
Abstract
Given the increase in the proportion of older people as well as the decrease in family size, it can be expected that more and more informal care will fall onto the shoulders of non-kin, such as neighbours. Currently, neighbours rarely provide informal care, and knowledge on their characteristics and motivations is limited. This study advances our knowledge of neighbour caregivers by examining the impact of anticipated reciprocity and previous (negative) caregiving experience. Combining retrospective and factorial survey data on caregiving, we show that people have higher intentions to provide care to a neighbour when the likelihood of reciprocity is high (compared to low) and that prior caregiving experience is irrelevant for intentions to provide care to neighbours. However, our study suggests that the impact of reciprocity may depend on previous caregiving experience; having actual caregiving experience overrides expectations regarding the general norm of reciprocity, but only if the previous caregiver did not experience caregiver burden. With these results, this study indicates that neighbours can form a safety net for those who cannot rely on their family members for care.
Introduction
With various demographic shifts in European societies in the coming decades, the future of healthcare is expected to change substantially. First, as the proportion of older people increases, it is expected that the share of people who require care due to health issues or functional limitations will also increase (Broese van Groenou and de Boer, 2016; Keating et al., 2019). It is unlikely that this increase in care needs will be fully covered by welfare states and formal care arrangements due to rising costs and welfare state retrenchment. Instead, it is expected that people will have to rely more and more on their personal network for health-related care, the so-called informal care (Broese van Groenou and de Boer, 2016).
Informal care is currently largely provided by family members, such as children or spouses (Kloostermans and Schmeets, 2020). However, demographers project family size to decline (Alburez-Gutierrez et al., 2023), making fewer family members available for caregiving. Hence, if demand for informal care is expected to increase, it is likely that non-kin, such as friends and neighbours, will take the brunt of this increase in informal caregiving.
Unfortunately, academic knowledge on informal caregiving by non-kin is limited. Previous research has mostly focused on family caregivers or did not differentiate between kin and non-kin. Studies that explicitly focus on informal care provided by non-kin have mostly studied the experience of informal caregiving (Barker, 2002; Lapierre and Keating, 2013; Nocon and Pearson, 2000; Pleschberger and Wosko, 2015). A few studies have examined selection into caregiving. Yet these studies have related selection mainly to other parts of the care network, such as an absence of children or spouse (Fihel et al., 2022; Jacobs et al., 2016). As a result, our knowledge of what makes non-family members select themselves into caregiving is limited.
Our study fills this gap by focusing on neighbours as potential informal care providers. We argue that neighbours can be a more comparable source of care compared to friends, as most people have neighbours, especially in our context of high population density in the Netherlands where neighbours are by definition proximal. Moreover, the relationship between neighbours is less voluntary than friendship and cannot easily be broken due to the close proximity. Thus, it can be assumed that people are generally willing to have positive contact with their neighbours. By focusing on this so far understudied source of care, we add to the understanding of the complexity of potential sources of informal care (Lapierre and Keating, 2013).
Furthermore, because it is expected that informal caregiving by neighbours will play a larger role in the future but does so less at the moment, we focus on caregiving intentions instead of current behaviour (following Quintiens et al., 2024). In doing so, we can further our understanding of the informal caregiving potential of neighbours and what affects this. Our study thus examines neighbours’ helping intentions for neighbours with a health issue. More precisely, we study the intention to help a neighbour with small caregiving tasks, which is often considered the start of a longer caregiving relationship (Barker, 2002; Nocon and Pearson, 2000).
To understand what may affect these intentions, we combine research on neighbours’ informal caregiving with research on neighbourhood support in general. Both these strands of literature indicate that reciprocity plays a substantial role in help exchange among neighbours (Carruth, 1996; Oudijk et al., 2011; Phan et al., 2009; Ramaekers et al., 2025; Zarzycki et al., 2023; Zarzycki and Morrison, 2021). This entails that people feel more obligated to help neighbours who have supported them in the past and are more willing to help neighbours who are likely to reciprocate their help (Manatschal and Freitag, 2014; Ramaekers et al., 2025). Hence, neighbours may be more likely to help when they expect some form of support in return (Pleschberger and Wosko, 2017).
Furthermore, research has indicated that previous (negative) caregiving experiences may shape intentions to provide care in a new situation (Quintiens et al., 2024). Informal caregiving is argued to build skills, such as time management and communication skills (Bovenberg, 2008; Greenhaus and Powell, 2006). These learned skills are argued to instil a sense of competence in the caregiving role, which may make people more willing and confident to provide informal care again. We expect that negative experiences of caregiving may dissuade people from taking up new care tasks because these may result in a stronger anticipation of the negative impact of caregiving on one's life (Goffman, 1959; Rohr and Lang, 2016). We understand negative caregiving experiences as having experienced caregiving burden, meaning that the caregivers felt that at least one previous caregiving situation felt taxing (Swinkels et al., 2017).
This study examines these two factors to understand whether the role of reciprocity may be negated by previous (negative) caregiving experiences. We argue that expected reciprocity will impact people's willingness to provide informal care less than prior experiences. The norm of reciprocity is a general norm that one may expect others to follow, yet personal prior experiences dominate people's considerations and decisions. This may particularly be the case for negative experiences, as negative experiences have been shown to affect people's behaviour more strongly (Baumeister et al., 2001; Norris, 2021). In summary, we answer the following research question: What role do previous (negative) caregiving experiences play in the relationship between reciprocity and intentions to provide health-related help to neighbours?
To answer this research question, we combine data from a survey on caregiving experiences (Verbakel, 2021) and a vignette study (Ramaekers et al., 2022) conducted among the Longitudinal Internet Studies for the Social Sciences (LISS) panel. In this way, we create a unique dataset that includes both retrospective life course data on caregiving and people's responses to hypothetical caregiving situations (vignette study).
Theory
According to the informal care model (Broese van Groenou and de Boer, 2016), selection in informal caregiving depends on various factors. The first step in selection into caregiving is the demand for informal care. When it has been established that there is a demand for caregiving, three factors determine why informal caregiving is provided according to Broese van Groenou and de Boer (2016): motivation (‘do I want to?’), feelings of obligation (‘do I have to?’) and ability (‘can I?’). Intentions to provide health-related help are mostly shaped after demand for it has been established. Hence, our theoretical framework focuses on the latter three factors.
Both feelings of obligation and motivation to provide care may arise because of the norm to reciprocate help. This norm entails that people's behaviour towards others corresponds with others’ behaviour towards them. For instance, if person A helps person B, it is expected that person B helps person A as well (Falk and Fischbacher, 2006; Gächter and Falk, 2002; Gouldner, 1960). Reciprocity can take many forms, including retrospective reciprocity, where people are motivated to provide support because they have received help and feel obligated to return it (Falk and Fischbacher, 2006; Fehr and Gächter, 2000; Gouldner, 1960), and anticipated reciprocity, where people are motivated to help because they expect reciprocity at a later moment in time (Axelrod, 1984; Simpson and Willer, 2015). The latter form of reciprocity, anticipated reciprocity, can motivate people who are not (emotionally) close to support each other. Given that relationships between neighbours in the Netherlands are generally characterized by low levels support (Ramaekers et al., 2025: 705). We focus on the latter: anticipated reciprocity.
