
Abstract
This two-year ethnographic study of the primary care departments in two U.S. hospitals examines how managers can bring about micro-level institutional change in professional practice even when such change challenges professionals’ specialized expertise, autonomy, individual responsibility, and engagement in complex work, which previous research has shown to create difficulties. In this study, managers in both hospitals attempted to implement the same patient-centered medical home (PCMH) reforms among doctors, had the same external pressures for micro-level institutional change, worked under the same organizational and reimbursement structure, and had the same contextual facilitators of micro-level institutional change present within their organizations. But managers in one hospital successfully accomplished change in professional practice while those in the other did not. I demonstrate that managers can accomplish micro-level institutional change in professional organizations using “subordinate activation tactics”—first empowering and motivating subordinate semi-professionals to activate their favorable structural position vis-à-vis the targeted professionals on behalf of managers and next giving semi-professionals positional tools to use in their daily work to minimize the targeted professionals’ concerns about the threats associated with change.
Keywords
Increased globalization, market competition, growth in demand for new business services, emerging expert technologies, and changes in dominant logics, norms, and regulatory regimes are creating pressures for managers of professional organizations to rapidly change professional practice (e.g., Bailey, Leonardi, and Barley, 2012; Brock, Hinings, and Powell, 2012; Morris, Smets, and Greenwood, 2015). In law, globalization has created pressure for new cross-border services (Smets, Morris, and Greenwood, 2012) and forms of organizing (Greenwood and Suddaby, 2006). In finance, increased market competition has created pressure for bigger risk taking (Pernell, Jung, and Dobbin, 2017) and greater work automation (Beunza and Millo, 2014). In architecture, growth in demand for new business services has created pressure for novel types of creative design (Rahman and Barley, 2017) and representation (Retelny and Hinds, 2016). In criminal justice, emerging expert technologies have created pressure for new methods of risk assessment (Brayne, 2017; Christin, 2017) and evidence provision (Bechky, 2017). In science, new logics have created pressure for different laboratory practices (Huising, 2014a, 2014b) and methods for solving scientific problems (Grodal and O’Mahony, 2017; Lifshitz, 2017). And in medicine, changes in norms and regulatory regimes have created pressure for new kinds of training (Kellogg, 2009, 2011a; Beane, 2018) and cross-occupational collaboration (DiBenigno, 2018a, 2018b; Valentine, 2018).
Scholars of work, professions, law, and organizations have shown that managers can accomplish micro-level institutional change in professional practice in response to such pressures using specific direct change tactics, such as engaging professionals in reform programs (e.g., Perlow, 2012; Dobbin, Schrage, and Kalev, 2015) and encouraging them to improvise new practices that address common problems (e.g., Orlikowski, 1996; Smets, Morris, and Greenwood, 2012). But the same scholars have also demonstrated that even when managers use such tactics, they still often fail to change professional practice (e.g., Dobbin, 2009; Currie et al., 2012; Kellogg, 2012). When they fail, it is usually because professionals resist changes that challenge their professional institutions—their specialized expertise (e.g., Abbott, 1988; Waring and Currie, 2009; von Nordenflycht, Malholtra, and Morris, 2015), autonomy (e.g., Bailyn, 1985; Turco, 2012; Ranganathan, 2018), individual responsibility (e.g., Greenwood, Hinings, and Brown, 1990; Cooper et al., 1996), or engagement in complex work (e.g., DiBenigno and Kellogg, 2014; Huising, 2014b). Professionals often resist micro-level institutional change because they believe that such change threatens their ability to honor the professional license that society has given them to protect the public’s safety and welfare (e.g., Scott et al., 2000; Gorman and Sandefur, 2011), even in cases in which strong research evidence suggests the opposite (e.g., Ferlie et al., 2005). For example, Timmermans and Berg (2003) detailed how physicians have resisted using evidence-based medicine in cases ranging from which diagnostic and screening tests to order to when to provide medical or surgical services.
Yet despite the dramatic changes taking place in the professional workforce, researchers have not, to my knowledge, examined how subordinate semi-professionals might help managers change professional practice. The same external pressures that are demanding micro-level institutional change in professional practice have also led to a proliferation of subordinate semi-professions across a wide range of work areas, because they have led managers of professional organizations to redistribute resources on the basis of competence rather than historical workforce hierarchies and roles (e.g., Nancarrow and Borthwick, 2006; Barrett et al., 2012; Currie et al., 2012). In this new environment, organizations are employing subordinate semi-professionals in large numbers (e.g., Susskind and Susskind, 2016; Barley, Bechky, and Milliken, 2017). Law firms are using paralegals to provide legal services in situations that previously required a lawyer (Brooks, 2011), accounting firms have replaced many of their certified public accountants with semi-professional tax preparers who rely on expert technology rather than formal training to deliver services to clients (Galperin, 2017), and universities have substituted administrative coordinators for research scientists with postgraduate degrees to monitor laboratory compliance (Huising, 2014a, 2014b). The lack of research focus on the potential role of subordinate semi-professionals in changing professional practice is understandable, because even managers who have formal authority over professionals often fail to accomplish change (e.g., Greenwood, Hinings, and Brown, 1990; Empson and Langley, 2015). But such failure, in combination with the increasing pressures for managers to change the work practices of professionals inside organizations, makes it imperative to consider new tactics, including those semi-professionals might use to help foster micro-level institutional change.
I conducted a two-year, comparative inductive study of the implementation in River and Harbor (pseudonyms) primary care departments of patient-centered medical home (PCMH) reforms. These reforms being rolled out across the United States require primary care doctors to change their daily work practices by moving from reactive care to prevention and by using evidence-based guidelines with patients who have chronic illnesses (e.g., Rittenhouse and Shortell, 2009). My research aims to understand how, as subordinate semi-professions proliferate inside organizations, managers can accomplish change in a different way with their help. The literature on change in professional organizations provides a good starting point for understanding how.
Micro-level Institutional Change in Professional Organizations
Scholars of professions, law, and organizations have long discussed a wide array of tactics that can be used to accomplish institutional change at the field level (e.g., Powell and DiMaggio, 1991; Scott et al., 2000; Greenwood, Suddaby, and Hinings, 2002). In recent years, there has been an increasing interest in the micro-foundations of institutional change (e.g., Weber, Rao, and Thomas, 2009; Kellogg, 2011a; Powell and Rerup, 2017). Studies have shown that it is possible for managers to accomplish micro-level institutional change using seven relatively direct change tactics: engagement, improvisation, mobilization, legitimation, social accountability, transparency, and contact with groups who will benefit from change. The first three of these tactics enlist professionals themselves to lead change, and the other four tactics persuade professionals to change using other means.
To enlist professionals themselves to lead change, managers can first engage them as participants in reform programs (such as mentoring programs or recruiting programs to increase diversity); if professionals are resisting micro-level institutional change because they do not believe it is important or useful, engaging them can shift their beliefs toward supporting change because people have a strong tendency to avoid cognitive dissonance by changing their beliefs to be consistent with their behavior (Perlow, 2012; Dobbin, Schrage, and Kalev, 2015). Second, managers can encourage improvisation; they can ask front-line professionals to improvise new practices to address problems that arise in everyday work (e.g., Reay, Golden-Biddle, and Germann, 2006; Smets and Jarzabkowski, 2013; LeBaron et al., 2016) and then extend these changes throughout the organization by pragmatically justifying them to a narrow set of peer practitioners (e.g., Valentine, 2018). For example, in their study of a global law firm, Smets, Morris, and Greenwood (2012) showed how managers encouraged English and German lawyers to improvise new practices to address specific breakdowns and opportunities; managers then codified these into best-practice guidelines and spread them to other lawyers concerned with solving specific problems. German lawyers initially resisted the new hybrid practices, but at the urging of their managers to get deals done quickly—and in the face of high financial and reputational costs of failure, which amplified this pressure—they grew more receptive to alternative ways of working.
Third, managers can help mobilize professionals who support reform by creating new roles for them with specific responsibilities for micro-level institutional change (e.g., Lounsbury, 2001; Truelove and Kellogg, 2016), by providing them with injustice frames or new collective identities (e.g., Creed, Scully, and Austin, 2002; Weber, Rao, and Thomas, 2009), or by giving them relational spaces for mobilization (Kellogg, 2009). For example, Kellogg (2011b) detailed how managers helped to mobilize surgical trainees to support a reduction in trainee work hours by framing 120-hour workweeks not as a valuable rite of passage for those training to be doctors but as an example of hospitals compromising patient care by using exhausted surgical trainees as “cheap labor.”
If enlisting professionals in leading micro-level institutional change fails, managers can persuade them to change using legitimation, social accountability, transparency, or contact with groups that will benefit from the change. Legitimation entails managers using discursive tactics, such as theorization (e.g., Greenwood, Suddaby, and Hinings, 2002; Zilber, 2002), rhetoric (e.g., Suddaby and Greenwood, 2005; Anteby, 2010), or naming organizational failings and linking them to potential solutions (e.g., Lawrence, Malhotra, and Morris, 2012). For example, Lounsbury and Crumley (2007) documented how banking managers justified new money-management practices by linking them to microeconomic theory, transforming the low-status art of business finance into the more prestigious science of financial economics. Social accountability tactics require managers to introduce new monitoring and measurement systems (e.g., Kalev, Dobbin, and Kelly, 2006; Ebrahim, Battilana, and Mair, 2014; Kalev, 2014) and to make professionals accountable for their decisions by making their practices known to all (Sauder and Lancaster, 2006; Castilla, 2015). Transparency tactics necessitate managers giving professionals clear information that informs them about opportunities for change (Dobbin, Schrage, and Kalev, 2015). And contact tactics demand that managers increase contact between professionals and groups that will benefit from the change; working side by side can break down stereotypes, which can lead professionals to be more supportive of changes that will help these groups (Kalev, 2009; Briscoe and Kellogg, 2011).
Yet even with this seemingly large arsenal of micro-level institutional change tactics, managers often fail to accomplish change, particularly if professionals have a high degree of autonomy or experience few financial or reputational costs associated with not changing. Researchers have shown that organizational managers faced fierce resistance from autonomous professionals as they tried to get frontline managers to change their hiring and promotion practices (e.g., Dobbin, 2009); army commanders to change their use of behavioral health services (DiBenigno, 2018); bankers to change their lending practices (Canales, 2014; Canales and Greenberg, 2015); scientists to change their use of chemicals (Huising, 2014a; Howard-Grenville et al., 2017) or means of solving scientific problems (Levina, Fayard, and Gkeredakis, 2014; Lifshitz, 2017); and clinicians to change their clinical trials practices (Heimer and Gazley, 2012), their training practices (Kellogg, 2012; Beane, 2018), or their diagnostic practices (McPherson and Sauder, 2013; Pine and Mazmanian, 2017). Yet managers are often tasked with accomplishing micro-level institutional change in professional practice in contexts in which professionals have a high degree of autonomy or experience few financial or reputational costs for not changing. This is where subordinate semi-professionals working closely with the professionals could play a role.
To date, scholars have not examined the role of subordinate semi-professionals in helping managers change institutionalized professional practice. When scholars do mention their role in change without the involvement of managers, they discuss it in terms of the hiving off of dirty work, in which professionals themselves choose to delegate less pleasant or stigmatizing work to semi-professionals with lower status (e.g., Huising, 2014b; Kellogg, 2014; Kaplan, Milde, and Cowan, 2017). Or scholars show change as stemming from semi-professionals in staff positions outside of the flow of professionals’ daily work, such as personnel officers, who introduce new bureaucratic solutions for reform that they learn from their network contacts, professional journals, or conferences (e.g., Dobbin, Kim, and Kalev, 2011; Perlow and Kelly, 2014). They have neglected how semi-professionals’ favorable structural position vis-à-vis professionals makes them an untapped resource for manager-led change.
Subordinates’ Favorable Structural Position
The same external pressures that are demanding micro-level institutional change in professional practice have also created pressures for managers of professional services organizations to delegate tasks that have traditionally been performed exclusively by professionals to subordinate semi-professionals (e.g., Nancarrow and Borthwick, 2005; Barrett et al., 2012; Currie et al., 2012). The ranks of subordinate semi-professionals—unorganized bodies of bureaucratically employed workers who do not apply esoteric knowledge to particular cases, do not enforce some kind of code of ethics, and do not rely on fees for service (e.g., Vallas, 1993; Barley, 1996; Abbott, 1998)—are growing rapidly.
Sociologists have shown that subordinates can assume and wield considerable power and influence despite having no formal authority to do so (e.g., Crozier, 1969). Their informal influence is derived from a structural position in the organization that gives them control over important resources (Emerson, 1962; Pfeffer and Salancik, 1978; Fligstein, 1990). Subordinates may play a central role in an information or friendship network (e.g., Kanter, 1993; Battilana and Casciaro, 2013), perform tasks that are critical for others (e.g., Crozier, 1969), or control uncertainty stemming from the external environment (e.g., Brass and Burkhardt, 1993).
But network theorists have demonstrated that actors may not be willing to activate their structural position in a network if they don’t feel comfortable calling on their contacts for help (Casciaro and Lobo, 2008; Bunderson and Reagans, 2011; Smith, Menon, and Thompson, 2012; Gulati and Srivastava, 2014). Even if actors are willing to activate their structural position, they may not have the ability to do so if their contacts fear some kind of loss involved in helping them, such as a loss of identity or status, and refuse to give them assistance (Smith, 2005; Burt and Merluzzi, 2014). If managers can find ways to increase subordinate semi-professionals’ willingness and ability to activate their favorable structural position vis-à-vis professionals on behalf of managers, they may be able to successfully change professional practice.
Methods
To develop a rich understanding of micro-processes involved in how managers can bring about change in professional practice inside organizations, I conducted a comparative ethnographic study of the primary care departments of River and Harbor hospitals. Using an inductive approach that is well suited for developing new theory (e.g., Van Maanen, 2011), I examined managers’ attempts to change doctors’ practices in the two organizations, which were well matched on the contextual and organizational factors that have been shown to be important to accomplishing micro-level institutional change in professional organizations. The contextual factors include professional associations taking an active role in promoting reforms (Greenwood, Suddaby, and Hinings, 2002; Lounsbury, 2002), growth in demand for new services (e.g., Greenwood and Suddaby, 2006; Morris, Smets, and Greenwood, 2015), financial or reputational costs associated with not adjusting (e.g., Greenwood, Suddaby, and Hinings, 2002; Sauder and Espeland, 2009; Lockett et al., 2012), reform-related attacks on the legitimacy of the profession and organizations within it (e.g., Hoffman and Jennings, 2011; McDonnell, King, and Soule, 2015), and legal enforcement of reforms (Kalev and Dobbin, 2006).
