These influencers also generally already have nuanced knowledge of their targets because of their daily interactions engaging in core work with them. And these influencers often have the means by which to easily establish trust because they can prove their worth to their targets through the superior execution of core work. In addition, if influencers and targets are in the same occupation, they are likely to share similar demographic backgrounds, which can facilitate liking and trust (e.g., DiBenigno and Kellogg, 2014). Although a few studies on issue selling have examined what would qualify as peripheral experts (e.g., Howard-Grenville, 2007), a close read of these studies finds that influence occurred only after a relational foundation had been established, such as when former core members joined the peripheral expert group and leveraged prior relationships to exert influence. Peripheral experts, such as a new safety officer or sustainability specialist who has never worked in the industry, may require rapid relationality tactics to first build a relational foundation with line managers before they can exert influence. Prior scholarship on low-power influence has also not examined this earlier period of relationship formation, suggesting that it is an open empirical question whether any low-power influencer, not just those in peripheral expert roles, might also benefit from using rapid relationality tactics.
Next, prior scholarship on influence by low-power groups has largely portrayed influence tactics as universal, such that they can be utilized by nearly anyone (e.g., Dutton et al., 2001). This study suggests there may be limitations to this one-size-fits-all approach, as individuals may vary in the speed at which they can establish an influential relationship. Influencers with characteristics valued by their influence targets may have a greater initial level of relational resources they can use to more quickly build a relational foundation for influence. Unlike prior work, this study examines how the unique attributes of each peripheral expert affect which tactics are available to them and the level of effort required to build an influential relationship.
Consistent with scholarship that has found gender (dis)advantage to be context-specific (e.g., Turco, 2010; Ridgeway, 2011), I found that civilian female providers were generally more successful than male civilian providers, even though masculinity was more highly valued in this male-dominated context. There may be two reasons for this. First, commanders may have evaluated male providers using a higher bar, as many commanders viewed knowledge of the army as something any “real man” should possess. Second, male providers may have been less willing and able than female providers to deploy some of the rapid relationality tactics. Since women often operate from lower-power and lower-status positions in society (e.g., Ridgeway and Smith-Lovin, 1999; Doering and Thébaud, 2017), they may be more accustomed to, and possibly more skilled at, utilizing relational forms of power to strategically achieve influence over higher-power others (e.g., Williams and Dempsey, 2014).
This study also extends our understanding of issue-selling processes in organizations. The greatest overlap between issue-selling moves and the tactics described here is in the third phase of rapid relationality, in which providers used relational expertise to maintain their influence and minimize the threat they posed by deferring to and affirming the culture and authority of the dominant commander group. In this third phase, the providers used issue-selling packaging moves such as strategic framing and tapping into the cultural values and schemas most cherished by the dominant group (Dutton et al., 2001; Howard-Grenville, 2007). The tactics elaborated in this paper in the other two phases of rapid relationality do not overlap with those detailed in the issue-selling literature. This difference is likely because scholars have not examined this early period in which peripheral experts first need to establish a relational foundation for influence (going through the getting-in and proving-oneself phases) before they can effectively use the kinds of tactics described in the issue-selling literature. My findings contribute to our understanding of issue selling by elaborating an additional set of tactics that may be necessary for issue sellers who are in peripheral positions in their organizations without alternative ways of acquiring relational assets (e.g., Howard-Grenville, 2007), a situation that is becoming more common as the use of experts in organizations continues to grow (e.g., Anteby, Chan, and DiBenigno, 2016).
This study also advances our understanding of scholarship on upward influence tactics, which has focused nearly exclusively on what people do (e.g., Kipnis, Schmidt, and Wilkinson, 1980; Falbe and Yukl, 1992; Farmer et al., 1997; Bruins, 1999) and the factors affecting whether an influence attempt succeeds, such as the organizational context, skill of the influencer, and characteristics/receptiveness of the target (e.g., Schilit and Locke, 1982), rather than on when they do it. These factors were largely held constant, however (e.g., same context, providers all skilled as clinicians at influencing behavior, nearly all targets initially resistant), and I observed variation in influence effectiveness. This may be because existing scholarship has not focused on the speed or temporal sequencing of deploying influence tactics. Applying a temporal lens to influence may help explain the mixed findings on the efficacy of various influence tactics in prior studies (e.g., Higgins, Judge, and Ferris, 2003). Whether certain influence tactics are effective may depend on whether one has first gotten in and proven oneself in their relationship with their specific influence target. Since most studies of influence tactics are survey-based and cross-sectional, few have data on the relationship history between the influencer and target over time, and they do not attend to temporal sequencing.