In the literature on informal caregiving, anticipated reciprocity is scarcely investigated. When studies address anticipated reciprocity, they focus on generalized reciprocity, where provided care is not expected to be reciprocated by the care recipient but by others, such as people providing care to their family members with the expectation that other family members (such as children or niblings) will eventually care for them (Zarzycki et al., 2023).
An exception to this is the study by Pleschberger and Wosko (2017). They showed that the anticipation of a direct exchange between neighbours plays a role in caregiving among neighbours. This finding is in line with studies on the exchange of support among neighbours (Curry et al., 2013; Manatschal, 2015; Phan et al., 2009; Ramaekers et al., 2025). These studies reported that anticipated reciprocity motivates people to provide support to their neighbours (Manatschal, 2015; Ramaekers et al., 2025). Hence, it is likely that informal caregiving among neighbours is motivated by anticipated reciprocity as well. Particularly, anticipated reciprocity may motivate people who do not share a strong emotional bond with their neighbours to start helping neighbours with health issues, as they may believe they will eventually gain support by providing help now. Helping neighbours with health issues may later transform into a more intensive caregiving relationship. This leads to our first hypothesis: people have stronger intentions to help their neighbour with health issues when the likelihood of reciprocation by this neighbour is high compared to when it is low.
Motivations to provide health-related help to neighbours are likely not only affected by anticipated reciprocity but are also shaped by past caregiving experiences. Prior experiences shape the lens through which people interpret new situations (Goffman, 1959). Having experience with caregiving likely builds feelings of competence in caregiving and a sense of mastery (Hansen et al., 2013), providing (former) caregivers with the confidence that they can handle another caregiving situation. This means that people are more willing to provide care when they have already done so in the past. Support for this theoretical framework is also found with respect to informal care provided to non-kin specifically. Caregivers report feelings of satisfaction because they care for their neighbour (Nocon and Pearson, 2000) and are more willing to take up new tasks (Quintiens et al., 2024). In short, people with prior caregiving experience are more likely to engage in informal caregiving again.
However, not all caregiving experiences may inform the intention to provide informal care in the same manner. Negative experiences, such as caregiver burden, may weaken intentions to provide care. Caregiver burden refers to a feeling that (previous) caregiving was hard or taxing (Swinkels et al., 2017). People who had this experience in the past may possess the confidence in their competences and ability to provide informal care again yet are not motivated to do so (Zarzycki and Morrison, 2021). They may be more aware of potential negative experiences that may occur during caregiving, which may discourage them from providing informal care again (Bandura and Walters, 1977; Rohr and Lang, 2016). This may even be the case with respect to small caregiving tasks, as these may result in more intense caregiving relationships (Barker, 2002; Nocon and Pearson, 2000).
Taken together, people who have prior experiences but without burden will have the strongest intentions to help a neighbour who cannot do a task due to a health issue. Those with caregiving experience with a burden will avoid caregiving the most likely. Arguably, people without any caregiving experience, so those who cannot base their decision on previous experiences, will be more likely to help compared to those who have experienced burden and less likely than those with experience without burden. This is summarized in hypothesis 2: helping intentions are strongest among people who have prior experience with caregiving but did not experience burden, followed by people without caregiving experience, and are least strong for people with burdensome caregiving experiences.
Prior caregiving experience may also affect the role that anticipated reciprocity plays in the intention to provide informal health-related help to a neighbour. Previous caregiving experience provides a (former) caregiver with a lot of information about the impact of helping people with health issues on their lives and thus shapes how caregivers evaluate new potential helping or caregiving situations (Goffman, 1959). In contrast, general norms such as the norm of reciprocity are less informative in forming expectations about the potential impact of helping, as it is uncertain whether other people will actually adhere to these norms. We argue that as a result, people who have caregiving experience mostly rely on this prior experience instead of anticipated reciprocity in determining whether they want to provide support again, weakening the relationship between anticipated reciprocity and helping intentions. Particularly negative experiences, here caregiving burden in previous caregiving situations, may override reciprocity as negative experiences are more memorable and dominate over positive or neutral experiences (Baumeister et al., 2001; Hoefman et al., 2017). The relationship between reciprocity and helping intentions is strongest for people without caregiving experience, as they cannot rely on real-life experience. Overall, we propose a weakening of the relationship of reciprocity on helping intentions when there is previous caregiving experience, especially negative experiences, leading to our third hypothesis: the relationship between the likelihood of reciprocity and helping intentions is strongest for people without previous experiences, followed by those with caregiving experience but no experience of burden, and least strong for those with burdensome caregiving experiences.
Methodology
For the analyses, we created a unique dataset from two separate surveys that were both conducted in the Dutch Longitudinal Internet studies for the Social Sciences (LISS) panel, thus among the same sample of respondents. The LISS panel is based on a representative sample of the Dutch population (Scherpenzeel and Das, 2010) and is used for a large variety of survey research. In addition to the running panel, researchers can develop additional surveys among the respondents of the LISS panel. The two sources of survey data that we use in this study are such additional data collections, namely, the retrospective caregiving data (Verbakel, 2021) and factorial survey data on informal neighbour help (Ramaekers et al., 2022). 1 We will first discuss both data sources before we explain the operationalization and measurement of the variables in the study. 2
Retrospective caregiving data
The first data source concerns retrospective caregiving data. This data is based on a two-step data collection. In January 2020, the complete LISS panel was asked a screening question: ‘The following questions are about providing informal care to people you know with health problems. These people could be your partner, a family member, a friend, neighbour, acquaintance, or colleague who needs or needed help because of physical, psychological, or mental limitations or because of old age. Examples of informal care are doing household chores, helping with washing, and dressing, keeping company, providing transport, or performing odd jobs. You may have done so for a short period or for a long period. It could involve people known to you to whom you provided care in the past, but could also involve people known to you to whom you are providing care at present. Care provided as part of your occupation or as a volunteer does not count. Have you ever provided this type of care in your life?’.
Of the entire LISS panel, 82.9% answered this screening question (N = 5315) (Verbakel, 2021) with 3758 respondents answering that they had ever provided care (71%) and 1557 respondents answering that they had never provided care (29%). Respondents who said they provide care or did so at least once in their lives were invited for a follow-up questionnaire in March 2020 (the onset of the COVID-19 pandemic did not statistically influence the data collection; see Raiber et al., 2021). There were 3061 respondents (81%) who participated in this follow-up study. In the follow-up, respondents aged below 79 years were asked retrospective questions on their caregiving experiences. 3 This was done for up to seven caregiving episodes, that is, seven periods of their lives where they cared for another person. A more detailed questionnaire was asked for up to three randomly chosen episodes in which burden was measured. From both the screening question and the retrospective data, we can deduce who had caregiving experiences and if these were burdensome.