River and Harbor were both exposed to all of these contextual factors, but the pressures for change were fairly weak. In 2002, the American Academy of Pediatrics defined the patient-centered medical home (PCMH) concept, a care delivery model in which patient treatment is coordinated through the primary care physician to ensure that patients understand and receive necessary care when and where they need it. In 2007, along with three other U.S. primary care professional organizations (the American Academy of Family Physicians, the American College of Physicians, and the American Osteopathic Association), it created pressure for change by crafting joint principles for PCMH reform (Rittenhouse and Shortell, 2009). By the time of my study, four accreditation organizations used the same published standards to accredit sites implementing PCMH; however, PCMH accreditation was not supported by financial incentives in most accredited sites (Edwards et al., 2014). My interviews showed that doctors at both River and Harbor perceived only weak field-level pressures to implement PCMH. There was no growth in demand for reform-related services, no financial or reputational costs associated with not adjusting, no reform-related attacks on the legitimacy of the profession, and no legal enforcement of reforms.
The organizational factors that have been shown to facilitate change in professional practice fall into three categories: resources, internal support for change, and other micro-contextual supports. Regarding resources, large organization size (e.g., Kelly, 2010) and monies dedicated to change (e.g., Cooper et al., 1996; Greenwood and Suddaby, 2006) have been shown to be important. River and Harbor were part of the same parent organization, did similar work, and employed doctors and clinical staff with similar backgrounds. Both received new resources for change in the form of grants of $750,000 at the same time to implement the same PCMH reforms. River was larger than Harbor. While some scholars have pointed out that larger organizations may have more resources (staff and infrastructure) to implement reform successfully, River and Harbor received the same resources to implement PCMH. Because Harbor was smaller than River, serving roughly two-thirds of the primary care patient population served at River, Harbor managers thus received a greater level of resources per patient.
Regarding internal support for change, factors that have been shown to be important are a governance system in which change agents have formal authority over change targets (Cooper et al., 1996), managers with change capabilities (e.g., Lockett et al., 2012; Smith and Besharov, 2017), a supportive corporate culture for change (e.g., Kelly and Kalev, 2006; Dobbin, Kim, and Kalev, 2011), network connections between users of new change methods outside the organization and non-users inside (e.g., Jennings and Zandbergen, 1995; Kelly and Dobbin, 1998; Dobbin, 2009), and internal reformers (e.g., Kelly and Dobbin, 1998; Lounsbury, 2001; Kellogg, 2011a).
The medical directors had formal authority over the doctors in their departments but, as in other organizations governed by medical professionalism, theirs was less a traditional, hierarchical relationship than an ambiguous and negotiated relationship among professional peers (e.g., Empson and Langley, 2015). The medical directors at River and Harbor had been elected by their peers to the formal leadership role for a fixed term of office and could be deposed at their peers’ discretion. Including the medical director, there were five clinical managers in the primary care department at River and three at Harbor. At each hospital a non-clinical operations director assisted the clinical managers in day-to-day administrative tasks. In addition to their administrative tasks, all clinical managers saw patients.
The clinical managers, who had been appointed by the medical directors to lead change informally in line with PCMH reforms (with part of their salaries funded by the grant monies), had no formal authority over the other doctors. All staff members except doctors (e.g., nurses, medical assistants, and secretaries) formally reported to the medical director and operations director. To minimize the use of multiple terms, I use the term “manager” to refer to all of the managers. River and Harbor also appointed a doctor on each patient care team (six at River, four at Harbor) to be an informal “team leader” whose charge was to work with the other team members (doctors, nurses, medical assistants, and secretaries) to implement the changes required by PCMH. A small part of the team leaders’ salaries was funded by the grant monies. River and Harbor managers had similar levels of experience in leading change efforts and had access to the same experts from the granting agency who provided ongoing advice. Other staff members at the two hospitals—nurses, medical assistants, and secretaries—also had similar skills and backgrounds.
River and Harbor both also had supportive cultures for change; both had applied for the grant, and the granting agency related that it had given grants to organizations with histories of successful change efforts. River and Harbor managers had the same set of network connections. They were part of the same parent organization and were part of the same network of grantees attempting to implement PCMH reforms.
Doctors at both hospitals did both clinical work and research. On average, they saw patients for 3–4 four-hour clinical sessions each week (out of 10 total weekly sessions). Each doctor was supported by one medical assistant (MA). MAs each worked for the same 3–4 staff doctors on a regular basis. Depending on patient volume, each team contained 7–9 staff doctors, 2–3 MAs, 2–3 nurses, and 4–5 secretaries. Staffing ratios were similar at the two hospitals.
Ethnographic Data Collection
I focused my data-collection efforts at the two hospitals on observing interactions among managers, doctors, and staff to better understand how managers attempted to influence doctors to change their practices. I observed day-to-day work for three months before River and Harbor managers began to try to influence doctors to change their practices. I then watched managers’ attempts to implement change for 24 months, by which time River and Harbor had developed consistent patterns. I drew on three data sources—observations, informal interviews, and documents used by managers—to capture change attempts, change outcomes, and the factors that shaped these attempts and outcomes.
Observations
To establish a baseline for determining how changes in doctors’ practices occurred, for the first three months, before the introduction of any reform-related changes, I focused my research on documenting traditional day-to-day practices at River and Harbor. During these initial observations, I noted that managers were the key players involved in the strategy and discussions with doctors regarding PCMH. Doctors and medical assistants (MAs) were the key players involved in the day-to-day changes in line with the reforms. Once I saw this, I began to focus most of my observations on the interactions among the managers, doctors, and MAs (6 managers, 28 doctors, and 15 MAs engaged in the study at River and 4 managers, 20 doctors, and 9 MAs engaged in the study at Harbor). I studied all managers and MAs in each department, and the number of doctors I focused on in each was proportional to the size of the department. I paid particular attention to their interpretations of why they were acting the way they were.
To examine how micro-level institutional change attempts unfolded at the two hospitals, for the next 10 months I spent 5+ hours per week at each site observing members in the daily clinics and in meetings related to the reform. I also socialized with the group members: I regularly ate breakfasts and lunches with them, and fraternized with them when they took breaks in the clinic rooms, conference rooms, and one another’s offices.
After 13 months of observation, the work practices targeted for reform were changing much more quickly at River than at Harbor. Therefore I scaled back my time at Harbor to 2+ hours per week for the final 14 months of fieldwork. At River, where the targeted work practices were still undergoing rapid change, I continued to spend 5+ hours per week onsite. At both hospitals, I varied my days and times of observation. This enabled me to focus on the quickly changing work practices at River while continuing to follow the less quickly changing work practices at Harbor.
To understand both traditional and new work practices, and how managers attempted to influence doctors to change, I conducted 1- to 2-hour sessions shadowing managers, doctors, MAs, and secretaries. Over the course of the study, I conducted 566 shadowing sessions at River (139 manager, 197 doctor, 189 MA, 26 nurse, and 15 secretary shadowing sessions) and 370 at Harbor (79 manager, 158 doctor, 105 MA, 15 nurse, and 13 secretary shadowing sessions). I shadowed them in the clinics as well as in meetings in which the reforms were discussed (e.g., manager meetings, doctor staff meetings, MA staff meetings, cross-functional transformation team meetings, and care team meetings). I took extensive notes during my observation sessions. During my shadowing in clinics, I took detailed notes by hand, which I typed up within 24 hours. During my shadowing in meetings, I typed notes directly into the computer.
Informal interviews
I conducted informal interviews to understand five main issues: organization members’ backgrounds, career histories, and goals; members’ views of key dimensions of work; their descriptions of their daily work practices; the doctors’ use of the PCMH reforms; and particular key incidents they perceived to be related to the micro-level institutional change in doctors’ practices that I had observed. Interviews took place during breaks in daily work, lasted between 10 and 30 minutes depending on how busy the day was for a member, and took place in private settings—clinic rooms or conference rooms. When I shadowed a particular member, I was often able to briefly interview other team members directly before or after my shadowing session. For most interviews, I typed notes into the computer in real time; otherwise, I took detailed notes by hand, which I typed up within 24 hours.
Documents
I drew on organizational documents to check my impressions from observations and interviews about the factors shaping micro-level institutional change attempts and outcomes over time. I had access to documents that River and Harbor department members used in day-to-day work and to others that were circulated in the meetings in which the reforms were discussed. These included PowerPoint presentations, forms, clinic paperwork, and materials developed by the managers and care teams to facilitate PCMH.
Data Analysis
I used a comparative, longitudinal research design to investigate how managers can bring about micro-level institutional change in professional practice. In my inductive, open-ended analysis, I traveled between the data and the literature and emerging theory. In this process of gradual abstraction, I categorized raw data, linked categories to themes, and aggregated these into a theoretical framework (e.g., Glaser and Strauss, 1967; Miles and Huberman, 1994). Data analysis occurred in several steps.
First, during data collection, I performed coding focused on understanding micro-level institutional change in doctors’ practices (or not) in line with the reforms at River and Harbor. Each week, I uploaded my field notes, interview notes, and department documents by hospital and date into Atlas.ti, a qualitative coding software program, and I coded the notes. This coding led me to identify four important themes, about which I wrote weekly memos: (1) difference between managers and doctors in views of PCMH at both River and Harbor; (2) doctors’ resistance to managers’ attempts to influence doctors to change their practices in line with the reforms at both hospitals; (3) managers’ tactics enlisting MAs to influence their doctors on the managers’ behalf at River but not at Harbor; and (4) variation in success over time of managers’ attempts to accomplish this micro-level institutional change at River.
Second, while I was in the field, I saw clearly that there was variation in River doctors’ practices over time; that there were three breakpoints in River managers’ micro-level institutional change tactics; and that the River doctors’ changes in practice were linked to managers empowering MAs and giving them positional tools to influence doctors on the managers’ behalf. After I left the field, I focused specifically on the tactics used by managers at River and Harbor to implement micro-level institutional change. I first coded the data for breakpoints to define periods of managers’ different change tactics at the two hospitals. The data showed one key breakpoint viewed by managers at both River and Harbor as a crucial disjuncture: the one-and-a-half-day “Learning Session” hosted by the granting agency, during which reform advocates gave presentations and led discussions related to how managers could influence doctors to implement PCMH reforms. I took this breakpoint to mark two phases of micro-level institutional change that occurred at both River and Harbor: Phase 0 began at the start of my observations, before any managers’ change attempts around PCMH (10/2012); Phase 1 began with the Learning Session, which led managers to begin to attempt change in doctors’ practices (1/2013).
The data showed two additional key breakpoints identified by managers at River. Each of these breakpoints occurred when River managers reached out to external contacts in their network in an effort to find out how to employ MAs to help implement PCMH reforms. Breakpoint 2 at River (11/2013; beginning of Phase 2) occurred when managers, using information they had obtained from a contact familiar with the use of MAs to influence doctors at Lakeview (a pseudonym), began to use empowerment tactics with their own MAs. Breakpoint 3 (7/2014; beginning of Phase 3) at River occurred when managers, after reaching out to Lakeview contacts directly, learned about the importance of giving MAs concrete materials to help them change doctors’ practices and began to use what I call positional tools.
Third, to track month-by-month micro-level institutional change outcomes, I used data from the 28 doctors at River and 20 doctors at Harbor on whom I focused my observations. I did not include doctors who were also managers. The River and Harbor IT systems did not capture data that could be used to measure the degree to which daily work processes changed. And I was not able to use observational data from visits to track the degree to which each of the different work processes changed because I was not able to see if a patient was due for a test but the doctor did not order it. For example, I was able to see if the doctor did get a patient who was due for a colonoscopy to schedule this test before leaving the office, but I was not able to see if a patient was due for a colonoscopy and the doctor did not get the patient to schedule it before leaving the office. For this reason, I used observations in meetings during each month and interviews with doctors and MAs to track whether doctors in the group had changed their practices in line with each of the PCMH reforms. The biweekly care team meetings and transformation team meetings were focused on increasing reform implementation and, as part of their discussion of how to better implement the reforms, doctors and MAs publicly discussed which doctors on their teams were implementing each of the reforms. In addition, in my interviews, I asked doctors to privately report whether they had changed their practices in line with the reforms and asked MAs to privately report whether they perceived that their doctors had changed their practices in line with the reforms. I checked public reports by doctors and MAs in the care team meetings and transformation team meetings against private reports by doctors and MAs in interviews. The reports were consistent with one another at River and for the first two phases at Harbor. In Phase 3 at Harbor, private reports by doctors and MAs were consistent with one another, so I used these private reports to track Phase 3 Harbor outcomes; as I explain below, with increased pressure on accountability, public reports in meetings differed from private reports during this phase at Harbor. After leaving the field, I checked my conclusions with informants from River and Harbor in informal meetings to ensure that these interpretations represented their experiences. These checks did not affect informants’ actions during the study.
Difference in Micro-level Institutional Change Outcomes at River and Harbor
While managers—doctors who played managerial roles in their departments—at both River and Harbor faced substantial barriers to changing doctors’ practices in line with PCMH reform, by the end of my study, River managers had successfully brought about micro-level institutional change in doctors’ practices while Harbor managers had not. These changes, based on the outcome measures discussed above, are displayed temporally in table 1.
