
Abstract
Keywords
Introduction
A number of studies have demonstrated adverse health outcomes of belonging to the social minority groups, which are subordinate in the social hierarchy (e.g. Dannefer, 2003). An important extension to this line of research is the consideration that individuals belong simultaneously to various social groups of which some are subordinate, while others are not. Structural approaches to stratification and health posit a multiple jeopardy hypothesis and argue that individuals who belong to multiple social groups that are subordinate in multiple stratification systems such as race and gender are at a higher risk to suffer from ill-health. A few studies have investigated the multiple jeopardy hypothesis (e.g. being female and black, see Grollman, 2014; Rosenfield, 2012). Yet, the literature is still inconclusive because it lacks a common conceptualization regarding how social minority statuses may intersect and relate to health outcomes when combined. Another important limitation is that the vast majority of relevant studies has been conducted in a single societal context (usually the United States; e.g. Grollman, 2012, 2014), which raises questions about the generalizability of the results and whether there are important societal boundary conditions. Furthermore, perceived discrimination (PD) has been widely assumed to be the reason of adverse health outcomes among social minority groups (see Kazarian and Evans, 2001; Thoits, 2010). Several studies have corroborated this (Pascoe and Smart Richman, 2009), focusing on specific kinds of discrimination, such as ageism (e.g. Vauclair et al., 2014), sexism (e.g. Campbell, 2000) or racism (e.g. Paradies et al., 2015). Yet, PD has rarely been considered as a mediator in studies examining health outcomes for individuals belonging to multiple social minority groups (Bauer and Scheim, 2019).
Hence, the aim of the current research is to use a systematic conceptual and analytical approach as well as cross-national data to examine (a) how social minority statuses and their intersections relate to health outcomes, (b) whether these associations vary depending on the societal context, and (c) whether perceived discrimination constitutes a psychosocial pathway for the (multiple) social minority status—health link.
In this study, we provide evidence on the multiple jeopardy hypothesis using multilevel modelling on cross-national data from round 4 of the European Social Survey. We find that the health outcomes depend on the respective social minority groups and their combinations, with older age and female gender being associated with poorer health outcomes which is especially the case in less affluent countries of the European region. Individuals who belong to two social minority groups, but not three, have generally worse health outcomes than those who belong to just one social minority group. Perceived discrimination only fully mediates the link between social minority status and health in the case of ethnicity providing support for an important psychosocial pathway in this social minority group.
Belonging to multiple social minority groups: A multiple jeopardy
Social minorities are groups of people who are relatively disadvantaged or marginalized in regard to their social position in society relative to the dominant or privileged group. Hence, they have less power and access to opportunities, resources and services, which can be due to various reasons, such as explicit discrimination or structural inequalities in society (e.g. access to healthcare) and cultural differences (e.g. cultural health beliefs and practices). Several studies termed the combination of social minority statuses (e.g. being female and of ethnic minority) a multiple jeopardy. It is synonymous to an increased risk or hazard of physical or mental health. The multiple jeopardy concept was introduced in the 1980s within the intersectionality framework in the field of feminist studies in order to explain the unique forms of experiences black women face because of different overlapping social statuses (Bowleg, 2008; King, 1988). Intersectionality theorists suggest that harmful outcomes depend on the specific combination of social minority statuses because they tend to interact with each other resulting in some emergent properties that do not necessarily reflect a simple sum of its components. King (1988) suggested using the term multiple jeopardy to differentiate it from double or triple jeopardy models, which assume that belonging to two or three social minority groups simply adds up in its harmful consequences regarding discrimination or oppression. Ever since, the jeopardy term has become an increasingly popular framework in other fields as well (e.g. Alley et al., 2010; Bauer, 2014; Harnois and Bastos, 2018) including epidemiology where it has been applied to health outcomes (e.g. Ferraro and Farmer, 1996), yet the conceptual distinction between multiple, triple and double jeopardy is not always maintained (e.g. Rosenfield, 2012).
Empirical studies examining how belonging to more than two social minority groups may be harmful for health outcomes often focused on particular intersections, such as age, race and access to benefits (Dowd and Bengtson, 1978) or age, gender and HIV (McCoy et al., 2015) to name a few. Several studies examined even associations between physical and/or mental health and belonging to more than three social minority, such as in Grollman (2014) and Wemrell et al. (2017). These and other related studies provide crucial insight into how particular combinations of belonging to various social minority groups can impair health. However, the chosen social groups and their combinations as well as the studied health outcomes differ widely, rendering comparisons between studies very difficult. Furthermore, the samples are often from an Anglosaxon cultural context, further attesting to the cultural biases in the psychological literature and compromising the generalizability of the results (Henrich et al., 2010). Most importantly, the studies vary widely in the way they conceptualized and operationalized the effects of belonging to multiple social minority groups, with some taking an additive approach and referring to it as dual disadvantage (e.g. Grollman, 2014) or, in contrast, a multiplicative approach, but referring to it as triple jeopardy (e.g. Rosenfield, 2012). The lack of a common conceptual framework with a corresponding systematic analytical approach compromises the comparability of the studies, so that general conclusions about health outcomes and potential additive or multiplicative effects are hard to draw. In the current study, we adopt a conceptual framework, as suggested by Raver and Nishii (2010), to examine how multiple aversive effects may combine. This allows us to test simultaneously additive and multiplicative combinations and we follow this approach systematically throughout our analyses.