Factorial survey data
The second data source is based on a factorial survey that was conducted in February 2022. A factorial survey presents respondents with hypothetical situations (vignettes) and asks them how they would respond to them (Auspurg and Hinz, 2015; Fekjær et al., 2023). A key characteristic of factorial surveys is that the description of the vignette is varied on a limited number of elements. In the case of our factorial survey data, respondents were asked to imagine that they had just moved to a new neighbourhood. One of their new neighbours asked for help with sweeping leaves from their garden. Then a description of the neighbour was presented, and respondents were asked how likely it was that they would agree with the request. A (translated) example of a vignette is included in Appendix A.
Every respondent was presented sequentially with three random vignettes. 4 After each vignette, the respondents were asked how likely it was that they would accept the request for help. They were also told before a new vignette that they should consider the new vignette as an entirely different situation and should not take into consideration the characteristics of the previous vignette.
Vignettes varied on three elements: (a) reason for requiring help, (b) helpfulness to other neighbours and (c) likelihood of reciprocity. The level of helpfulness to other neighbours was expressed in three dimensions (unhelpful, neutral and helpful), likelihood of reciprocity in two dimensions (likely and unlikely) and reason for requiring help in two dimensions (health problems and being busy). Vignettes always differed on two elements from previously shown vignettes. See Table 1 for an overview of the three dimensions.
Dimensions and categories used in the vignettes.
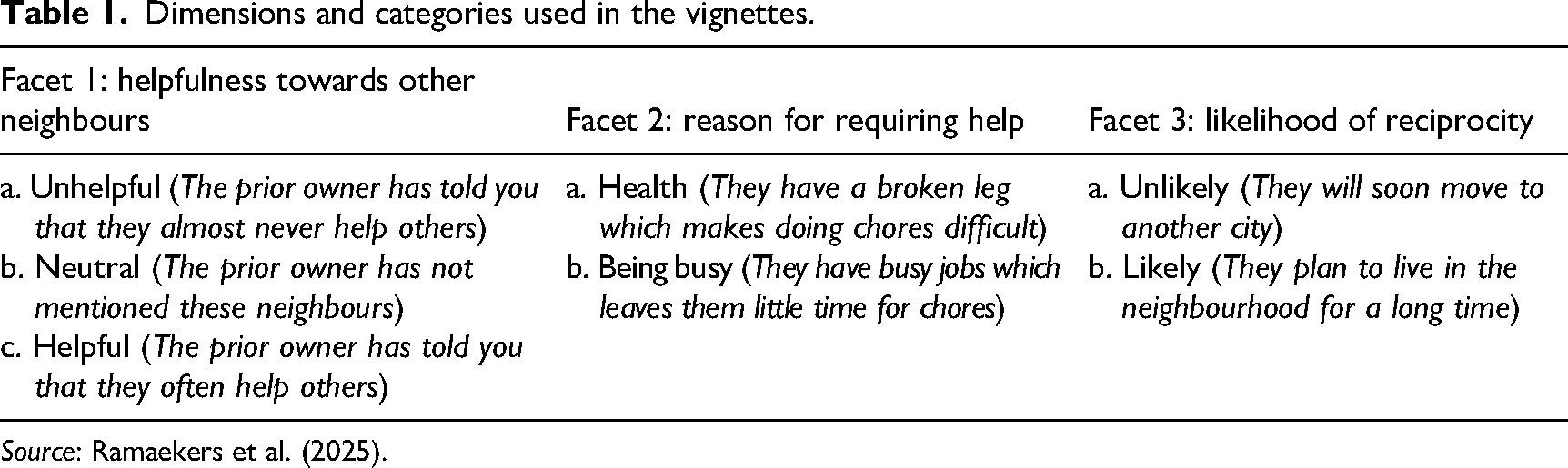
Source: Ramaekers et al. (2025).
Because every respondent reviewed three vignettes, the data consisted of 3312 observations over 1104 respondents. Our study focuses on informal caregiving (defined as providing support that is required because of health or elderdom reasons), so we only use vignettes in which the neighbour was presented as needing help due to health problems. That halves our dataset into 1652 observations over 1104 respondents.
Combining data sources
Both surveys were conducted among the same respondents. This allowed us to match the retrospective caregiving data to the responses to the factorial survey. However, not every participant participated in both surveys. We selected respondents who had participated in the factorial survey and in the screening question. Respondents who indicated in the screening that they (ever) provided care but did not answer the retrospective caregiving questionnaire were excluded. This resulted in 1202 observations on the vignette level over 810 respondents.
Despite the surveys being conducted among the same panel, there is a time lag between the two data collections. The retrospective caregiving data were collected in March 2020 and the factorial survey data in February 2022. Fortunately, the LISS panel is surveyed every year on informal caregiving in their core module on social integration and leisure. The core module asks all respondents to report whether they provided informal care in the 12 months before the survey. Afterwards, they are asked a short set of questions about their caregiving, among which is a measure of caregiver burden. We used data from the 2020 and 2021 social integration and leisure modules to bridge the gap between the retrospective and factorial surveys (see also robustness checks).
Measurements
The dependent variable in this study is intentions to help a neighbour with health issues, from now on referred to as caregiving intentions. In response to each vignette, respondents were asked how likely it was that they would help the neighbour. They could respond on a scale from 0 (very unlikely) to 10 (very likely). After selecting respondents on participation (see the ‘Combining data sources’ section for further explanation), there were no missing values on the dependent variable.
The measurement of likelihood of reciprocity is based on the reciprocity dimension of the vignette. As shown in Table 1, neighbours were described to respondents either as ‘planning to move to another city soon’ (category 0, low likelihood of reciprocity; see Appendix A as an example) or as ‘planning to stay in the neighbourhood for the foreseeable future’ (category 1, high likelihood of reciprocity). A manipulation check confirms that people interpret these descriptions as low and high likelihood of reciprocity (Ramaekers et al., 2025: 20).
Caregiving experience was based on two questions. First, we used the screening question on informal caregiving to determine whether someone had caregiving experience (1) or not (0). For people who reported that they did not have caregiving experience, we checked whether this had changed between 2020 and 2022, using the 2020 and 2021 social integration and leisure core modules. If respondents indicated in these modules that they had given care in 2020 or in 2021, they were considered as having caregiving experience (1). This applied to 14 respondents (2%).