Changes in Doctors’ Practices at River and Harbor (Doctors’ Monthly Use of PCMH Reforms)
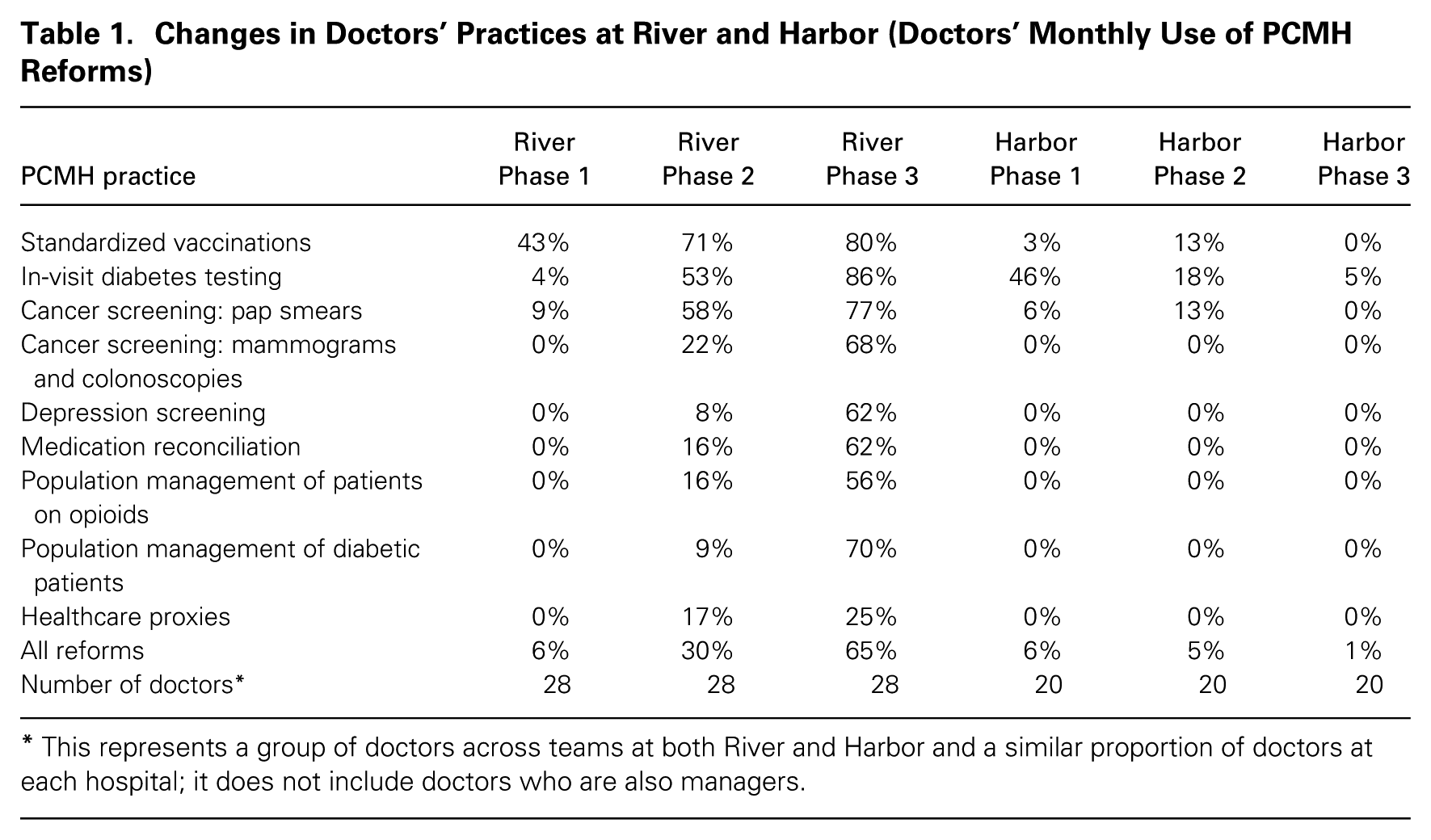
This represents a group of doctors across teams at both River and Harbor and a similar proportion of doctors at each hospital; it does not include doctors who are also managers.
In Phase 0, managers had not yet attempted to implement the reforms, and doctors and staff members worked in traditional ways. In Phase 1, although both River and Harbor managers implemented the reforms with their own patients, and although doctors at both sites were happy to implement the first new reform process (as described below), managers were unsuccessful in their attempts to influence the doctors to implement other new processes. In Phase 1, the average monthly percentage of doctors who changed their practices in line with the reforms (who were not also managers) at both River and Harbor was 6 percent. Harbor’s monthly usage rate of PCMH reforms remained low for the rest of the study (5 percent in Phase 2 and 1 percent in Phase 3), while River’s increased over the next two phases. In Phase 2, River managers were somewhat successful in influencing the doctors, achieving an average monthly usage rate among doctors of 30 percent. In Phase 3, River managers were highly successful, achieving an average monthly usage rate of 65 percent.
Phase 0: Historical Work Structures and Processes
The River and Harbor primary care departments were organized like typical doctors’ offices in the community setting, except that they were larger. At River, the department was divided into six teams, each with a secretarial desk, a patient waiting area, and a set of clinic rooms. The department at Harbor, which was divided into four teams, was set up similarly.
In both hospitals, doctors, nurses, medical assistants, and secretaries were each permanently assigned to a team, and each team took care of the patients seen by the doctors on their team. Secretaries took incoming calls, booked appointments, and directed other calls to the appropriate members of the clinical staff. Medical assistants (MAs) brought patients from the waiting room to the exam room, weighed them, took their blood pressure, and left them in the exam room for the doctor to arrive. Nurses were not involved in supporting the clinic workflow of doctors; instead they spent their time triaging patients who called in, giving injections, and preparing prescriptions for doctors to sign. Throughout the day, doctors saw patients in “sick visits,” scheduled for 15 minutes, and in longer “annual visits.”
River and Harbor received large outside grants at the same time to help them implement patient-centered medical home (PCMH) reforms. Managers at both River and Harbor tried to persuade fellow doctors to adopt a host of new practices in line with a particular set of PCMH reforms: (1) standardize delivery of vaccinations; (2) standardize delivery of pap smears; (3) schedule colonoscopies and mammograms for cancer screening before the patient leaves the office; (4) conduct depression screening; (5) review and reconcile medications; (6) conduct in-visit diabetes testing; (7) engage in population management of patients on opioids; (8) engage in population management of diabetic patients; and (9) get patients to sign healthcare proxies.
A small number of doctors at River and Harbor, who had been at their respective hospitals for many years and were highly committed to traditional ways of working, were adamantly opposed to the PCMH reforms, but the majority of doctors at River and Harbor believed that the reforms had merit. Even so, they were concerned that the day-to-day changes the reforms required them to make in their practice ran counter to their ability to apply their specialized expertise to help patients, use their discretion and autonomy in treating patients, take individual responsibility for patients, and engage in complex work within their jurisdiction to protect the public’s health, safety, and welfare. In addition, the doctors did not feel a sense of urgency to change because neither regulatory agencies nor their patients were demanding that they implement PCMH reforms. Furthermore, there were no reputational or financial consequences for the doctors associated with failing to change.
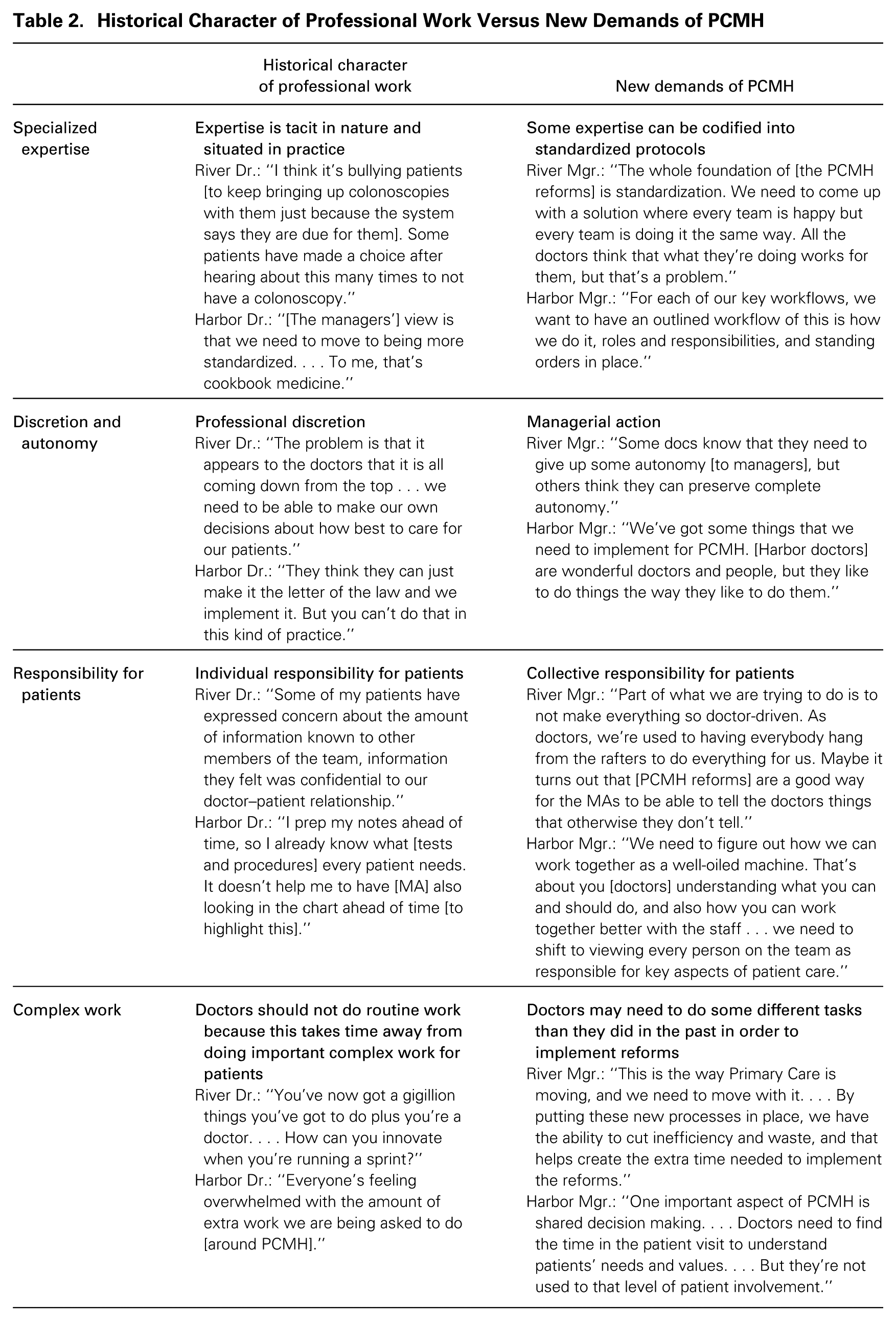
A handful of doctors at River and Harbor exhibited a high level of support for the reforms—the managers. Because they themselves were doctors, they were committed to using managerial practices that would complement rather than interfere with their colleagues’ existing work practices wherever possible. These managers believed in the importance of standardized processes to complement doctors’ specialized expertise, the idea of using managerial direction to complement professionals’ discretion and autonomy, the worth of promoting collective responsibility for patients to complement doctors’ taking individual responsibility for patients, and the importance of doctors doing non-traditional tasks in line with the reforms to complement their engagement in complex work within their jurisdiction. Table 2 sketches the differences between River and Harbor’s traditional professional work and the demands of the new practices. In addition to believing in the value of the reforms, the managers also had career incentives to implement them. The PCMH reforms they were seeking to implement were consistent with the departmental goals that had been set by top managers at each hospital; because River and Harbor were part of the same parent organization, their departmental goals were very similar. Finally, the managers were socially accountable for PCMH implementation because managers from all of the sites involved in the grant reviewed their progress with one another twice a year, which allowed for peer comparison.
Historical Character of Professional Work Versus New Demands of PCMH
Phase 1: Failed Micro-level Institutional Change Using Direct Tactics
In January 2013, managers and team leaders at both hospitals attended the “Learning Session” held by the granting agency. Reform advocates gave presentations and hosted discussions about how managers could influence doctors to implement PCMH reforms. Reform advocates at the granting agency believed strongly in the importance of engaging doctors to improvise new processes, and requirements for doctors’ engagement and improvisation were built into the grant. In accordance with grant requirements, managers at both River and Harbor set up biweekly care team meetings for the doctors, nurses, MAs, and secretaries to discuss process improvement ideas related to PCMH. Before this change, these cross-functional groups of staff members, who worked together every day, had very rarely talked with one another outside of their interactions during busy clinic sessions. At the learning session, reform advocates had suggested that managers pick a theme to organize process improvement efforts across their departments, and they had given as examples the reforms of delivering needed vaccinations and of performing needed diabetes testing.
In Phase 1, at both River and Harbor, the managers used engagement, improvisation, and social accountability in care team meetings to develop and implement new processes. River’s first reform effort focused on increasing the rate at which patients received needed vaccinations. Harbor’s first reform effort focused on increasing the rate at which patients received needed in-visit diabetes testing. Most doctors at both River and Harbor were initially willing to use the care team meetings to improvise a new process that they thought would be helpful in improving operations on their teams.
Historically, at both River and Harbor, when patients were overdue for vaccinations, in-visit diabetes testing, pap smears, colonoscopies, or mammograms, expert software in the electronic medical record (EMR) had flagged this for doctors. But with all of the other things that the doctors needed to do in patient visits, doctors sometimes did not administer preventative services such as vaccinations and screening services such as cancer screening. At River, the teams developed a new process in which the MA (rather than the doctor) did “pre-visit work” the day before each patient’s visit, reviewing the part of the patient’s EMR dealing with vaccinations to determine whether the patient was due for vaccinations. The team created the new tool of a “huddle sheet” that the MA could use to mark vaccinations needed by each patient scheduled for a visit the following day. The next day before the beginning of the clinic session, each MA met with their doctor in a two- to three-minute “huddle” to briefly review vaccinations due for each patient. The huddle sheet minimized threat to doctors’ expertise because doctors could choose to approve vaccines or not. If the doctor agreed, the MA (rather than the doctor) informed the nurse, who delivered the vaccination to the patient. The new process allowed the nurse to deliver the vaccination to the patient before the patient went in to see the doctor if the doctor was running late. This increased the likelihood that patients would not leave the office before receiving needed vaccinations.
At Harbor, the teams developed a new process in which the MA (rather than the doctor) did “pre-visit work” the day before each patient’s visit, reviewing the part of the patient’s EMR dealing with diabetes testing to determine whether the patient was due for this testing. Historically, with all of the other things that the doctors needed to do in patient visits, doctors sometimes did not do needed diabetes testing. The team created the new tool of a diabetes testing order form, and the MA (rather than the doctor) ordered in-visit diabetes testing by filling out the order form and placing it on top of the patient’s paperwork for the doctor. This minimized the threat to doctors’ expertise because doctors could choose to use the order form or not. If the doctor agreed, the doctor sent the order form with the patient to check out, and the secretary sent the patient to the lab to have blood drawn for the tests. This increased the likelihood that patients would not leave the office before receiving needed diabetes testing.