Combinations of multiple effects: Conceptual framework and analytical approach
According to Raver and Nishii (2010), multiple risk factors can have an additive or exacerbating effects. Although these terms were suggested within the scope of perceived discrimination, they can also be applied to social minority statuses. This comprehensive classification of potential patterns of effects allows for a systematic analysis of multiple risk factors on health. It is crucial that the term ‘effects’ used here carries a connotation of causality as conceptual notion.
Additive or cumulative effects
The most straightforward pattern, that is often implicitly assumed in the jeopardy literature, is the additive effect model. This describes a situation in which every social minority status adds to the effect of the other social minority statuses in the same degree as it does in isolation from the other social minority statuses. The model assumes that social minority statuses do not interact with each other, but that the effects simply add up. It implies that each minority status influences health independently of the other social minority statuses, and thus when they intersect, each of them impairs an individual's health in the same degree as it does when examined on its own (Thoma and Huebner, 2013). For instance, the health disadvantage of an ethnic minority woman would be a simple sum of the health disadvantage of being an ethnic minority member (same as for ethnic minority men) and for being a woman (same as for ethnic majority women).
Some studies implicitly adopted an additive perspective in their analytical approach by counting the number of social minority, social statuses or discrimination experiences when examining health outcomes (e.g. Grollman, 2014; Sanders Thompson et al., 2004).
Exacerbation effects
Multiple social minority statuses can interact with each other in such a way that one status exacerbates or multiplies the effect of the others (Beale, 1995; Sidanius and Veniegas, 2000). Exacerbation means that the simultaneous presence of two or more social minority statuses brings about an even greater health risk than the simple sum of risks brought by each status. Hence, combinations of minority statuses can be much more harmful than a single minority status. For instance, research has shown that being female and non-White may lead to worse health outcomes than simply summing up the effects of being female or non-White individually (Bowleg, 2008). This phenomenon suggests that additional social minority statuses can magnify each other in their effect on adverse health outcomes rather than merely adding up. In statistical terms, this is referred to as a multiplicative effect in which an interaction enhances the main effects (cf. Bauer, 2014). Notably, the interaction effect can be substantial even when the main effects of the individual variables are not statistically significant. Such findings would emphasize the importance of considering the combined impact of multiple social identities in understanding health disparities.
The exacerbation idea is consistent with threshold and energy theories (e.g. Wardian et al., 2014). For example, individuals who experience discrimination due to only one kind of social minority status may have enough energy to cope with it; however, additional stressors may undermine their coping ability and result in disproportionately larger harm than the one brought by every single stressor. The idea of exacerbation is important to better understand multiplicative effects when studying health disparities because it can provide a more accurate and comprehensive account of how different forms of social disadvantage can intersect and impact individuals’ lives.
Inurement effects
The exacerbation effect assumes that a combination of multiple social minority statuses results in more harm than predicted by each social minority status individually. However, it is also possible that a combination of social minority statuses leads to a weaker effect because one risk factor may dominate or absorb the effects of others. This can happen because individuals change group status from social majority to minority (e.g. first being female and only later in life transitioning into old age). When an inurement effect is present, individuals get used to (or inure to) their social minority status and develop defensive mechanisms (Raver and Nishii, 2010). When this is the case, the combination of social minority statuses demonstrates less harmful consequences compared to the ones that would occur if they were experienced separately. For example, aging and the accompanying experience of old ageism might be less stressful for ethnic minorities compared to someone belonging to an ethnic majority because the former was able to develop coping mechanisms across their lifespan to deal with discrimination experiences while the latter may face discrimination for the first time in their lives. Indeed, it has been demonstrated that people tend to habituate to stimuli to which they are repeatedly exposed (Diener et al., 2009), which suggests that, under certain conditions, they may build psychological resilience (Fletcher and Sarkar, 2013). 1
In its extreme, the inurement idea implies that belonging to multiple social minority groups does not cause more harm than belonging to a prominent single social minority group. Statistically, an inurement can be detected by an interaction effect that weakens the main (detrimental) effect of a single social minority group.