Second, we determined whether caregivers had burdensome caregiving experiences, using the statement ‘I found it taxing to provide care to [name care recipient]’. This question was asked about a maximum of three (random) caregiving episodes that a respondent had reported. Respondents were categorized as having experienced caregiving burden when they answered, for at least one episode, that they (completely) agreed with this statement. For respondents who reported that they provided care but never experienced burden, we checked whether this had changed between 2020 and 2022, using the 2020 and 2021 social integration and leisure core modules. The question on burden and its response options in these modules are slightly different from the retrospective data, namely, ‘On a scale from 0 to 10, did you find it taxing to provide informal care?’ 5 Respondents were categorized as having experienced caregiver burden when they answer 6 or higher (10 respondents; 1%). Based on these two questions, we divided respondents into three categories: no caregiving experience, caregiving experience that was not burdensome and burdensome caregiving experience. As non-caregivers are not able to have a caregiving burden, we had to make the combination of caregiving and burden a categorical variable (to avoid zero inflation). This results in less information on the side of burden yet allows us to keep the comparison with non-caregiving as central to our research question.
As we try to determine how past experiences shape current intentions and considerations surrounding informal caregiving, we want to avoid attributing the impact of other characteristics that determine informal caregiving to past (burdensome) experiences. Therefore, we control for a large set of control variables that are based on the informal care model (Broese van Groenou and de Boer, 2016). We control for gender (0 = male, 1 = female), age (in years) and education (ranging from primary school to university degree). Moreover, we control for working hours, number of children and having a partner. We also control for the level of religiosity, using four categories that range from ‘certainly not being religious’ (0) to ‘being very religious’ (3). This control variable is derived from another core module of the LISS panel. Not every person in our sample participated in this core module, which introduces missing values on this variable. To keep the sample as large as possible, we added a fifth category to this variable for missing values. Another control variable concerns subjective health. Respondents were asked to rate their health on a scale from ‘poor’ to ‘excellent’, which we divided into two categories good (‘good’, ‘very good’, ‘excellent’) and poor (‘poor’, ‘moderate’). Subjective health is also derived from another core module of the LISS panel, which introduces new missing values. To account for this, we added a third category to this variable for missing values. A final control variable that may shape current caregiving intentions is norms on whose duty to care. Respondents could answer the question on whose duty it is to provide care with ‘mostly a government duty’, ‘(slightly) more a government duty’, ‘(slightly) more a personal network duty’ and ‘mostly a personal network duty’.
In addition to these control variables on the level of the respondent, we also control for vignette characteristics. First, we control for the other dimension of the vignette: perceived helpfulness. Despite not playing a role in our theoretical framework, it is important to control for this dimension of the vignette, as we only use half of the vignettes. Therefore, a correlation between reciprocity conditions may exist. To avoid misspecification, we include the three levels of helpfulness in the model, with the unhelpful condition serving as the reference category (see Table 1 for an overview of the wording of these conditions). Second, we control for the order in which vignettes were presented.
The descriptive statistics of all variables are included in Table 2.
Descriptive statistics (N observation = 1202, N persons = 810).
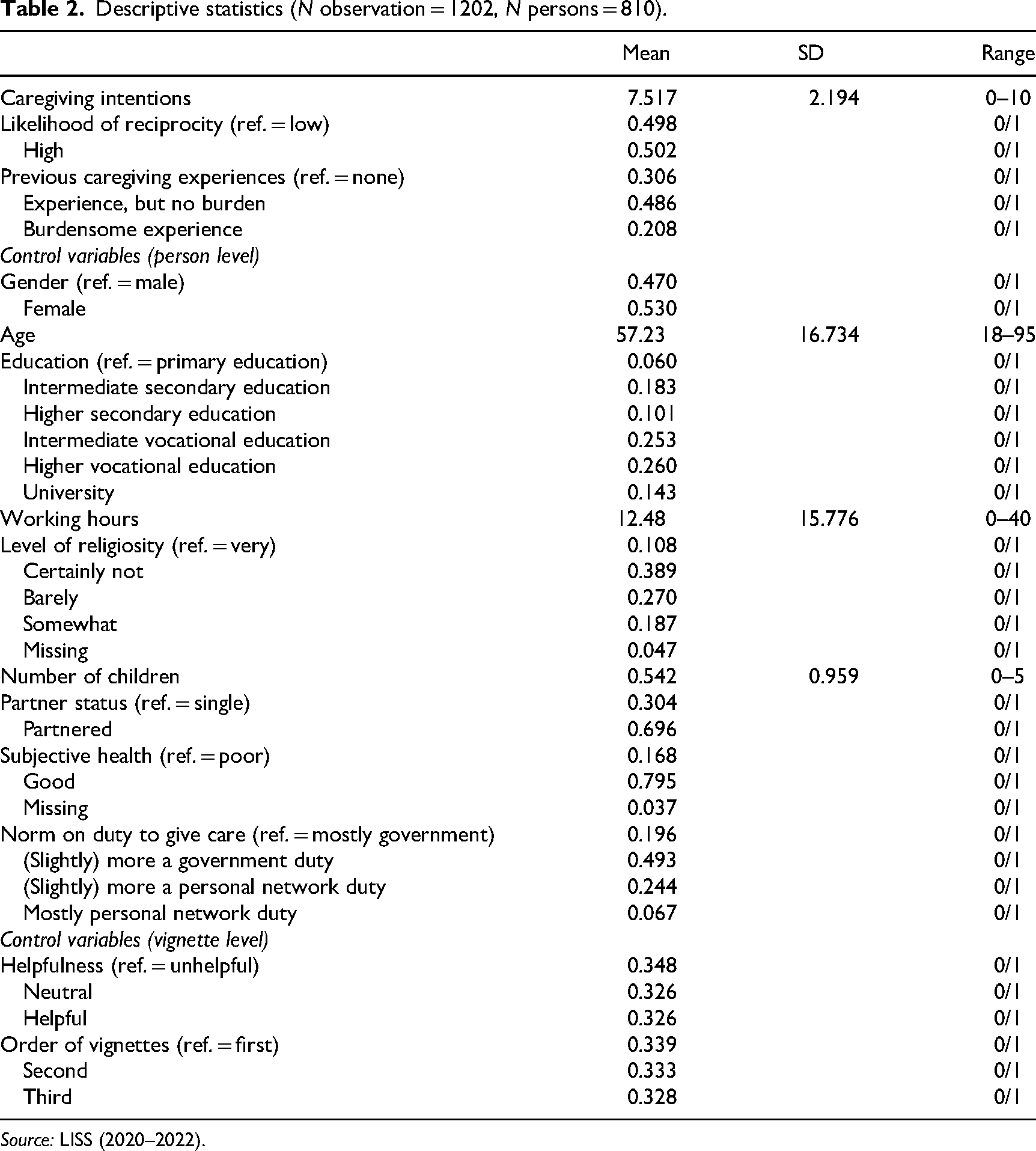
Source: LISS (2020–2022).