River and Harbor managers measured the implementation success of these processes to increase social accountability for implementation. The River and Harbor IT systems did not capture data that could be used to measure the degree to which daily work processes changed. But the managers wanted teams to learn from short-term feedback so that team members could try different approaches, if necessary, and so that they would be socially accountable for implementation. To provide these data, managers asked care team members to count, respectively, the number of vaccines given or the number of diabetes order forms used. These data were not meant to measure clinical outcomes for patients, merely to give a general idea of how well the new processes were working.
River and Harbor managers successfully engaged doctors to improvise a new process around the first PCMH reform they attempted. And some doctors asked their MAs to expand their work within this same new process to include highlighting vaccinations, in-visit diabetes testing, and pap smears. But when managers asked doctors to improvise a second new process around a reform related to high-risk patients (population management of patients on opioids or of diabetic patients, or the establishment of healthcare proxies), doctors resisted. Although doctors had been energized by working with staff in the newly established care team meetings to design and implement the first reform, they were not motivated to take on a second reform related to high-risk patients. A River doctor said, “With PCMH and [two other reforms coming from the Centers for Medicare & Medicaid Services], so many people are telling doctors what to do that it becomes dispiriting. We’re feeling stressed out and distracted. There’s no sanctity of cognition for medical decision making . . . it’s just a barrage of expectations.” A Harbor doctor noted, “A lot of my patients are elderly and have a lot of serious medical conditions. I don’t have enough time in the visit to cover everything I need to with them and do [multiple PCMH reforms].” Doctors at both sites felt that creating and implementing a second process around high-risk patients would prevent them from engaging in the complex work they needed to do with patients during the visits.
In Phase 1, River and Harbor managers also tried to use mobilization tactics with reformer doctors and reformer staff members, with the hope that these reformers would help others to implement the changes. According to grant requirements, managers at both River and Harbor established meetings of cross-functional teams of doctors and staff members who were supportive of PCMH changes (which they called transformation teams). In doing so, managers created relational spaces (Kellogg, 2009) in which supportive doctors could meet with supportive nurses, MAs, and secretaries apart from defenders of the status quo.
According to the literature, getting these reformers together should have helped them develop a sense of efficacy for micro-level institutional change and new relational frames and identities supporting change. These, in turn, should have facilitated the use of new processes outside of the transformation team meetings. At both River and Harbor, managers worked with transformation team members to develop a new process around the reform of looking at each doctor’s total population of diabetic patients (rather than looking only at diabetic patients coming in for visits on that particular day) and testing and treating them according to evidence-based guidelines. At both sites, the new process required MAs to use a tool already available in both sites—the software program PopulationCare (a pseudonym), which facilitated standardized in-visit diabetes screening—to identify the diabetic patients in each doctor’s full population of diabetic patients who were overdue for testing, review this list of patients with the doctor, and call patients to get them to come in for needed testing or a new treatment plan.
But when transformation team members tried to implement the new process on their teams, they failed. The transformation team members were drawn from across their respective departments and did not work together on the same care team. To implement the new processes, they depended on the work of others on their care teams who were not on the transformation team and were not mobilized to implement change. Doctors who were not on the transformation team were not willing to implement a process designed by others that they felt threatened their specialized expertise and autonomy. One Harbor doctor said, “I don’t agree with the guidelines built into the system.” A River doctor exclaimed: I’m revolting inside against this. It’s part of this one-size-fits-all, push-everything-down-on-us idea. Just the other day someone sent us something about joy in practice. Well, it’s not very joyful to be told how to do everything. We’re talking about doing team-based care, but really it’s only team-based care if we decide that we’re doing it exactly the way you say.
Even doctors who were on the transformation team could not persuade their own MAs to take on the extra work required by the reform. One reformer doctor at Harbor said, “It’s been tough getting others on my team to try [the new processes]. The doctors can’t see their way into it, and the staff don’t want to be adding anything new.” A reformer doctor at River said, “My MA is just not interested. She’s not doing any [pre-visit work].”
Phase 2: Empowerment Succeeds—And Fails
After change stalled at both River and Harbor, the operations director at River and the medical director at Harbor each sought expert help. The directors’ past work experience shaped the kind of help they sought, and each got different kinds of advice. As a result, in Phase 2 (11/2013–6/2014), River and Harbor managers used different sets of change tactics that generated different results. River managers were moderately successful in reforming doctors’ practices in line with PCMH, with an average monthly reform usage rate of 30 percent. Harbor managers in this phase achieved only a 5-percent monthly average rate of usage.
Empowering MAs at River
When direct change tactics failed at River, its non-clinical operations director contacted someone she thought might have experience with using MAs more actively to implement PCMH. “I used to work in community health where MAs played a bigger role,” she explained to me. “Whenever we wanted to introduce a new process, we knew that we needed to get the MAs on board. . . . [So, when the doctors resisted PCMH], I got in touch with the operations director at [a community health center owned by the same parent organization] to see what they were doing with their MAs around PCMH.”
The community health manager told the River manager that she had not yet begun trying to promote practices in line with PCMH but that Lakeview (a pseudonym), an organization of multiple suburban medical practices, was getting its MAs to influence the doctors. This contact also mentioned Lakeview’s practice of allowing MAs to meet together—apart from managers—to suggest and discuss process changes. The River manager told me, “Lakeview went at it with a vengeance. They restructured their entire clinical staff, got rid of nurses, and added MAs. . . . Their MAs play an important role in getting the doctors to [use the reforms].” I was in the meeting when the River operations director mentioned to the other managers that Lakeview had involved MAs in this way. From my field notes:
We’ve been pushing things to the doctors. But many of the doctors will take the lead from their MAs. . . . I’ve heard that they’re doing a lot with MAs up at Lakeview.
That might be more effective than one of us saying [to the doctors that] they need to shift gears.
But will the MAs be comfortable telling their docs to do things?
I don’t think they’ll mind doing it if they see it is helping their doctors.
Frames and rewards
I observed MA staff meetings at both River and Harbor in which groups of four to seven MAs met with one or two managers. The meetings took place in a conference room apart from the daily work sites and in two shifts to ensure coverage on the teams. In the Phase 1 staff meetings I observed at both River and Harbor, MAs were inhibited in their responses. Consistent with their low status, they filed into the meetings without speaking, sat upright and unsmiling during managers’ announcements, and rarely asked questions or made comments in response. As one River MA remarked to me, “You can’t expect people to speak up in meetings. Many of the MAs are scared and fearful. . . . A lot are single mothers . . . so there’s no fallback.”
In Phase 2, River managers began to allow the MAs to meet with one another at the beginning of staff meetings, before the managers arrived, and I observed these meetings too. These MA-only portions of the staff meetings helped facilitate positive emotion around influencing the doctors to change practices. “I love it that you can put things out there and hear other people are feeling the same way,” one MA told me. “Then you know you’re not the only one who isn’t sure how to do all of these new things.”
In Phase 1, before the River managers began to give the MAs information about how they could prompt their doctors to use the reforms, the MAs had a particular cognitive frame regarding the purpose of their work—to support the doctor in clinic by adapting to the doctor’s idiosyncratic task demands. In Phase 2, the River managers offered the MAs both new frames that helped change their perceptions about influencing their doctors and information that guided them in how to do this. One frame the managers used was that MAs who influenced their doctors would be helping their doctors deliver better patient care. In one Phase 2 meeting, a manager explained, “You’re helping their clinical care by doing it. The whole idea is that you use [the PopulationCare software to] find your doctors’ [diabetic] patients and look at what [tests] they are overdue for. For patients who are overdue for testing, you focus on making sure they get these tests [by telling the doctor this in the pre-session huddle].”
The River managers also gave the MAs new resources and rewards in Phase 2 that both freed up time for them to engage in the new work associated with influencing the doctors and increased their interest in acting on behalf of the managers. The managers established a two-way dialogue that allowed MAs to tell the managers about the hurdles they were facing and the resources they needed to address them. Initially, MAs did not see why it was in their interest to try to influence doctors to do what the managers wanted. Soon, though, in the MA-only part of the meetings, highly skilled MAs with long tenure in the organization began to focus the other MAs on desired resources and on the potential rewards of acting on behalf of the managers. For example, it was the traditional practice in both hospitals to cover staffing shortfalls by rotating MAs from one area of the department to another. Under such rotation, MAs experienced work intensification because they could not use downtime between doctors’ sessions to catch up on non-visit-based work. The MAs discussed this in the MA-only part of the meetings and raised this issue with the managers in the MA-manager part of the meetings. The managers responded by eliminating rotation of the MAs.
MAs’ favorable structural position
River managers’ decision to enlist the MAs to influence the doctors was not a well-accepted practice in primary care. My informants at River and Harbor told me that the MAs had traditionally served as the “maître d’s of primary care,” greeting patients in the waiting room, walking them back to the exam room, weighing them, taking their blood pressure, and then leaving them in the exam room to wait for the doctor. At River and Harbor, they were predominantly female, African American and Hispanic, with an average tenure of less than five years, and no college degree. Their median salaries at River and Harbor were $18.15 and $18.24 per hour, respectively (roughly $38,000 per year).
But while MAs had a low formal position and low status at both River and Harbor, they occupied a favorable structural position vis-à-vis their doctors. Historically, MAs had been very valuable to doctors because they helped to optimize patient flow through the visit. MAs’ flow management allowed doctors to see more patients and thus helped increase revenue for both doctors and the practice as a whole. The MAs’ central position in the doctors’ workflow also gave them access to and potential control over resources such as information about patients’ problems; they were the ones who gave the doctors significant data about patients, such as vital signs and current complaints. In addition, MAs were central in the doctors’ peer network. Each MA worked for several doctors on the team, and MAs often passed information to doctors about what other doctors on the team were doing. Finally, MAs were positioned between the patients and the doctors, so they could help to shield the doctors from some of the challenges associated with upset or angry patients.
Empowerment at River runs into roadblocks
The tactics the River managers used to empower subordinates initially gained traction but ultimately failed. While they provided the MAs with the willingness to act on behalf of managers, they did not give them the ability to act. The handful of River MAs who successfully influenced their doctors across multiple reforms during Phase 2 were those with the highest technical and political skill; they had their own abilities for action. For all their efforts, most River MAs failed to implement the majority of the reforms. The reform that required doctors to screen patients for depression according to evidence-based guidelines provides a good example. River managers suggested that the MAs do a brief depression-screening test with the patient and then enter the results into a “shared note” in the patient’s EMR started by the MA and added to by the doctor. If the patient scored high on the brief screening, the doctor would see this in the shared note and could then administer the longer version of the test during the visit. Most MAs failed to persuade their doctors to implement this reform. Doctors were very aware that their notes were legal records and must be precise because these documents might one day have to stand up in a court of law. One doctor explained that he did not want any inconsistencies in his patients’ records: “A lot of us don’t want to make that move from ‘I am perfectly fine. Everything is being done correctly, and I know it,’” he told me. “Every box is checked, and anything not done has my extensive note explaining why.” He believed that the new process posed a threat to his ability to take individual responsibility for patients.
Five of the 15 River MAs were successful in overcoming their doctors’ resistance in Phase 2. These five were more highly skilled than the others as measured by a combination of three indicators: salary rate, number of years as an MA, and manager ranking of skill. Like the other River MAs, they were empowered in Phase 2; unlike the others, they had a high level of technical skill that gave them the ability to successfully activate different aspects of their structural position (e.g., being central in the doctor’s peer network) to influence their doctors. For example, several of these highly skilled MAs told me in Phase 2 how they had influenced doctors to implement depression screening: they had persuaded one doctor to use shared notes and then enlisted the others by telling them that they had been doing it with the first one. As one of them reported, “I usually start with [Doctor 1] first. Then I go to [Doctor 2], who is usually willing to try it. Then I’ll go to [Doctor 3] and say, ‘Hey, [Doctor 1] and [Doctor 2] are doing this and it’s working for them. Do you want me to start doing it for you, too?’”
The three reforms around which both highly skilled and less skilled River MAs successfully influenced their doctors in Phase 2 were the vaccination reform from Phase 1 and the in-visit diabetes testing and pap smear reforms. The reason that the in-visit diabetes testing and pap smear reforms now succeeded while they hadn’t in Phase 1 was because the MAs were now empowered and so had the willingness to implement the reforms. The huddle sheet that had been created by the care teams in Phase 1 enabled the MAs to use their central position in the doctors’ daily workflow to minimize the threat that the vaccination, in-visit diabetes testing, and pap smear reforms would have otherwise posed to the doctors’ specialized expertise. Doctors supported these three reforms because they could choose to approve their implementation for each patient (or not) in the pre-session huddle.
Doubling down on engagement, improvisation, and mobilization at Harbor
Like at River, when direct managerial influence failed at Harbor at the end of Phase 1, it was a director’s prior work experience that led her to contact someone she thought could be helpful to the reform effort. At Harbor, it was the medical director who reached out to an expert from the granting agency who had a reputation for having extensive knowledge about engaging doctors in changes to their practices. The Harbor medical director told me how her past work experience had led her to see doctor engagement as a good solution for problems associated with changing professional practice. She had previously been involved in a major care-management initiative that required nurse care managers to monitor and respond to the health needs of the sickest patients through home visits, office appointments, and phone calls. As she explained, “We got great help from [experts funding that program and managers implementing the program in other hospitals] around how to increase doctor engagement. . . . They told us how to get the doctors involved in developing new workflows.” This experience informed her decision to connect with the expert from the granting agency and ask her about engaging doctors in changes to their practices. The expert told her that some other sites had successfully used pre-session huddles around reforms such as vaccinations and pap smears to engage their doctors in change. The Harbor doctors were supportive of the vaccination, pap smear, and in-visit diabetes testing reforms as long as they could approve their implementation for each patient (or not) in a pre-session huddle. Thus the Harbor managers did successfully engage the doctors to try pre-session huddles, but the MAs resisted, and without the MAs doing pre-visit work to identify patients’ needs, the use of huddles fizzled because the doctors felt they were not benefitting from them.
There was a similar proportion of highly skilled versus less skilled MAs at Harbor as at River. But Harbor managers had not empowered the MAs, so the Harbor MAs were not willing to implement the reforms. As they had done in Phase 1 at both River and Harbor, in Phase 2, Harbor MAs filed into staff meetings without speaking and rarely asked questions or made comments in response to managerial announcements. The Harbor managers were frustrated that they could not get the doctors to huddle, but they misdiagnosed the key problem as lack of doctor motivation rather than as lack of MA empowerment. With the new focus on vaccinations and pap smears, the doctors and MAs also stopped focusing on implementing the in-visit diabetes testing process that they had initially implemented in Phase 1.