Contributions to Our Understanding of Relationality in Organizations
The relational turn in the social sciences has yielded a substantial body of scholarship on the value and importance of relationships, relationality, and social capital (e.g., Granovetter, 1973; Coleman, 1988; Emirbayer, 1997; Gittell, 2001, 2006; Dutton and Heaphy, 2003; Heaphy et al., 2018). Yet surprisingly little work has examined how work relationships are actually formed, particularly when asymmetrical power relations exist between ties. Scholars of social networks have found that attributes such as proximity, homophily, and likeability predict the likelihood of a relationship forming (e.g., for a review, see Rivera, Soderstrom, and Uzzi, 2010) but have not told us how these relationships develop and get off the ground. Work on relational coordination has highlighted how critical relationships characterized by frequent communication, mutual respect, and shared knowledge and goals are for achieving valued organizational outcomes (e.g., Gittell, 2001, 2006) but has not yet identified the micro-processes underlying how these relationships are built. And while positive organizational scholars have proposed practices and processes for building high-quality connections at work, the processes identified, such as respectfully engaging by being present and genuine, apply to existing relationships with a foundation that peripheral experts lack (e.g., between managers and their subordinates in the same department, administrative assistants and their assigned faculty members, etc.) (Dutton and Heaphy, 2003; Dutton and Ragins, 2017). Finally, recent studies of professionals working inside organizations suggest they may need to deploy “relational authority” and “relational expertise” (Huising and Silbey, 2011; Huising, 2015; Sandefur, 2015) to get their work done, rather than rely solely on their professional expertise, yet do not specify the process through which the relationships underlying these forms of authority are built. This study begins to fill this important gap by identifying the three-stage process of rapid relationality through which one important type of organizational relationship can be cultivated: between peripheral experts and core line managers.
Limitations and Opportunities for Future Research
The theory developed here should be considered in light of the following boundary conditions and limitations. First, one unique feature of the organizational context I studied is that the peripheral expert providers were explicitly assigned to work in dyads with line manager commanders, such that the opportunity for forming a relationship existed in a way that it may not for other peripheral experts. A dyadic pairing may be an important enabling condition for rapid relationality that helps explain why prior scholars of peripheral expert influence have not observed much successful influence. Creating such dyadic pairings is something many organizations could plausibly replicate to enable the opportunity for relationships to develop between line managers and peripheral experts (DiBenigno, 2018). Yet creating dyadic pairings was not sufficient for an influential relationship to develop—utilizing rapid relationality tactics to quickly build a relationship before conflict occurred was also necessary. Future research should examine other ways that a relational foundation for influence may be achieved and enabled.
Second, future research is needed to examine the extent to which rapid relationality occurs in other contexts with other groups. I would expect this process to be most relevant to other situations in which an occupational group lacks not only formal authority but also a relational foundation of access to, knowledge of, and trust from their influence targets. This likely encompasses those in roles considered peripheral to the core mission of the organization such that their expertise is not valued or is considered threatening, who are removed from the daily work and social networks of core line managers, and who have low status relative to line managers. For example, sustainability and diversity officers might benefit from using rapid relationality tactics to develop influential relationships with line managers, especially when first joining an organization. I would also expect the extent to which one’s individual characteristics are valued by line managers to affect how difficult building rapid relationality will be. While gender and military status were important characteristics that affected how easily the mental health experts in this study built influential relationships with line manager commanders, in other settings, different characteristics that are valued by or similar to one’s influence targets may matter most (e.g., youth in the start-up world). Other peripheral groups—be they safety managers, internal consultants, or cybersecurity experts—may find it beneficial to use rapid relationality to build influential relationships, though future research is needed to test this theory in other domains.
Finally, future research is needed to examine rapid relationality under other conditions. The length of the window of opportunity for establishing a relationship in other settings may vary, especially if peripheral experts have greater control over when conflicts arise or more opportunities for failure and second chances. Other peripheral experts may face similar unpredictable conflict timelines. For instance, cybersecurity professionals typically have no control over when hacks occur, potentially creating conflict with organization members by disrupting their work with computer updates and patches.
Implications: The Dark Side of Rapid Relationality
My elaboration of the micro-process of rapid relationality helps build theory on how and when low-power peripheral experts can influence line managers in core functions. But there are a number of macro, system-level implications of this process that speak to a potential dark side of rapid relationality for what it reveals about power and the capacity for change in organizations. While rapid relationality tactics can lead to line managers complying with peripheral experts’ recommendations, the way in which this compliance is achieved requires peripheral experts to conform to the dominant organizational power and status structure. By engaging in rapid relationality, they may be reinforcing the very system that disadvantages them, potentially limiting more radical change in the organization’s culture and power structure.