Analytical strategy
As a start, we perform bivariate analyses between the dependent and independent variables. For the relationship between reciprocity and caregiving intentions, we perform a t-test. For the relationship between caregiving experience and caregiving intentions, we perform an ANOVA.
For our multivariate analyses, we decided to employ multilevel regression analysis that nests vignettes into persons. This means that we take into account the nested structure of our data, with respondents evaluating multiple vignettes. We estimate random intercepts for each respondent to account for the different baselines of the intrinsic motivation of each respondent to care for someone, independent of the situation (vignettes) presented to them. This analytical approach follows best practice for factorial survey (Auspurg and Hinz, 2015). Given our aim to test an interaction between a vignette characteristic (reciprocity) and a respondent characteristic (caregiving experience), it would be preferable to also estimate random slopes (for reciprocity). The idea behind random slopes is that individual respondents have their own slope in the model, meaning that it is accounted for that the decision process to provide care, depending on our variables of interest, can vary per respondent. However, the design of the factorial survey and our selection in vignettes have resulted in too few degrees of freedom to do so, meaning we were not able to compute these models. The impact of not including random slopes is likely minimal for our results, as it is a detail in the model specification. Yet we decided to present different alternative analysis strategies along with our main analysis (see their descriptions in the ‘Alternative analytical strategies’ section).
The intraclass correlation coefficient (ICC) of our model is 85.9%. This high level of intraclass correlation indicates that the majority of the variance can be ascribed to differences between persons (such as differences in caregiving experience, education or health). The minority of the variance can be ascribed to differences between vignettes (within a single person), such as anticipated reciprocity and level of helpfulness towards other neighbours. In terms of power, this division between variances between and within persons suggests that the power to find differences by caregiving experience is high and the power to find differences between reciprocity conditions is much lower.
Results
Bivariate analyses
Table 3 reports the results from the bivariate analyses. The table shows that people have significantly (p = 0.007) higher intentions to provide care to the neighbours when they believe the likelihood of reciprocity is high (mean of 7.7) compared to when they believe the likelihood of reciprocity is low (mean of 7.3). This is in line with hypothesis 1.
Bivariate analyses for the relationships between caregiving intentions and likelihood of reciprocity (t-test) and between caregiving intentions and caregiving experience (ANOVA).
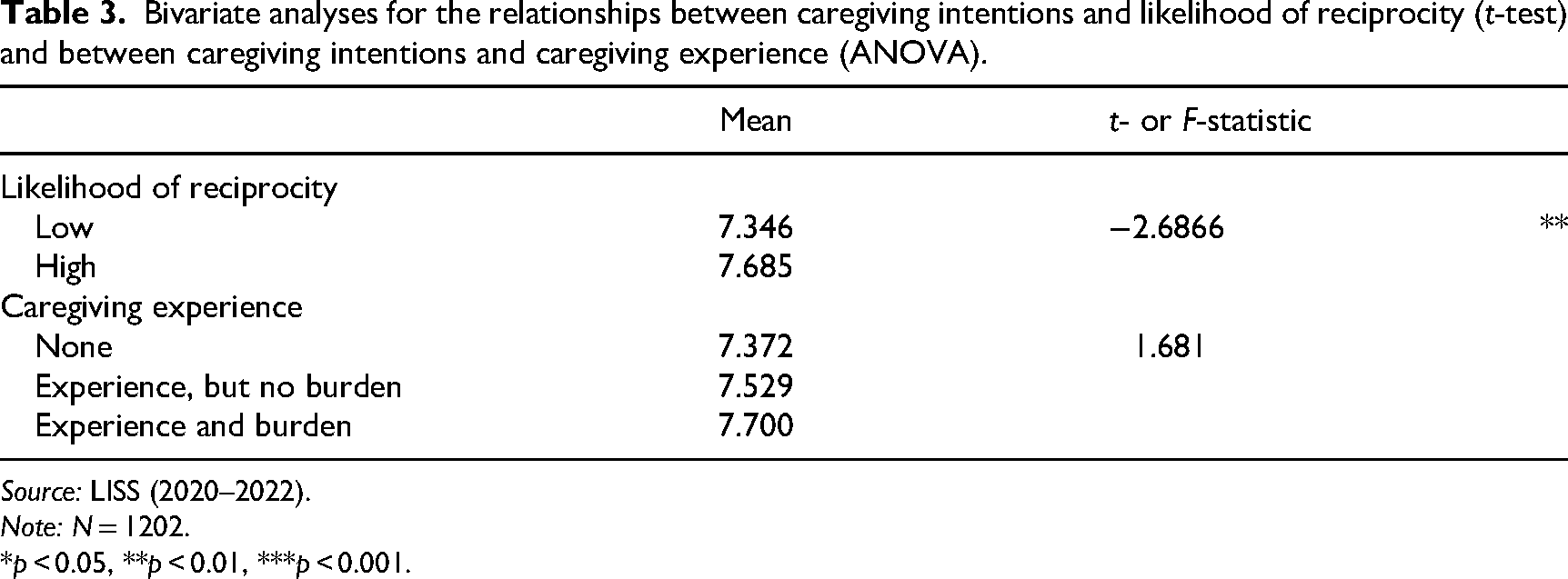
Source: LISS (2020–2022).
Note: N = 1202.
*p < 0.05, **p < 0.01, ***p < 0.001.
However, we do not observe any statistical differences in caregiving intentions by previous caregiving experiences (p = 0.187). Regardless of whether people had caregiving experience and whether this included caregiver burden, their caregiving intentions do not significantly differ. This opposes hypothesis 2.
Multilevel regression analysis
Tables 4 and 5 report the results from the multilevel regression analyses. Model 1 (Table 4) includes the likelihood of reciprocity and the control variables on both the person and vignette levels. This model reproduces the bivariate results; people have higher intentions to provide care to their neighbours when the likelihood of reciprocity is high compared to when it is low (B = 0.19, p = 0.002). This means that the effect is not explained by the nested structure of the data or any of the control variables. This finding is in line with hypothesis 1.
Multilevel regression results explaining caregiving intentions.