Phase 3: Positional Tools at River and Social Accountability at Harbor
Positional tools at River
Although River was more successful than Harbor in Phase 2 in influencing doctors to change their practices, River’s managers became frustrated that they hadn’t influenced more doctors. The operations director suggested contacting Lakeview managers directly for detailed information about using MAs to help influence doctors around PCMH. The other managers agreed. The River managers called the medical director and operations director at one of the Lakeview sites, and this phone call sparked the beginning of Phase 3 of change at River (7/2014–12/2014). I sat in on the phone call. The Lakeview medical director explained that each site had an MA representative on a centralized MA council, where they learned about new processes that they then took back to the MAs at their sites. From my field notes:
For anything new they want the MAs to do, [headquarters managers] discuss it with the MAs on the council. [Quality managers] build protocols and [HQ managers] present them to the MAs on the council. Those MAs are in charge of taking the protocols and rolling them out to MAs in their office.
The more concrete the better. . . . [The quality managers] do a lot of scripting and a lot of developing new forms. Some things they build into the [electronic medical record]. . . . They create a video so the MAs can see how to do it.
After this phone call, the River managers discussed the idea of providing more concrete resources to the MAs to help them influence their doctors.
We should take our best MA [for each reform] and say, “Here’s a specific example of what is done right.”
It sounds like we need to develop some scripting and some new materials.
Once we do that, we can give them to the MAs at the MA meeting.
In staff meetings, managers began to give MAs what I call positional tools—a subset of organizational tools that leverage subordinates’ favorable position vis-à-vis professionals to alter professionals’ perceptions of the threats that change poses to them— around each reform to strategically shape the interactions of the MAs and doctors. Each positional tool helped the MAs use their structural position to minimize the degree to which the reforms threatened the doctors’ specialized expertise, autonomy, individual responsibility for patients, or engagement in complex work.
River’s managers did not adopt Lakeview’s full set of practices around PCMH reform. Lakeview’s full process was quite different from the one River developed, as River’s managers selectively attended to only the subset of practices that related to activating the MAs to change doctors’ practices, because the River operations director had been successful using a similar solution in her prior work experience.
Workflow centrality
Some of the positional tools that the River managers provided to the MAs, such as information sheets and visual cues, enabled the MAs to use their central position in the doctors’ daily workflow to minimize the threat the reforms posed to the doctors’ specialized expertise. For example, the mammography and colonoscopy reform required that doctors use evidence-based guidelines to identify patients due for mammograms and colonoscopies and that they schedule these screening tests before the patient left the office. In response to MAs’ attempts in Phase 2, doctors had resisted changing their practices because they were concerned that, while the EMR quite accurately highlighted which patients were due for vaccinations, pap smears, and in-visit diabetes testing, it did not as accurately highlight which patients were due for colonoscopies and mammograms—notes on patients having declined the tests and on possible exceptions were captured in free text fields that were not used by the expert software in the EMR. Thus in Phase 2, only the highly skilled MAs had been able to persuade their doctors to change because their doctors perceived that these MAs had the skills to properly identify the patients due for testing.
In Phase 3, the River managers provided all MAs with information sheets on colonoscopies and mammograms that explained common reasons why a patient would not truly be due for a colonoscopy or mammogram despite being flagged by the EMR expert software (e.g., patients above a particular age would not receive a colonoscopy). Using the combination of expert software, the information sheet, and the huddle sheet minimized the threat that the reform posed to the doctors’ expertise. One doctor noted, “It’s not straightforward to see which patients need which tests. The MA marks it on the schedule based on what the system suggests and what the [information sheet advises], and I review it in the huddle.”
The introduction of a second positional tool further explains why MAs were able to successfully influence their doctors to implement the colonoscopy and mammography reform in Phase 3. Historically, the MAs had given their doctors a “patient packet” for each patient visit. Doctors had used a purple checkout form, including a list of potential future visits or tests for the patient, to indicate to the secretaries what type of visit the next appointment should be. In a weekly manager meeting in Phase 3, a manager suggested an additional use for the form: “The MAs are telling doctors at the huddle who needs colonoscopies or mammograms, but that’s not translating into these being scheduled before the patient leaves the office. . . . Maybe we could start having MAs use the purple sheet to mark required colonoscopies or mammograms. That would be a direct reminder to the doctors [at the time of] the visit.” The other managers agreed this would be a good idea, and one of them said she would modify the purple sheet to include a check box for the MAs to indicate whether the patient was due for a colonoscopy or mammography. In a staff meeting soon after, one of the managers handed out the modified purple sheet to the MAs. “You can use this to remind the doctor that this patient is overdue for [colon- or breast-cancer] screening. It’s helpful for them to have the extra reminder. Then, if the doctor is willing, they order it.” The visual cue of the purple sheet helped MAs define the situation as one in which the doctor was getting a helpful reminder from the MA rather than as one in which managers were asking doctors to take on the routine work of ordering screening tests before the patient left the office. “The purple sheet is helpful,” one doctor told me. “I like to think that once I look at anything, it’s already in my head. But there is so much going on [at the time of the visit] that it’s good to be reminded.”
Task criticality
Other positional tools that the River managers gave to the MAs—what I call favor scripts and favor tools—were effective because the doctors depended on the MAs for critical tasks, so they were open to doing favors for the MAs. The favor scripts and favor tools minimized the threat the reforms posed to the doctors’ autonomy because they led the doctors to see themselves as implementing the new practices to help their MAs rather than to meet managerial demands. In one meeting, the managers discussed the idea of giving the MAs a script to help them persuade their doctors to implement the PopulationCare reform for diabetic patients. A manager said, “One of the things that has been powerful for doctors to change the ways they do things is to show how it helps their staff. The docs think, ‘If there’s something that will allow my MA to work better and it’s a small change for me to make, I’ll do it.’ That works with the docs. . . . We should make sure the MAs know that.” Soon after, I saw the managers give the MAs a favor script. “For doctors who aren’t doing PopulationCare,” a manager told the MAs, “you could couch it as ‘It’s very helpful for me,’ rather than ‘This is the policy’ or ‘We need to do it.’”
In Phase 2, before the managers had provided this favor script, the doctors had resisted MAs’ visual cues around PopulationCare because this reform challenged doctors’ autonomy. One MA recalled explaining to her doctor that she would use the PopulationCare system to help identify the testing that patients needed: “I go as far as highlighting [patients who need to be screened], and I put in the form [to get a screening test ordered for the patient], but then it comes back [from the doctor] with [no orders] signed off on.” But in Phase 3, the experience was different. As one MA explained, “I told [doctor] that when patients are on the list, I need to keep managing them, and that takes time. Finally, she said she would do the [lipid panel checks] to get those patients off the list for me.”
In these interactions, the MAs were clearly subordinate to the doctors; the doctors did not perceive the MAs’ requests for favors as challenging their autonomy as the managers’ direct requests had. The doctors felt an obligation to help the MAs because the MAs were so helpful to them. One doctor offered this example: The guidelines built into PopulationCare require that [diabetic] patients with high LDLs need to be checked every year, regardless of medication. If we don’t check the level every year, those patients will keep showing up on [MA’s] list. And [MA] needs to deal with the patients. So, fine, I’ll check it every year.
Doctors expressed that they were willing to have their MAs remind them to check cholesterol levels every year to help the MAs as long as these decisions did not run counter to their clinical judgment.
In Phase 3, in addition to equipping MAs with a favor script, the River managers gave them a favor tool. I observed the managers talk about this in one of their meetings:
We need to find a way to keep review of the PopulationCare lists on people’s radar screen. It seems to drop off and people forget about it. What do you think of some kind of PopulationCare tracking tool? . . . I’m thinking of it as just a way to prompt people, to remind them and nudge them. We could post it in a central place in the pod, and MAs could mark off when they’ve had the conversations with their doctors.
This would help the MAs be able to come up and say, “We haven’t touched base yet this month, and it’s week two.” A lot of [doctors] won’t want to do it, but their MAs will get them to.
Soon after, the managers gave the MAs the tool:
There needs to be a time for you to touch base with your doctors on PopulationCare. It would be good to track this to remind the doctors to do it. This tracking tool is a reminder.
Make sure the doctors hear about it, too.
The way I’ll phrase it to them is that we’ve been working on setting clear expectations about what the MAs need to be doing regarding the PopulationCare list. I’ll tell them that this will serve as a reminder for everyone to touch base.
Before the MAs had use of this favor tool, they had reported feeling frustrated about trying to get their doctors to do PopulationCare. “I spend a lot of time working on his lists [to highlight which patients are overdue for testing],” one MA had said, “and he won’t [order the tests]. It’s a lot of work for us to do and bring it to the doctor and they say, ‘Whatever.’” The favor tool allowed the MAs to reinforce that the doctor would be doing this for the MA, to help her do her job. One MA related, “I bring it up with him, and he may decide to do something about it with that patient or not. . . . The [favor tool] shows that it’s only once every two weeks. I’m not going to be asking him every day . . . it shows that this is something that I have to do, that this is part of my job. I can’t do my job unless he meets with me about the list.”
Referring to their suggestions as requests for favors enabled the MAs to minimize the threat to doctors’ autonomy. The doctors were not complying with a managerial requirement but doing a favor for their valued MA. As one doctor put it to me, “We want to keep the MAs happy because we depend on them. Like, with PopulationCare, [the MAs] want us to talk about it with them twice a month. . . . Because I know that, I do it, even though it is kind of a pain. I like to keep them happy.”
Peer network centrality
One tactic that MAs said worked well when they were trying to get their doctors to try a reform for the first time was an MA-led pilot with one of the doctors on the team. Each MA worked for several doctors on the team, and so the MA was central in the doctors’ peer network. River managers began to suggest to the MAs that they should pilot new processes with a single doctor on their team before approaching the other doctors. The MAs could then use a peer doctor who had converted to PCMH to persuade other doctors that the reform did not require them to go against their need to take individual responsibility for patients.
In Phase 2, before the managers had enlisted the MAs each to persuade an initial convert, I had observed several MAs attempt to influence their doctors to do depression screening using shared notes. Each had failed. In Phase 3, however, they began to succeed. One MA told me how using an initial convert had helped her to convince one of her doctors to do it: After the huddle, I said to [Doctor 4]: “Okay, today we’re going to start something new—shared notes.” I gave her the sheet of instructions explaining how the shared-notes process works. “This explains it all right here. I’ve been doing it with [Doctor 5], and he likes it.” [Doctor 4] said, “You’ve been doing it with [Doctor 5]?” I said, “Yes, and it’s working well. Here’s how it works.” Then I showed her on my computer how I did it. I told her, “I go into the vitals section and put in the vitals, and then I send the note to you. I’ll also put in the scores for the [brief screening test]. You pick it up and work in it just like you always do.” I said, “How about we start with two of your patients today and see how it goes?” She agreed.
By using initial converts to change doctors’ perceptions about shared notes—from an unprofessional delegation of tasks to others to engagement in a new practice approved by peers—MAs again minimized a threat to doctors. One doctor said, “[MA] told me she was doing it with [doctor] and he said he really liked it. So I said, ‘Fine, let’s try it.’”
In a less explicit way, in Phase 3 the River managers also discussed the idea of using surprise converts to help MAs persuade their doctors to implement depression screening using shared notes. Some doctors were not persuaded by the use of reform practices by doctors whom they perceived to be very open to new innovations, but when a doctor they perceived to be impervious to change adopted a reform, they took note. Managers understood the value of a surprise convert. In one meeting I listened to a manager reflect: “Actually, he’s someone—if you could get him on board, that would really send a signal.” Soon afterward, a manager asked an MA to relate to others how she had influenced a doctor who had been adamantly against shared notes to start using them. The MA said she knew [Doctor 6] would be surprised to hear that [Doctor 8] had started the practice, so she approached [Doctor 6] only after she had persuaded [Doctor 8] and used the fact of that conversion as bait. The surprise converts enabled MAs to better influence their doctors to change. One morning, as I was shadowing a doctor, she recalled how her MA had persuaded her to use shared notes: I didn’t want to do it because I prep my notes ahead of time, so I would have to save my note as a different user. I had an anxiety attack. . . . [MA] said, “[Doctor 7] does it.” I said, “Yeah, but [Doctor 7] does everything.” Then she said, “[Doctor 8] is doing it.” I said, “No way! [Doctor 8] is doing it? Get out!” So then, of course, I had to do it. . . . So, there is the competitiveness and also healthy joking.
In between doctor and patient
River managers also gave MAs legitimacy scripts and legitimacy tools that allowed MAs to shape patients’ perceptions of the reforms. This, in turn, protected their doctors’ ability to engage in complex medical work rather than in what they saw as disruptive emotional work. These materials were effective, in part, because the MAs were positioned between the patients and the doctors; they could help to shield the doctors from the emotional challenges of upset or angry patients. For example, one PCMH reform was to get patients who were prescribed narcotics to sign opioid agreements and to engage in quarterly drug testing to monitor the use and abuse of opioids by patients and to prevent the diversion of opioids to people who were not patients. Several MAs had reported in Phase 2 that they had tried to point out in huddles the patients who needed opioid agreements, but their doctors were concerned that asking their patients to sign these agreements would make them upset or angry. Trying to implement this reform could derail patient visits into long discussions of routine matters unrelated to the delivery of complex patient care. In a manager meeting in Phase 3, one manager remarked, “One thing [MA] does differently is that she’s got a way of prepping people for the conversation. I think [MA] has a nice script, and that’s not the case across all of the teams. It would be nice to get some good lines together for all of the MAs.” Soon after, I saw the managers encourage the MAs to use such a script with patients. In one meeting a manager asked the MA she had referred to in the manager’s meeting to tell the other MAs about the script she used. From my fieldnotes:
This is a new law and all patients on opioids will need to do this. [MA], you’ve been trying it on your team. How do you bring it up with patients?
I tell them that it is a new law and your doctor will be reviewing this [opioid agreement] with you. I give them a heads up, what [the agreement] looks like, and what the doctor will talk to them about. . . . I bring it up in the huddle with the doctor and the doctor may say, “This patient will have a hard time.” Then I know to do a little more explaining about the new law.
In a different meeting, the managers gave MAs scripted language to handle interactions with patients on opioids.
Will we get resistance from the patients?