Even when top managers in organizations invest in bringing in experts to promote change, such experts are often sidelined and appear as window dressing (e.g., Meyer and Rowan, 1977; Westphal and Zajac, 2001; Tilcsik, 2010). This study suggests yet another reason why organizations tend toward inertia and the decoupling of the rhetoric around change used by top managers from the reality of on-the-ground practices. Even when a particular expert group is not sidelined and learns creative ways to effectively get line managers to heed their expertise, how they achieve this influence—by aligning with rather than challenging or subverting the dominant cultural values and organizational power structure—may limit the extent of change in the underlying organizational culture and hierarchy that is part of the problem. These findings are consistent with others that have found internal social activists can drive change by framing it in ways that resonate with their organization, but this may temper the radicalism of their efforts given organizational constraints and activists’ dependency on their organization for employment (Heinze and Weber, 2015; Briscoe and Gupta, 2016).
In addition, the fact that these experts are devoting significant amounts of time and energy to building relationships, rather than utilizing the technical expertise for which they were ostensibly hired, suggests the potential for system-level organizational losses from rapid relationality. It also highlights the asymmetrical nature of relationship building across power divides where the lower-power party performs the majority of relational work, with the higher-power party often oblivious to the behind-the-scenes strategic time- and labor-intensive tactics being utilized. But this time and energy may be well spent if it results in important protections for vulnerable employee groups that experts may be acting on behalf of, as in the case presented here. For those groups, peripheral experts’ early use of rapid relationality tactics may prevent them from becoming victims of conflict between the experts and their own superiors. As organizations continue to turn to expert professional groups to solve pressing problems, it is imperative we understand the processes through which these peripheral experts can effectively influence line managers.
Supplemental Material
DS_10.1177_0001839219827006 – Supplemental material for Rapid Relationality: How Peripheral Experts Build a Foundation for Influence with Line Managers
Supplemental material, DS_10.1177_0001839219827006 for Rapid Relationality: How Peripheral Experts Build a Foundation for Influence with Line Managers by Julia DiBenigno in Administrative Science Quarterly
Footnotes
Acknowledgements
This paper greatly benefited from the insightful feedback of Katherine Kellogg, Lotte Bailyn, Ezra Zuckerman, John Van Maanen, John Carroll, Amy Wrzesniewski, Rene Almeling, Rodrigo Canales, Aruna Ranganathan, Mabel Abraham, Pat Satterstrom, Leslie Perlow, Ruthanne Huising, Phech Colatat, Mae McDonnell, Amanda Sharkey, Melissa Valentine, and Tiona Zuzul. I am also grateful for the comments from audience members and seminar participants in Yale OB, Sociology, and Anthropology, Stanford WTO and SCANCOR, MIT Sloan Economic Sociology Working Group, Rotman, Kellogg, CRAFT, NYU Qualitative Group, JROT 2016, AOM 2016, ASA 2016, and the Davis Conference on Qualitative Research. I am indebted to Forrest Briscoe and three anonymous reviewers for realizing the potential of this work, as well as Linda Johanson and Joan Friedman for their copyediting prowess. This study would not have been possible without the generous support of Jayakanth Srinivasan on all aspects of this research, as well as the soldiers, mental health providers, commanders, and Army and Behavioral Health leaders. This research was supported by grant cooperative agreement W81XWH-12-2-0016. The views and conclusions contained herein are those of the author and do not necessarily reflect the views of the U.S. government or Army.
1
Nearly all mental health providers reported encountering a subset of soldiers for whom psychological testing and reviews of military records revealed exaggerated or fabricated traumas or symptoms, particularly after the U.S. Army changed its policy to provide disability payments for PTSD at 50 percent of one’s salary (increased from 5 percent). Yet even though providers generally estimated this subset to be small, for most commanders, concerns that soldiers were faking sick loomed large as a concern of extreme moral significance given the army’s core values of honor and sacrifice.
2
One may wonder whether providers were successful at getting commanders to regularly follow their recommendations not because they successfully used rapid relationality tactics but because they were coopted such that they only made recommendations commanders would agree to. My data do not support this alternative account. First, in prior work I demonstrated how providers’ clinic colleagues helped anchor them to their clinician identity and prevent cooptation (DiBenigno, 2018). Second, nearly all providers indicated they were concerned about “losing their license” to practice professionally if their recommendations were not followed and they were later sued over an adverse outcome. Although such lawsuits were rare, to help protect themselves, providers carefully documented their recommendations and may have exhibited a more conservative bias to make recommendations favoring patients (not commanders). Third, providers were highly consistent across commanders in the recommendations made for similar types of soldier issues that required work modifications or restrictions (e.g., recommending that soldiers who reported suicidal thoughts have restricted access to firearms). The large subset of dyads for which I have data on the same provider working with multiple commanders allows me to address this concern most convincingly. I did not observe significant variation in within-provider recommendations based on whether the commander followed their recommendations or not.
Author’s Biography
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.