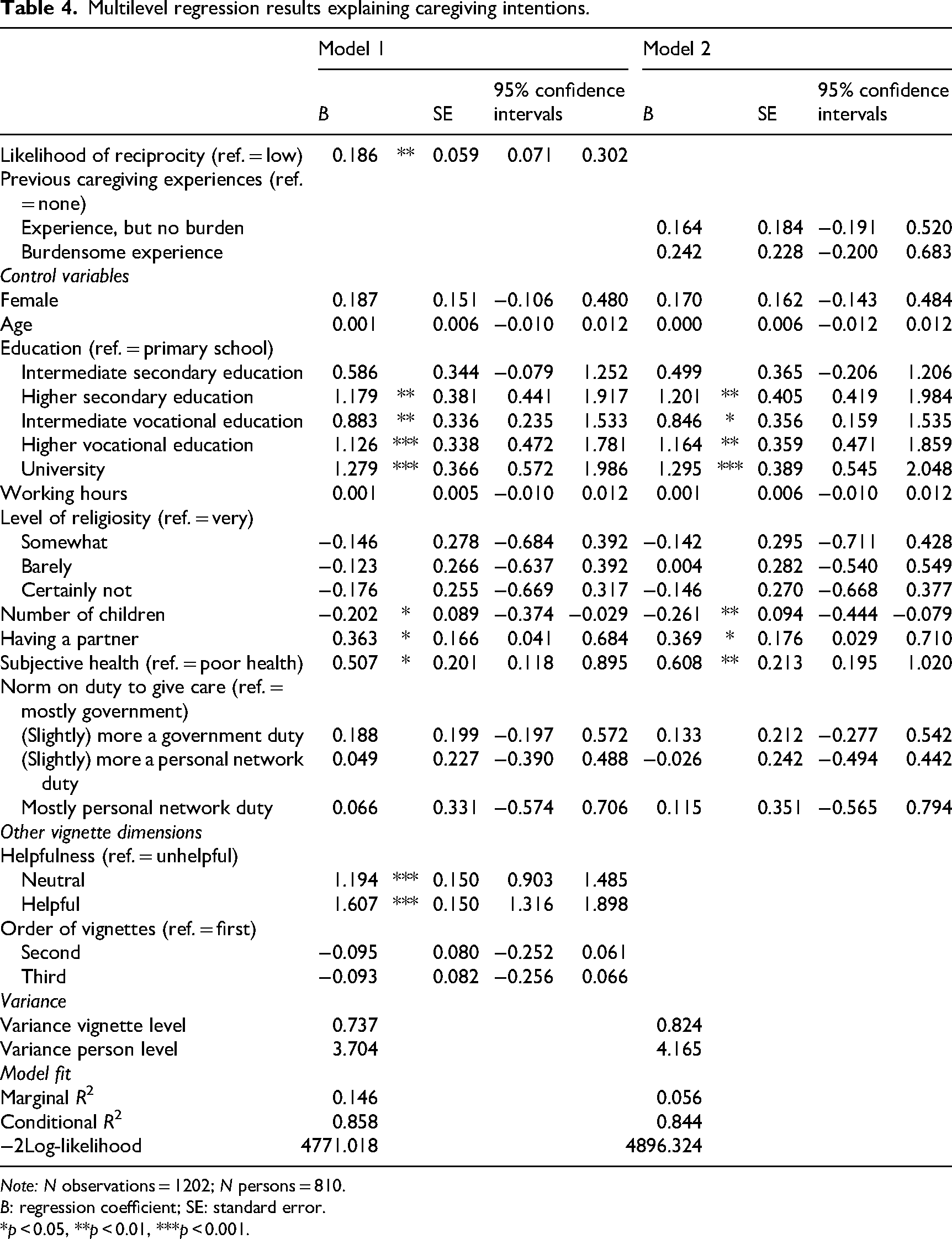
Note: N observations = 1202; N persons = 810.
B: regression coefficient; SE: standard error.
*p < 0.05, **p < 0.01, ***p < 0.001.
Multilevel regression results explaining caregiving intentions.
Note: N observations = 1202; N persons = 810.
B: regression coefficient; SE: standard error.
*p < 0.05, **p < 0.01, ***p < 0.001.
Model 2 (Table 4) includes previous caregiving experience and the control variables at the person level. This model also reproduces the bivariate results; there are no significant differences in caregiving intentions depending on caregiving experience (compared to no caregiving experiences: without burden, B = 0.16, p = 0.371; with burden, B = 0.24, p = 0.290). This finding contrasts with hypothesis 2, where we expected that those with negative experience would especially have lower caregiving intentions.
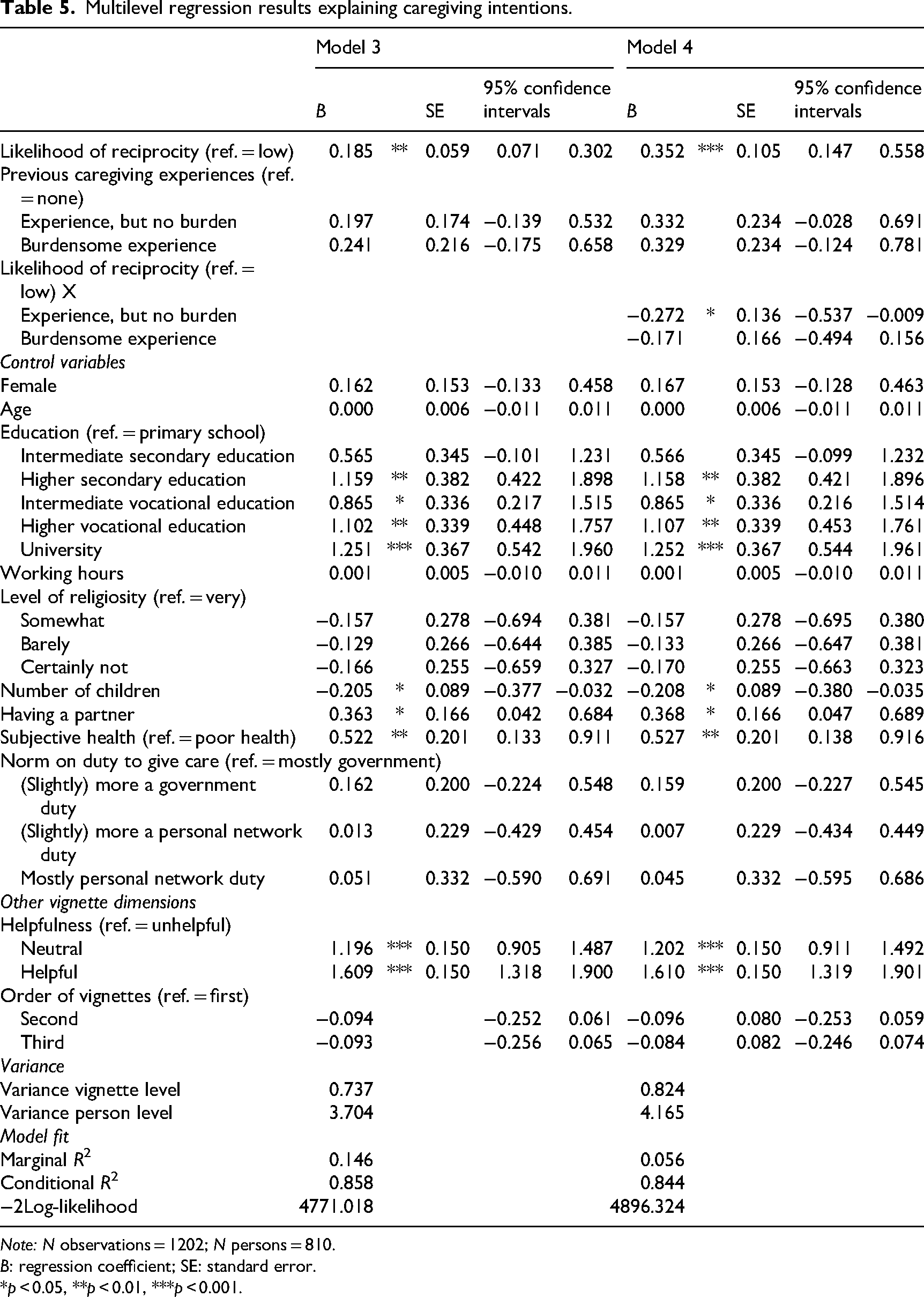
Including both the likelihood of reciprocity and previous caregiver intentions in the same model (model 3; Table 5) does not lead to different conclusions; the likelihood of reciprocity affects caregiving intentions (B = 0.19, p = 0.002), but previous caregiving experience does not (compared to no caregiving experiences: without burden, B = 0.20, p = 0257; with burden, B = 0.24, p = 0.264). Model 3 also indicates that people with higher levels of education, a partner and good health have stronger caregiving intentions. The more children a person has, the weaker their caregiving intentions.