These may not be easy conversations. . . . Language choice is important. We should move away from using the terms “substance abuse” or “narcotics” [when talking to patients]. Instead, we should say “opioids.”
In addition to giving the MAs scripts, the managers gave them an information sheet on the opioid policy that they could pass to patients “so they won’t feel picked on.” The information sheet conveyed the legitimacy of the reform by showing that all patients on opioids were being asked to sign this agreement as part of nationwide regulations. The sheet read: Opioid pain relievers are related to addictive drugs like opium, morphine, and heroin. The use of opioid pain medication is tightly controlled and monitored by the federal government through the Drug Enforcement Agency (DEA). . . . Guidelines and policies such as this one limit unnecessary prescription and misuse of opioid pain medications. . . . For our patients’ wellbeing and because of ever-tightening regulations and oversight, River has adopted the following policy for the treatment of post-operative or post-injury pain management. . . .
The legitimacy script and information sheet helped MAs minimize the threat the reform posed to the doctors’ ability to engage in complex work. The doctors saw that patients were less likely to become upset or angry and more likely to be accepting of the new law. One doctor said to me, “[MA] giving them the information first makes the whole conversation go a lot more smoothly.”
The positional tools that River’s managers gave to MAs in Phase 3 helped them to change their doctors’ perceptions of the threats that the reforms posed to them. Change was very successful: the average monthly reform usage rate rose to 65 percent. Table 3 shows the dramatic increase in use of various positional tools at River in Phase 3, in contrast to their very limited use at Harbor through all three phases.
MAs’ Regular Use of Positional Tools with Doctors in Each Phase*
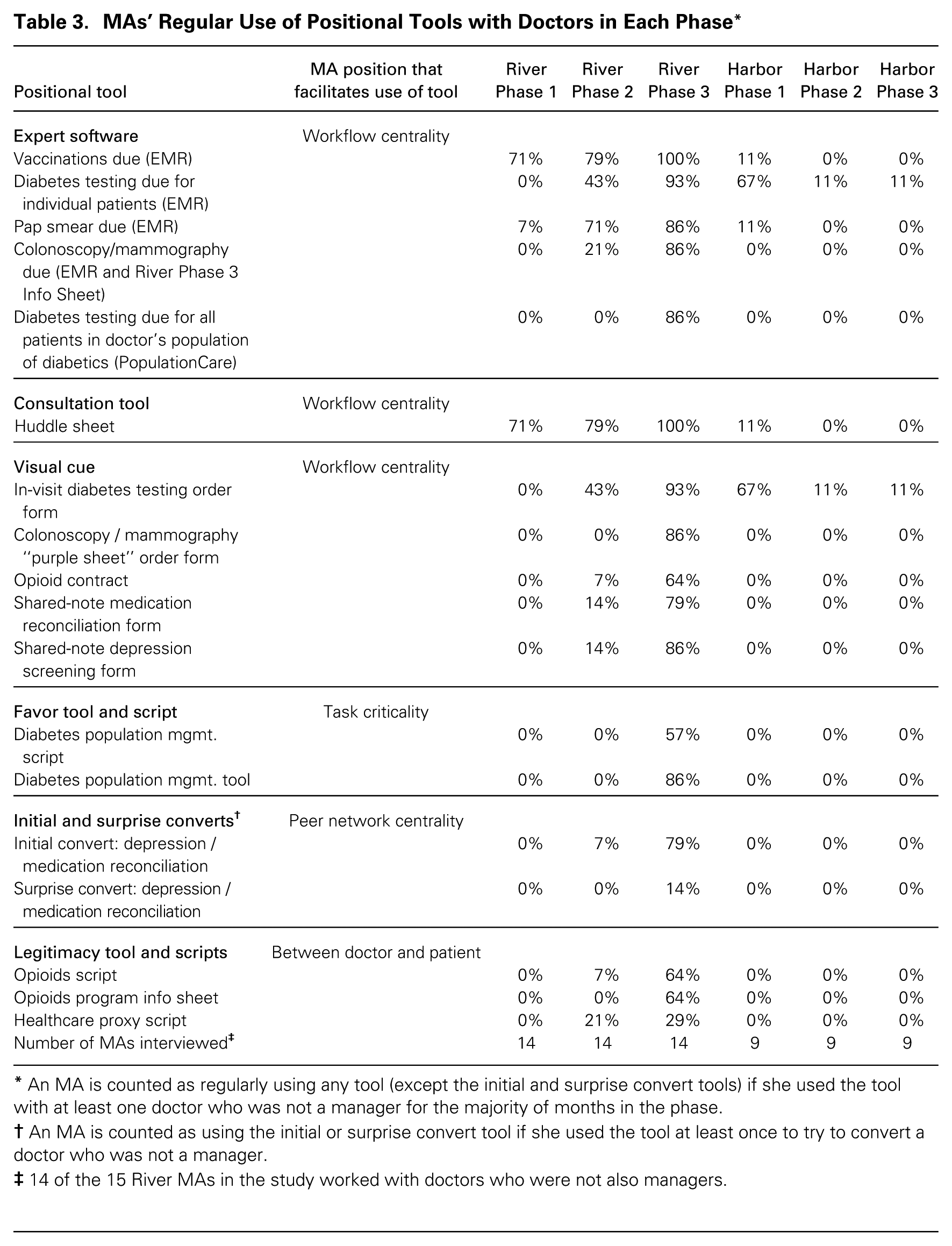
An MA is counted as regularly using any tool (except the initial and surprise convert tools) if she used the tool with at least one doctor who was not a manager for the majority of months in the phase.
An MA is counted as using the initial or surprise convert tool if she used the tool at least once to try to convert a doctor who was not a manager.
14 of the 15 River MAs in the study worked with doctors who were not also managers.
Failure of direct tactics at Harbor
While managers at River gained significant traction in the change effort in Phase 3, at Harbor, they did not. In this phase, the Harbor medical director’s prior work experience led her once again to seek solutions focused on doctor engagement. This time, the medical director connected with a manager in a primary care department at Mountainside Medical Center (a pseudonym) and, as in Phase 2, she discussed the advice she received with the other managers. They tried three new ways to better engage the doctors in change.
First, Harbor managers tried to increase doctors’ attendance at the biweekly care team meetings by announcing, before meetings, formal policies they planned to discuss around which they knew doctors would want to provide input. Second, managers circulated testimonials from doctors and MAs on the transformation team about the benefits to care team members of engaging in pre-session huddles. And third, the managers tried to increase social accountability. In one meeting, the medical director said to the other managers, “How can we make [huddles] more effective for the docs? I’m not giving up on this. I talked to people at Mountainside. They were having trouble making doctors have huddles happen. . . . One of the things that has worked well there is to track that the huddles are happening. We can start measuring it.”
Managers made up tracking sheets that allowed the tracking, for each doctor for each week, of whether or not the doctor had had a pre-session huddle with the MA. In an effort to avoid a command-and-control approach that doctors might see as limiting their discretion, managers did not strictly define what counted as a huddle. The MAs checked off each time they huddled with a doctor, and the managers collected the sheets and began to report to the teams what their huddle rate was. But with the new focus on huddle outcomes without a strict definition of huddles, MAs began to count any communication with doctors about patients during the day as a huddle rather than counting only pre-session communication with a doctor as a huddle. Pre-session communication was required for the implementation of the vaccination and pap smear reforms, because it allowed doctors to approve (or not) their use for each patient. Despite the large number of huddles reported on the tracking sheets during this time, in my shadowing of doctors and MAs in clinic, I did not observe pre-session huddles regularly occurring, and doctors and MAs both reported privately to me that they were not checking in with one another before each session to discuss which patients needed vaccinations and pap smears. In Phase 3, Harbor managers continued to fail to influence the doctors to change their practices: doctors’ monthly usage rate across the same reforms that River attempted was 1 percent.
My inductive study indicates that the difference in managers’ use of subordinate activation tactics is what led to the different outcomes at River and Harbor. Table 4 shows these differences by demonstrating that managers at each facility used direct tactics such as engagement and improvisation at similar rates to try to get doctors to implement changes, because the grant that both River and Harbor received stipulated that they hold biweekly care team meetings, in which the managers used engagement, improvisation, and social accountability tactics, and transformation team meetings, in which managers used mobilization tactics. But managers at River—and not at Harbor—also encouraged change in doctors’ practices by empowering the MAs and giving them appropriate positional tools to use in that effort. There are several other potential alternative explanations for the successful micro-level institutional change I observed at River, which I address in the Online Appendix (http://journals.sagepub.com/doi/suppl/10.1177/10.1177/0001839218804527).
Managers’ Attempts to Change Professional Practices at River and Harbor*
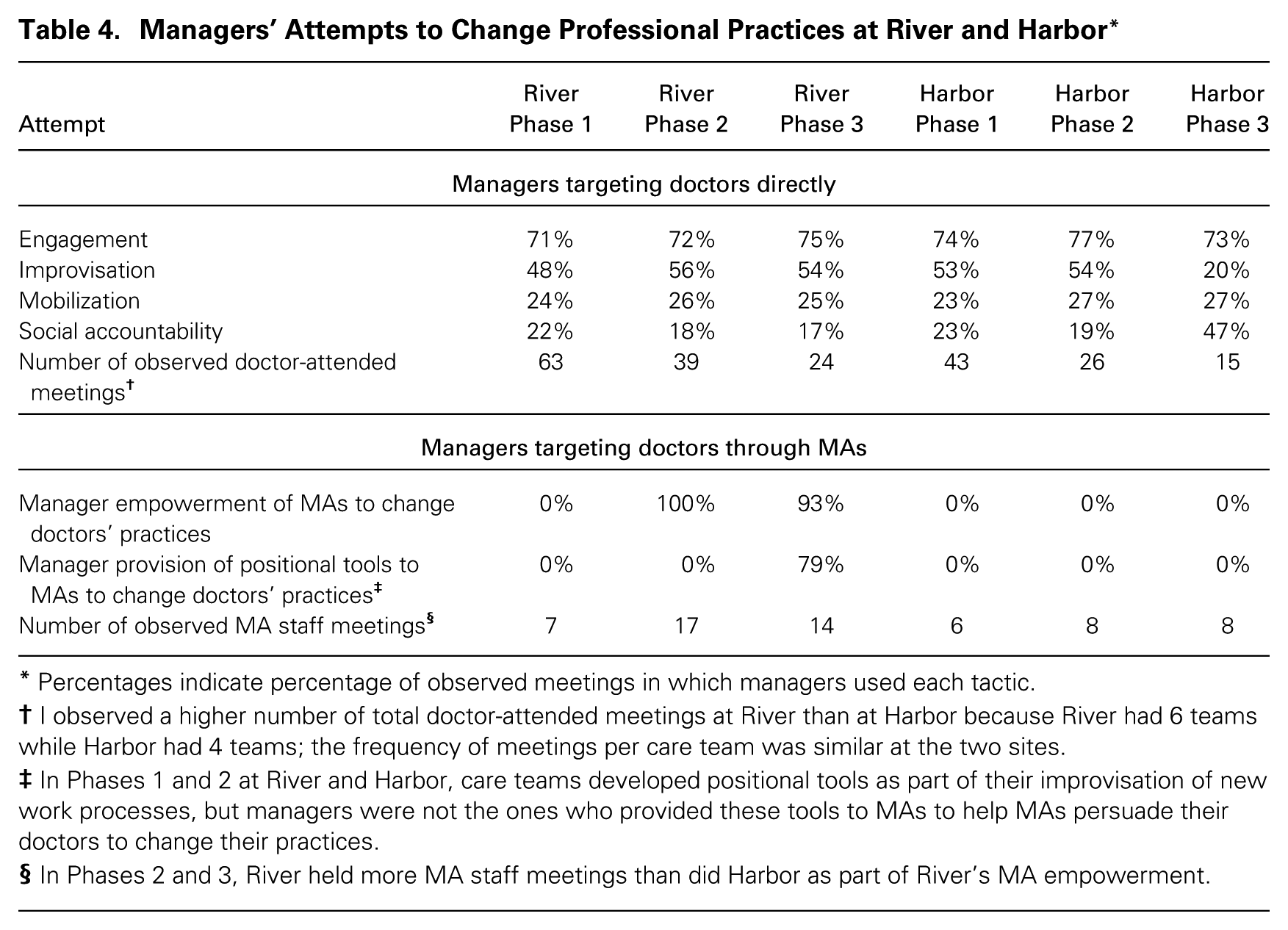
Percentages indicate percentage of observed meetings in which managers used each tactic.
I observed a higher number of total doctor-attended meetings at River than at Harbor because River had 6 teams while Harbor had 4 teams; the frequency of meetings per care team was similar at the two sites.
In Phases 1 and 2 at River and Harbor, care teams developed positional tools as part of their improvisation of new work processes, but managers were not the ones who provided these tools to MAs to help MAs persuade their doctors to change their practices.
In Phases 2 and 3, River held more MA staff meetings than did Harbor as part of River’s MA empowerment.
Discussion
A Model of Subordinate Activation Tactics
This paper details how subordinate activation tactics can be used for successful micro-level institutional change in seemingly intractable contexts. Figure 1 shows how these came into play during the professional practice change effort I studied. Such tactics entail managers drawing on the favorable structural position of subordinate semi-professionals vis-à-vis superordinate professionals to indirectly change professional practice. As the ranks of subordinate semi-professionals continue to expand, subordinate activation tactics represent an important new set of tactics for micro-level institutional change. They work because subordinate semi-professionals, despite having no formal authority over professionals, have a high capacity for influence derived from their favorable structural position. When they occupy a central position in the professionals’ workflow, they can control professionals’ access to information about new practices and can offer professionals opportunities for consultation about these practices before implementation. When they perform tasks that are critical to professionals’ daily work, they can ask for favors of them. When they occupy a central position in the professionals’ peer network, they can convert one or two professionals and then tell the others about the new practices peers are using. And when they are positioned between the client and the professional, they can suggest changes in professional practice while also shielding professionals from the emotional challenges of upset or angry clients.