Model 4 (Table 5) reports on the interaction between reciprocity and caregiving experience. This model shows that the impact of the likelihood of reciprocity depends on a person's previous caregiving experience. The difference in caregiving intentions between situations in which the likelihood of reciprocity is high and situations in which the likelihood of reciprocity is low (B main effect = 0.35, p = 0.001) is smaller among people who have previously provided informal care but did not experience caregiver burden (B interaction = −0.27, p = 0.045) than among people who have never provided informal care. This means that reciprocity was less important for those with caregiving experience than for those without caregiving experience, which is in line with hypothesis 3. Yet the impact of the likelihood of reciprocity does not differ between people who have experiences of caregiver burden compared to having caregiving experiences without burden and non-caregivers (B interaction = −0.17, p = 0.303), which opposes hypothesis 3.
Alternative analytical strategies
Although we are confident that our analytical strategy was the best option given the structure of the data and based on best practices (Auspurg and Hinz, 2015), we acknowledge that it is a disadvantage that we were not able to estimate random slopes. To check the robustness of our findings, we employed two alternative analytical strategies (see Supplementary Table A1 for an overview of the coefficients of the effects of interest in each model) and compared their results to the results of our main analyses (see Tables 4 and 5).
For the first alternative strategy, we removed our selection of vignettes in which the neighbour needs help due to health issues. We used all vignettes, including vignettes in which the neighbour needs help for other reasons. An advantage of this approach is that the inclusion of the additional vignettes increases the degrees of freedom, allowing us to estimate random slopes. To produce results for caregiving intentions, it is necessary to then interact with the direct effects of reciprocity and caregiving experience, as well as the interaction between them with the reason for requiring help, resulting in three-way interactions. As a disadvantage, both vignettes in which help is required due to health reasons and vignettes in which help is required due to other reasons are used to estimate random slopes, even though we are only interested in vignettes in which help for health problems is required.
For the second alternative strategy, we used our original data selection. However, we added person-fixed effects instead of nesting vignettes in persons and estimating random intercepts. To do so, we added a dummy variable for every respondent, eliminating differences between persons, allowing us to focus solely on differences between vignettes. The advantage of this approach is that it is a more parsimonious model, as it is not necessary to estimate random slopes. The main disadvantage of this approach is that we can estimate only the direct effect of reciprocity and its interaction with previous caregiving experience. The direct effect of caregiving experience cannot be estimated because all differences between respondents are eliminated.
The results of these alternative analytical strategies produce uniform results with respect to the direct effects of reciprocity and caregiving experience. Both models report that people have higher caregiving intentions when the likelihood of reciprocity is high compared to when the likelihood of reciprocity is low. Furthermore, neither of the additional models indicates that caregiving intentions differ by caregiving experience. These findings indicate that our first two findings are robust.
However, this does not apply to the interaction effect that we report in model 4 (Table 5) between reciprocity and having non-burdensome caregiving experience. The random slopes model produces an interaction term that is in the same direction as the one from Table 5 but is non-significant (B = 0.014; p = 0.952). The interaction term in the person-fixed effects model is in the same direction at a significance level of 10%. Even though the direction of the interaction is stable, we are less certain because of the marginal significance. Hence, this interaction should be interpreted with more caution until it can be replicated.
Additional robustness checks
In addition to the alternative analytical strategies, we performed two robustness checks. First, prior research has theorized that repeated caregiving may be the result of social norms on who should care for those in need (Verbakel et al., 2024). Because we are interested in understanding how providing informal care may change caregiving intentions, we control for people's social norms. However, this may explain why we do not find a relationship between previous caregiving experiences and caregiving intentions. To shed more light on this relationship, we removed social norms as a control variable. Doing so did not lead to different conclusions. Hence, this is not the reason we do not find a relationship between caregiving experience and caregiving intentions.
Second, we removed any person who changed their answer on having cared or having experienced burden between 2020 and 2022. As these changes are based on responses to a different questionnaire than the other responses, this may have resulted in lower reliability, and these observations may disproportionately affect the results. However, we find that removing these observations does not substantially change the conclusions of this paper.
Effect size of main effects
We can thus conclude that our findings with respect to the main effect, which is a positive effect of a high likelihood of reciprocity and no effect of caregiving experience on caregiving intentions, are robust. However, the effect size of reciprocity is rather small. According to Table 5 (model 3), the effect of the likelihood of reciprocity is 0.185 (p = 0.002). This means that the difference in caregiving intentions between a situation where the likelihood of reciprocity is high and a situation where the likelihood of reciprocity is low is 0.084 standard deviation (2.194; see Table 2). This is small in comparison to the other situational factor included in the model. For instance, for helpfulness, the difference between the neutral and unhelpful conditions amounts to 0.545 standard deviation, more than six times the size of the effect of the likelihood of reciprocity.
Discussion
With ageing populations, more people will need health-related care, and also with declining family sizes, non-kin will likely play a bigger role in taking over caregiving tasks. In this paper, we focused on helping intentions for neighbours, who are a likely source of care, considering their close proximity. In more detail, we looked at the impact of reciprocity and previous caregiving experience, finding that people have stronger intentions to provide care to neighbours when they anticipate reciprocity. This is in line with our expectations (hypothesis 1) and with previous research on reciprocity (Falk and Fischbacher, 2006; Fehr and Gächter, 2000; Manatschal, 2015; Nocon and Pearson, 2000; Ramaekers et al., 2025). It highlights that, in the care context, not only does experienced, retrospective reciprocity matter but anticipated help from others as well. This finding has positive and negative implications. It is positive in the sense that it means that people who have not heavily invested in their neighbourhood relations may still be able to rely on neighbours for care. Simultaneously, this finding suggests that people may expect something back from their neighbours when they provide care. However, not everyone, especially those who already experience health issues, is able to give something back.