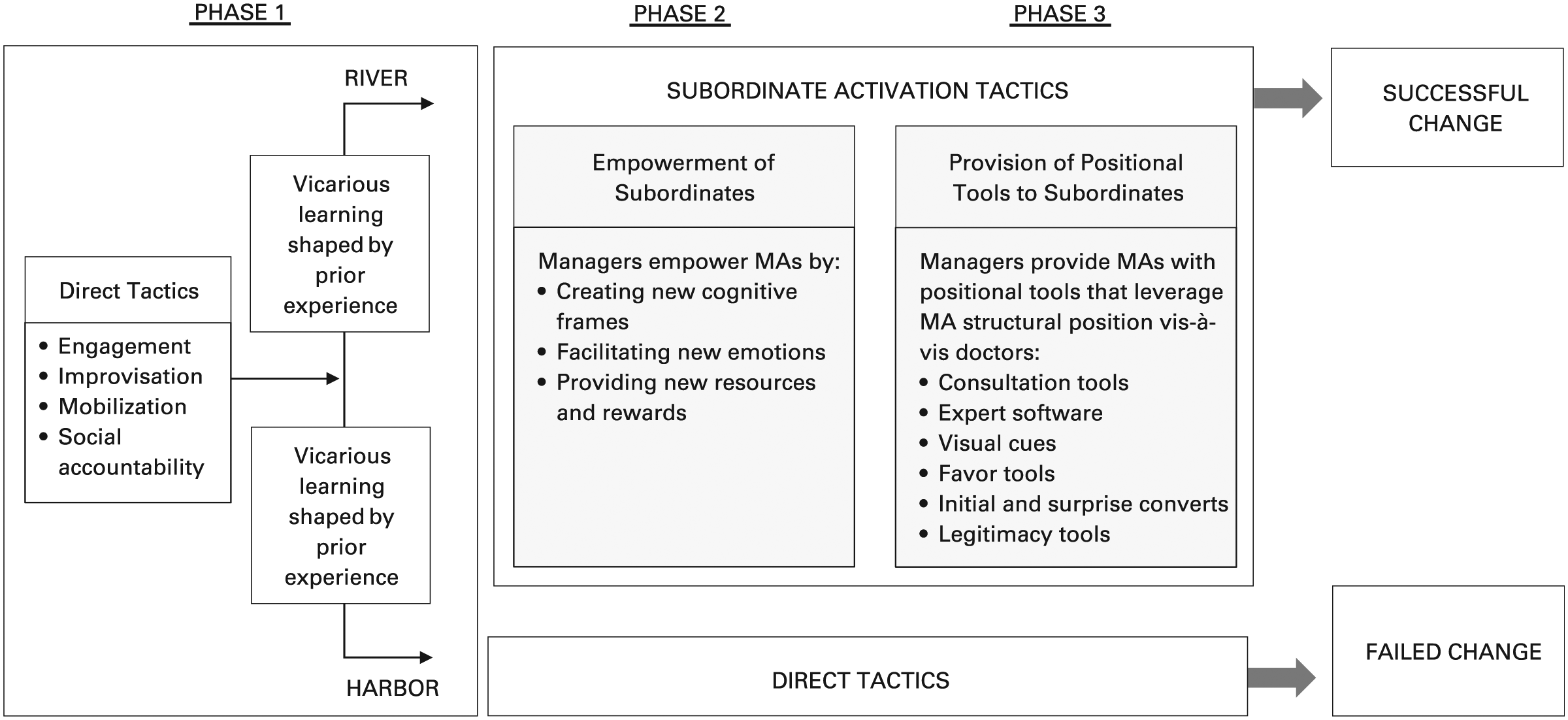
Subordinate activation tactics and micro-level institutional change at River but not Harbor.
Managers can activate the favorable structural position of subordinate semi-professionals by first empowering subordinates and then giving them positional tools to intervene in the work processes of the professionals with whom they work. By empowering subordinates, managers can give them the willingness to activate their favorable structural position to change professionals’ practices. Managers can accomplish broader micro-level institutional change by also providing them with positional tools that leverage their favorable position vis-à-vis professionals to reduce the threats that change poses to the professionals. The positional tools can increase subordinate semi-professionals’ ability to accomplish change by helping to minimize challenges to professionals’ institutions—their specialized expertise, autonomy, individual responsibility for clients, and engagement in complex work. By empowering subordinate semi-professionals and giving them positional tools, managers can enlist them to use their favorable structural position to accomplish change on the managers’ behalf as outlined in figure 1.
Conceptualizing Positional Tools
The concept of positional tools adds to our understanding of tools that can facilitate change in professional organizations. Scholars of cross-occupational collaboration and reform implementation have highlighted the importance of providing organizational tools for change. Scholars of cross-occupational collaboration have shown that collaboration tools such as rules and routines, boundary objects, and common spaces can improve collaboration by bringing occupational groups together and specifying responsibility for tasks (e.g., Kellogg, Orlikowski, and Yates, 2006) or by supporting the translation of meanings and the negotiation of status across occupational boundaries (e.g., Bechky, 2003). And Dobbin and his colleagues have shown that top managers are often willing to adopt bureaucratic solutions that apply consistent and complete rules across situations to reduce risks in their organizations, because these solutions run smoothly and have predictable costs (Dobbin and Kelly, 2007; Dobbin, 2009).
Positional tools are a subset of collaboration tools and bureaucratic solutions that leverage subordinates’ favorable position vis-à-vis professionals to reduce the threats that micro-level institutional change poses to professionals’ specialized expertise, autonomy, individual responsibility for clients, and engagement in complex work. As summarized in figure 2, there are many types of positional tools. Consultation tools supported by expert software leverage subordinates’ position in the daily workflow to allow professionals to review and approve subordinates’ proposed changes in daily work. Visual cues leverage subordinates’ position in the daily workflow to attract the attention of professionals who face many concurrent demands in their daily work. Favor tools leverage professionals’ dependence on subordinates for critical tasks to minimize threats to professionals’ autonomy. Initial and surprise converts leverage subordinates’ central position in professionals’ peer networks to reduce challenges to professionals’ identity. And legitimacy tools leverage subordinates’ position between professionals and their clients to help reduce challenges to professionals’ engagement in complex work. This paper demonstrates that when subordinate semi-professionals are central in professionals’ daily workflows, critical to their daily work, central in their peer networks, or positioned between professionals and their clients, managers can give subordinates positional tools that help them leverage these favorable structural positions to change professional practice. Positional tools represent a previously unidentified yet powerful set of tools for micro-level institutional change that can be highly effective in seemingly intractable circumstances.
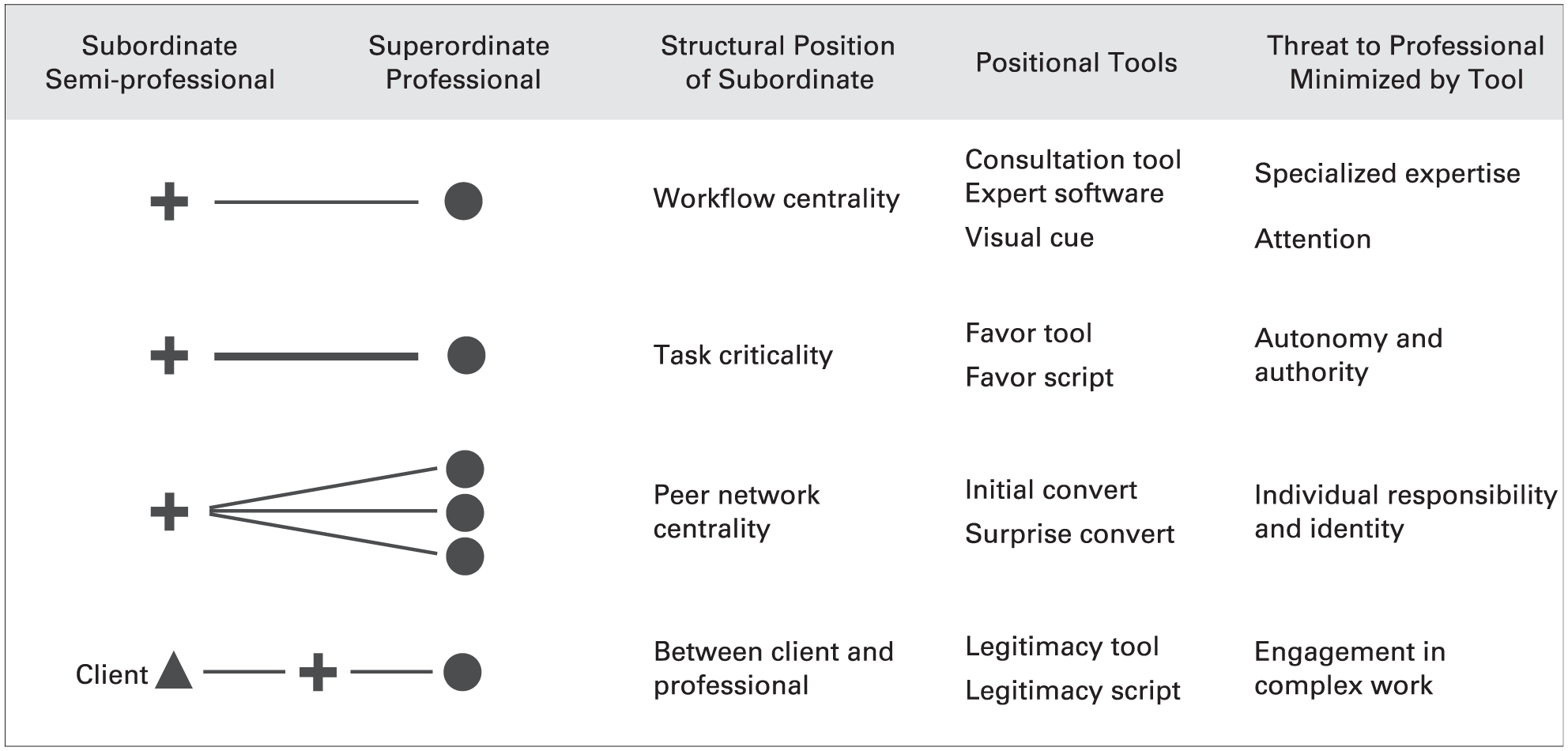
Positional tools for subordinates to use to reduce threat of change for professionals.
At first glance, subordinate activation tactics may look similar to mobilization tactics, such as the tactics used by surgical trainees in the relational spaces described by Kellogg (2009, 2011a), but subordinate activation is different from mobilization in two ways. First, subordinate activation allows managers to enlist third-party actors who have no initial interest in changing professionals’ work practices but who occupy a favorable structural position vis-à-vis the professionals, rather than entailing self-mobilization by subordinate and superordinate professionals who are interested in changing work practices. Second, subordinate activation requires managers to provide these third-party actors with positional tools to influence the professionals to change, rather than subordinate and superordinate professionals using their own resources to accomplish change. The differences between the findings presented here and the findings in studies of mobilization suggest that when subordinates have no initial interest in changing professionals’ work practices but occupy a favorable structural position vis-à-vis professionals—and when there is a large status difference between subordinates and professionals—managers can accomplish broad change by both empowering subordinates and offering them positional tools. The findings have several implications for our understanding of micro-level institutional change tactics.
Contributions to Our Understanding of Micro-level Institutional Change Tactics
As noted earlier, seven tactics have been shown to be effective for accomplishing micro-level institutional change: engagement, improvisation, mobilization, social accountability, legitimation, transparency, and contact with groups who will benefit from the change. In the study presented here, managers used four of these seven tactics—engagement, improvisation, mobilization, and social accountability—yet failed to change professional practice. None of the managers at either site tried to use the other three tactics: legitimation, transparency, and contact with groups who will benefit from the change. My findings highlight the conditions that may explain the failure of the first four tactics, as well as some reasons why managers may be unwilling to use the other three tactics.
Regarding engagement, scholars have shown that managers can persuade professionals to change their practices by engaging them in promoting reform; engagement can be effective because when individuals engage in reform and their beliefs do not match their behaviors, they experience cognitive dissonance and have a strong tendency to address it by changing their beliefs (Perlow, 2012; Dobbin, Schrage, and Kalev, 2015). Both River and Harbor tried to engage doctors in the development of new work processes related to PCMH, but engagement ultimately failed.
Engagement initially succeeded as doctors at both River and Harbor worked with their care teams to develop a new process related to the PCMH reforms. But engagement failed to accomplish widespread change because when managers tried to engage the doctors in developing a second process around managing high-risk patients, doctors resisted. They were being asked by multiple different groups to introduce reforms and to do so within their brief doctor–patient visits. They felt that creating and implementing a second new process would prevent them from engaging in the complex work they needed to do with patients during the visits. This finding suggests that engagement may fail in contexts in which professionals are already responding to multiple external demands or there is little slack in the system to allow them time to fulfill their regular professional responsibilities in addition to participating in change programs.
Regarding improvisation, prior research has shown that managers can encourage professionals to change their practices by improvising new practices in day-to-day work in response to everyday contingencies, breakdowns, exceptions, and opportunities (e.g., Orlikowski, 1996; Reay, Golden-Biddle, and Germann, 2006; Smets and Jarzabkowski, 2013) and by codifying them into best-practice guidelines and targeting them toward a narrow network of peer professionals concerned with pragmatically solving specific problems (e.g., Smets, Morris, and Greenwood, 2012; Valentine, 2018). Both River and Harbor tried to improvise new work processes related to PCMH, as required by the grant, but improvisation ultimately failed.
Unlike in the contexts previously studied, such as the law firm Smets, Morris, and Greenwood (2012) studied, in my setting change was not urgent, nor were the financial or reputational costs high for professionals not changing. In addition, the proposed change challenged doctors’ specialized expertise, autonomy, ability to take individual responsibility for clients, and engagement in complex work. Doctors resisted implementing the new practices because they did not see them as pragmatically efficient. This finding suggests that improvisation tactics, while useful in some contexts, may fail when pressures on professionals to change their practices are weak or when the proposed change challenges multiple dimensions of professionals’ institutions.
Regarding mobilization, Kellogg (2009, 2011a) has shown that subordinate and superordinate reformer professionals can mobilize with one another in relational spaces to challenge defender professionals to change their practices. Yet, as required by the grant, both River and Harbor had relational spaces available to them in the form of transformation team meetings in which managers gathered reformer doctors and staff members together to meet apart from doctors and staff members who did not support the changes, apart from the work itself, and with other reformers from each of the different work positions involved in the practices targeted for change. Kellogg’s prior research suggests that the relational spaces should have helped these reformers develop a new sense of efficacy, new frames, and new identities to allow them to challenge defenders of the status quo outside of the relational spaces. But they did not.
Mobilization using relational spaces failed at River and Harbor because managers drew reformer doctors, nurses, MAs, and secretaries on the transformation team from across their large departments, and these reformers did not work together on the same care teams. To implement new processes, these reformers depended on the work of others on their local care teams who were not on the transformation team and so not mobilized, and these others resisted change. This suggests that relational spaces may fail even if they include reformers from all of the different work positions involved in the practice targeted for change if reformers are not from intact teams that can mobilize with one another in their everyday work to change practices.
Regarding social accountability, we know from past research that managers can increase it by introducing new monitoring and measurement systems (e.g., Kalev, Dobbin, and Kelly, 2006; Kalev, 2014) or by making professionals’ practices known to all (Sauder and Lancaster, 2006; Castilla, 2015). At both River and Harbor throughout the course of the study, managers tried to measure and report reform outcomes, but this tactic failed for several reasons. First, because the River and Harbor IT systems did not capture data that could be used to measure the degree to which daily work processes (rather than outcomes) changed, managers needed to rely on more labor-intensive means of measurement such as counting by hand the number of vaccines that had been delivered to patients before their doctor visits. For this reason, managers did not track and report results about the implementation of all the reforms on a regular basis. In addition, in Phase 3, Harbor tried to increase social accountability by tracking the implementation of huddles around vaccinations, pap smears, and in-visit diabetes testing on a regular basis; however, managers did not announce what indicators they used to measure the outcome they were trying to accomplish (pre-session huddles) because they were concerned that professionals would see this as a threat to their autonomy. Without specifying indicators, the measures became meaningless. These findings suggest that social accountability tactics may be less effective in contexts in which the outcomes of interest are work processes rather than outcomes and are difficult to track. The findings also serve as a warning to managers that without specific indicators for desired outcomes, social accountability is unlikely to be effective.
The three tactics that the literature shows to be effective that River and Harbor managers did not use are legitimation, transparency, and contact with groups who will benefit from the change. Regarding legitimation, managers at both sites did attempt to use this tactic, but not in the way the literature would recommend. We know from past research that legitimation is most effective when frames resonate with the beliefs of targeted professionals (e.g., Greenwood, Suddaby, and Hinings, 2002; Zilber, 2002; Lawrence, Malhotra, and Morris, 2012). Managers at both River and Harbor did use one frame—”PCMH reforms will benefit patients”—that resonated with doctors, but managers used other frames, such as the need for standardization and for taking collective responsibility for patients, that did not resonate with most doctors. Managers did not attempt to marshal specific evidence for the efficacy of the PCMH reforms, even though past research has shown that evidence of efficacy resonates with the beliefs of targeted professionals and so can increase professionals’ motivation to alter their work practices (Tucker, Nembhard, and Edmondson, 2007). This finding suggests that the reason managers may appear unwilling to use the tactic of legitimation is that they underestimate the importance of developing resonant frames for change.
Even though the literature has shown transparency tactics to be effective (Dobbin, Schrage, and Kalev, 2015), River and Harbor managers also didn’t use these tactics. In this setting, such tactics would have included giving the doctors transparent information that informed them about all of the opportunities for change. At both River and Harbor, managers never gave doctors clear and complete information about the full set of reforms they hoped to implement, in part because they were concerned that doctors would actively resist all PCMH reforms if they saw the full list. I have no counterfactual case in my dataset to assess whether the managers were correct in this assumption, but prior studies showing the usefulness of transparency have not examined contexts in which a large number of reforms were being introduced at the same time.
Finally, the literature suggests that contact tactics can be effective (Kalev, 2009; Briscoe and Kellogg, 2011), but River and Harbor managers did not use them. In this setting, such tactics would have entailed increasing the contact between doctors and patients, those who would benefit from change. At both River and Harbor, managers talked of bringing patients into contact with doctors outside of clinic visits by including patients on their transformation teams, but neither site did it. Managers were concerned that including patients on these teams would redirect efforts away from the particular PCMH reforms that managers were attempting to implement and toward other efforts that the patients might have wanted, such as improving the department’s website to make it easier for patients to navigate. Managers felt pressure to implement PCMH reforms and did not want to detract from these managerial imperatives.
Contributions to Our Understanding of Network Mechanisms for Change
Subordinate activation is a network mechanism for change that adds to our understanding of three other related network change mechanisms: upward influence, two-step leverage, and network activation. Scholars of upward influence have shown that subordinates often have informal influence—the ability to change the actions of others in some intended fashion despite having no formal authority to do so. Scholars have shown that when subordinates have a favorable structural position (Emerson, 1962; Pfeffer and Salancik, 1978; Fligstein, 1990), they may be able to use tactics such as consultation, rationality, inspirational appeal, ingratiation, social proof, upward appeal, assertiveness, and exchange to influence others in dyadic interactions (see Higgins, Judge, and Ferris, 2003, for a review). In professional organizations, tactics such as consultation, exchange, and social proof have been shown to be particularly effective (e.g., Battilana and Casciaro, 2013; Empson and Langley, 2015).
All prior studies of upward influence, to my knowledge, have investigated situations in which subordinate influence agents have a favorable structural position vis-à-vis superordinate targets and in which subordinates try to influence superordinates in dyadic interactions. My study adds to our understanding of upward influence by suggesting that influence agents (e.g., managers) with an unfavorable structural position vis-à-vis targets (e.g., doctors) can accomplish informal influence triadically rather than dyadically by providing members of a third-party group (e.g., MAs) who do have a favorable structural position vis-à-vis targets with both empowerment that gives third-party members the willingness to activate their structural position and positional tools that give them the ability to do so.
The concept of subordinate activation tactics also adds to our understanding of the network mechanism of two-step leverage (Gargiulo, 1993). Scholars of two-step leverage have described how the weak party in a dependence relationship (party A) may attenuate the negative effects of this dependence by enlisting the help of a third party (party C) who has power over the strong party (party B). Two-step leverage examples include the subordinate investment banker A who enlists the help of his more senior boss C to persuade another investment banker B to provide knowledge and information to the subordinate investment banker (Galunic, Ertug, and Gargiulo, 2012) or the female professional A who seeks a mentor–protégé relation with a powerful senior ally C to enhance her legitimacy with other players B above her level (Ibarra, 1997; Burt, 1998). These prior studies of two-step leverage have examined situations in which the initiating party A engages a third party C who is senior to targeted party B.
In contrast, subordinate activation tactics describe a change mechanism in which the initiating party A (e.g., manager) engages a third party C (e.g., MA) who is subordinate to rather than superordinate to targeted party B (e.g., doctor). In previously elaborated two-step leverage processes, Step 1 involves the initiating party covertly making influence requests of superordinate third-party members. With subordinate activation, since third-party members are subordinate to both the initiating party members and the targeted party members, Step 1 also involves the initiating party empowering third-party members by facilitating their development of new cognitive frames and giving them resources and rewards to act on behalf of the initiating party. Along these same lines, in previously described two-step leverage, Step 2 involves superordinate third-party members constraining targeted party members by using their superordinate position to make demands. In subordinate two-step leverage, third-party members cannot use formal position power to make demands of targeted party members but, instead, must use their informal position power. Positional tools leverage subordinates’ favorable position vis-à-vis targets to reduce the threats that change poses to the targets.
Finally, subordinate activation tactics contribute to our understanding of network activation. Network theorists have shown that even if actors have a favorable structural position, some may not be willing to activate it to accomplish goals because of individual characteristics (e.g., Sasovova et al., 2010; Srivastava and Banaji, 2011), because of situational characteristics (Srivastava, 2015a), or because being low status prompts an inhibition response—negative emotion, inhibited behavior, and attention to threat rather than rewards (Bunderson and Reagans, 2011; Menon and Smith, 2014; Srivastava, 2015b). The network activation literature also shows that, even if actors are willing to try to activate their structural position, they may not be able to do so if they do not have the cultural resources needed to shape and alter the meaning and purpose of social relations (Gulati and Srivastava, 2014; Goldberg et al., 2016; Ranganathan, 2017). Actors may also not have the ability to activate their structural position if their targets fear some kind of loss involved in helping them, such as a loss of identity or status, and so refuse to assist them (Smith, 2005; Burt and Merluzzi, 2014).
While the literature on network activation highlights how willingness and ability are necessary to activate structural position, it does not investigate how members with a favorable structural position, but without the willingness or ability to activate it, can be equipped to do so. The concept of subordinate activation demonstrates that third-party actors can increase actors’ willingness to activate their structural position by empowering them. Third-party actors can also increase low-capacity actors’ ability to activate their favorable structural positions by giving the low-capacity actors positional tools (such as consultation tools or favor tools) that allow them to leverage various aspects of their structural positions to reduce the threats that helping them poses to the targets.
Contributions to Our Understanding of Vicarious Learning
Finally, this study adds to our understanding of vicarious learning. Dobbin, Simmons, and Garrett (2007) proposed four main mechanisms for the diffusion between actors of reform policies, models, or tactics: social constructivism, coercion, competition, and vicarious learning. The vicarious learning mechanism best explains the diffusion of implementation tactics at River and Harbor because it was new evidence on the successful implementation of PCMH reforms in other medical organizations that led River and Harbor managers to change their beliefs about the best ways to implement the reforms and adopt these tactics. But the diffusion of different implementation tactics to River and Harbor cannot be completely explained by the concepts advanced in prior studies of vicarious learning.
Political scientists and sociologists have shown that the process of vicarious learning is shaped by an availability bias, in which actors are most likely to learn from peers who share their norms and beliefs and from highly successful actors or outcomes (Dobbin, Simmons, and Garrett, 2007), and by a theoretical bias, in which actors are most likely to learn about practices that are supported by current theory (Lee and Strang, 2006). My findings add to our understanding of how vicarious learning occurs by demonstrating that actors’ vicarious learning processes may be shaped not only by an availability bias and a theoretical bias but also by an experience bias. This study demonstrates that, in addition to learning from the solutions that are most available to them or are supported by research in vogue, actors also learn from the solutions that seem correct to them because they have successfully used the same kind of solution in the past. River and Harbor managers had the same solutions available to them because they were in the same network, so their different tactics cannot be explained by an availability bias. And they were exposed to the same theories of change from the granting organization and their professional journals, so their different tactics cannot be explained by theoretical bias. The reason that Harbor managers doubled down on the engagement tactics they had used in Phase 1 while River managers switched after Phase 1 to tactics of enlisting subordinates was because of an experience bias: managers at River and Harbor were each exposed to the same arsenal of tactics, but each chose a subset of these tactics to learn from based on the kind of solution that had been successful for them in the past. It was lucky for River managers that a solution similar to one that had worked for them in the past turned out to be successful in the PCMH reforms; Harbor managers also chose a solution similar to one that had worked for them in the past, but they failed by doing so. As prior studies have shown, vicarious learning is not a purely rational process. What we gain from this study is that the new data actors choose to add to their prior knowledge to revise their behavior is shaped by their prior experiences. When looking to others for solutions, actors need to guard against such experience biases stemming from familiarity with particular kinds of solutions that have worked for them in the past.
Generalizability and Future Research
Future research could explore how the concept of subordinate activation tactics is applicable to other cases of micro-level institutional change. First, in the U.S. medical profession, there is often a low degree of urgency for change or low financial or reputational costs associated with not changing because doctors deliver a service to one set of actors (patients), yet a different set of actors pays for the service (payers). Future research could test whether subordinate activation tactics are particularly useful in contexts in which there is a low degree of urgency for change and low financial or reputational costs associated with not changing. Second, the governance structures of U.S. hospitals typically give professionals extensive autonomy. Future research could explore whether subordinate activation tactics are more important in organizations with this kind of governance structure than in organizations with governance structures such as partnerships or managed professional businesses (e.g., Cooper et al., 1996), where professionals may be more amenable to the exercise of formal authority by managers. Third, in U.S. hospitals, as in many professional organizations, subordinate semi-professionals are often highly dependent on managers because they report up through a managerial hierarchy so that professionals’ expert time can be spent doing professional work rather than managerial work. Future research could explore how subordinate activation tactics work when subordinate semi-professionals are not as dependent on managers. Fourth, while the MAs at River reported that the quality of their work life had improved from using these tactics, such tactics raise the possibility of exploitation of the third party by the initiator agents. Future research could explore the costs for subordinate third-party members that stem from engaging in influence attempts with more powerful targets on behalf of initiator agents and how these might be prevented.
Conclusion
This paper details a novel set of tactics that led to change in the most unlikely of circumstances given the extensive autonomy of the professionals targeted for change and the low costs to professionals associated with not changing. The findings demonstrate that subordinate semi-professionals, who have been shown in past research to wield a high degree of informal power vis-à-vis the professionals with whom they work, offer an indirect way for managers to accomplish micro-level institutional change in professional practice. We can expect to see growing ranks inside professional organizations of different kinds of subordinate semi-professionals such as LPNs, paralegals, social workers, administrative assistants, technicians, financial analysts, clerks, bank tellers, EMTs, tax preparers, compliance officers, and teachers’ assistants because of the increasing pressures for managers of professional services organizations to redistribute resources on the basis of competence rather than historical workforce hierarchies and roles. Subordinate activation tactics may be key to implementing changes that members of elite professions, by dint of their professional training and beliefs, resist.
Supplemental Material
DS_10.11770_001839218804527 – Supplemental material for Subordinate Activation Tactics: Semi-professionals and Micro-level Institutional Change in Professional Organizations
Supplemental material, DS_10.11770_001839218804527 for Subordinate Activation Tactics: Semi-professionals and Micro-level Institutional Change in Professional Organizations by Katherine C. Kellogg in Administrative Science Quarterly
Footnotes
Acknowledgements
The author gratefully acknowledges help from Dev Jennings, Lotte Bailyn, Emilio Castilla, Julia DiBenigno, Roberto Fernandez, Sarah Kaplan, Erin Kelly, Tom Kochan, Ray Reagans, Susan Silbey, Ned Smith, Sameer Srivastava, Emily Truelove, Cat Turco, Steve Vallas, John Van Maanen, Ezra Zuckerman, MIT ESWG, Cynthia Braun, Alan Reeder, and three anonymous reviewers. The paper has benefited greatly from comments on earlier drafts by seminar participants at Dartmouth, Kellogg, KVEJJ, Iowa, Michigan ICOS, Northeastern, Ohio State, Stanford, UCSD, UMass Amherst, UMass Boston, Wisconsin, and Yale SOM. This paper would not have been possible without the time donated by providers and staff members at River and Harbor hospitals.
Supplemental Material
Author’s Biography
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.