Our second main finding is that people with (negative) caregiving experiences did not differ in their caregiving intentions from people without caregiving experience. This is in contrast to previous research (Quintiens et al., 2024), which found that people with caregiving experience have higher intentions to provide care to neighbours with health issues. We did find preliminary support for our expectation that anticipated reciprocity is more important for people without previous caregiving experience compared to those with caregiving experience. However, this finding was not robust. We recommend that future research replicate our study with a research design that allows for the estimation of random slopes and with a larger sample.
Interestingly, we did not find any differences between people who have experience with caregiver burden and others, neither with respect to the direct effect nor with respect to the interaction effect. This can be due to the power issues of our models, but there are also potential theoretical reasons for not finding a difference between those with and without experiences of caregiving burden. Caregiving relationships in which a caregiving burden occurs are often paired with other characteristics of the caregiving situation related to the relationship with the care receiver. For instance, caring for a spouse is often related to caregiving burden as one is the sole caregiver, one feels a high obligation to care for the person and the person lives in the same household (Broese van Groenou et al., 2013). The point is that even if one did experience caregiving burden before, one might not expect the same type of negative experiences in a caregiving relationship with a neighbour. This can be interpreted positively for care provision in general: more caregiving, and especially burdensome caregiving, which is expected in the future, will not directly translate into unwillingness to care for their neighbours anymore.
In this study, we combined two unique data collections, both based on a representative sample of the Dutch population, more precisely, retrospective caregiving data on previous caregiving experiences with a vignette study on helping intentions. We were able to combine both reciprocity and experiences of care with each other. Moreover, we accounted for situations that had not occurred yet, which is not possible in another study setup (Ramaekers et al., 2025). However, vignette studies have been criticized for not being able to actually predict real-world behaviour (see Forster and Neugebauer, 2024, for an overview). We recommend that future research based on past behaviour validates our findings further. Another angle for future research would be to replicate our findings in other contexts. The Netherlands is a context in which there is high trust (Statistics Netherlands, 2019) and neighbourhood care is relatively high (Raiber, 2024), meaning that the respondents might have been more likely to agree to care for their neighbours and believe in reciprocity compared to other contexts in Europe. This could mean that the findings are less likely to be replicated to the same extent in other contexts, yet these assumptions are worthwhile to examine in more detail.
Another advantage of our approach was that we could look at helping intentions that are comparably low key, meaning that it is a small task to help the neighbour with removing leaves from their front yard. Previous literature argues that the time investment in helping does indeed matter (Qvist, 2024). One could argue that this task is too small to matter for the caregiving context, considering that we look only at vignettes for someone with a broken leg (health issue). This could relate to our null findings for caregiving experiences. The respondents might not have interpreted the vignette as being related to their previous caregiving experiences, as they did not interpret it as care. Ideally, we would have liked to also compare the willingness to provide bigger tasks; however, these are not available in the data. Yet we argue that the small tasks particularly present an interesting case. It is the most likely case to say yes to. In our case, a reduced willingness is a clear sign of a person not wanting to help with a task one is able to do (as it is presented in the way that the person was already removing leaves from their own yard). Bigger tasks bring more constraints that are potentially less dependent on reciprocity and previous caregiving, which we were interested in. Furthermore, previous literature highlights that these initially small tasks are needed to build up a caregiving relationship (Barker, 2002; Nocon and Pearson, 2000).
Overall, we can conclude that even if there is more caregiving and, therefore, also potentially more caregiving burden in the future, those experiences do not negatively influence the willingness to help a neighbour. This is even more true if there is anticipated reciprocity. In the context of ageing societies, where families are getting smaller, being able to rely on neighbours is getting more crucial. Taken together, this means that in a society where the norm is high to care and give care back, neighbours can be considered a safety net for those experiencing health problems.
Supplemental Material
sj-docx-1-asj-10.1177_00016993251372768 - Supplemental material for Care for thy neighbour: A study of neighbours’ caregiving intentions by likelihood of reciprocity and previous caregiving experience
Supplemental material, sj-docx-1-asj-10.1177_00016993251372768 for Care for thy neighbour: A study of neighbours’ caregiving intentions by likelihood of reciprocity and previous caregiving experience by Marlou JM Ramaekers and Klara Raiber in Acta Sociologica
Footnotes
Author contributions
Ramaekers and Raiber conceived of the idea for the paper together. Ramaekers conducted the analyses and wrote the first draft of the text. Raiber edited the text and took the lead in the revisions.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors are grateful to the Netherlands Organization for Scientific Research (NWO) and the Dutch Ministry of Education, Culture and Science (OCW) for generously funding the collection of the factorial survey data in the context of its 2017 Gravitation programme (grant number 024.003.025).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The data used in this paper are from the LISS panel and can be found in the LISS Data Archive (https://www.dataarchive.lissdata.nl/). They are open for non-commercial use but do require an account for the LISS Data Archive. The data archive contains the two main sources of data: the retrospective caregiving data (https://doi.org/10.17026/dans-z6w-rd24) and the factorial survey data (https://doi.org/10.17026/dans-zpc-742n), as well as the additional datasets that are used to bridge the gap between 2020 and 2022 and for the control variables: the Social Integration and leisure core modules – wave 13 (https://doi.org/10.17026/dans-z2p-gj2k) and wave 14 (https://doi.org/10.17026/dans-x29-njc5), the Health core module – wave 14 (https://doi.org/10.17026/dans-znw-ka2 m), the Religion and Ethnicity core module – wave 15 (https://doi.org/10.17026/dans-xkw-t8dm), and the Work and Schooling core module – wave 15 (https://doi.org/10.17026/dans-x26-tttv). The R script for data preparation and analysis can be found here: ![]() .
.
Supplemental material
Supplemental material for this article is available online.
Notes
Author biographies
Appendix A – Translated example of the vignette
Source: Ramaekers et al. (2025).
Appendix B – Assigning vignettes to respondents
Each vignette included a profile of the neighbour requesting support. This profile had three dimensions that differed between vignettes. As shown in Table 1, the profile had either three or two levels. In other words, the vignette experiment had a 2 × 2 × 3 design. Because there were no illogical combinations of levels, this resulted in 12 different vignettes. The vignettes were divided over four decks, each with three vignettes (see Tables B.1 and B.2 for all possible combinations). We varied the order of the vignettes within each deck, which resulted in six versions of each deck (see Table B.2). In total, there were 24 different conditions (four decks, each with six versions) to which respondents were randomly assigned.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.