The moderating role of societal development
The large majority of studies on multiple jeopardies were conducted in the United States focusing on African Americans (e.g. Ferraro and Farmer, 1996), which implies a very specific socio-cultural context. Cross-cultural psychologists have found that numerous psychological phenomena and processes are far from being universal and are moderated by societal variables (Henrich et al., 2010). Hence, the question remains to what extent previous insights into the jeopardy hypothesis from mainly Anglosaxon countries can be generalized to the experience of social minorities in other countries.
One of the most influential variables that generally indicates a favourable context in terms of living conditions and that has been found to be associated with various psychological outcomes, including health outcomes, is the level of economic development (Inglehart, 2018; Oishi and Graham, 2010). In fact, economic conditions universally affect people's daily lives, regardless of whether they belong to a social minority or not. A relatively high gross domestic product (GDP) usually indicates a strong economy with a well-developed healthcare system that provides access to medical care and public health services (Human Development Report, 2019). A country with higher levels of economic development has more resources to invest in healthcare infrastructure, medical research and public health initiatives, such as vaccination campaigns and disease prevention programmes. Higher level of economic development is also related to higher levels of education and employment, which are both associated with better health outcomes: people with higher levels of education are more likely to have access to health information and resources, therefore, making healthier lifestyle choices; while people with stable employment are more likely to have health insurance and access to healthcare. Moreover, countries with higher levels of economic development usually provide better for basic needs related to health, such as clean water, sanitation and nutritious food. Overall, this suggests that a less favourable economic context can create universally harmful conditions for the health of all groups in society, yet the degree to which health is impaired might be exacerbated if individualś also belong to social minorities.
Recently it has been argued that population health can be best understood if structural inequalities at the macro-level are also considered besides the individual-level approach focussing on social minority statuses (Homan, 2019; Homan et al., 2021). The framework of structural intersectionality considers the ways in which social identities and power relations intersect at multiple levels of society to create health disparities by emphasizing the role of structural factors, that is the large-scale social, economic and political forces that constitute the structure and organization of society as a whole, in shaping the social determinants of health. A structural intersectionality approach emphasizes that there are multiple systems of oppression and that structural factors, which systematically subordinate and exclude marginalized groups with respect to resources, opportunities and freedoms in major social institutions, should also be acknowledged and considered in health disparities research. The macro-economic context may create such conditions as also suggested in group conflict theory (e.g. Meuleman et al., 2018). The main tenet of group conflict theory is that group conflict arises from competition over scarce resources. When economic conditions are poorer, the material goods that are the object of intergroup competition become scarcer, thereby leading to more threat perceptions. Moreover, the power asymmetry between groups allows dominant groups to maintain their position of privilege and control over resources via the expression of prejudice. Altogether, this might pose a threat to health equity with social minorities not being afforded equal opportunities in achieving good health due to their background and social status. There is mixed empirical support for this proposition with some authors finding that societal prosperity is indeed negatively related to ethnic prejudice (e.g. Schneider, 2008), while others find that a high GDP is related to positive attitudes towards some social minority groups (e.g. women), but not towards others (i.e. immigrants; Meeusen and Kern, 2016).
Given the dearth of multilevel theories and research on the multiple jeopardy hypothesis (see also Homan, 2019; Homan et al., 2021), we draw on the framework of structural intersectionality and group conflict theory to propose that a poorer economic context is universally harmful, but more so for social minorities due to their subordinate social position in the societal strata which may exclude and marginalize them, and therefore, exacerbate their health risk in these contexts.
The mediating role of perceived discrimination
One of the main psycho-social explanations for why social minority status is related to ill-health is perceived discrimination (e.g. Harnois, 2014; Krieger, 2014; Williams et al., 1997). Perceiving one kind of discrimination has often been found to be negatively related to various indicators of well-being such as subjective well-being (Schmitt et al., 2014) or physical health (Pascoe and Smart Richman, 2009), and even objective health (Paradies et al., 2015). There is also some evidence that perceived discrimination plays a mediating role for the social minority status-health link (e.g. Fuller-Rowell et al., 2012).
Only very few studies empirically tested more than one ground of discrimination as mediators, that is, health outcomes due to belonging to more than one social minority groups as mediated by multiple perceived discrimination. However, they produced somewhat inconclusive results, because most of them did not measure different forms of perceived discrimination (e.g. Grollman, 2014), only differentiated generally between racial and non-racial discrimination (see Stuber et al., 2003), or limited their study to a specific domain (e.g. workplace, see Harnois and Bastos, 2018; Raver and Nishii, 2010). Moreover, they widely differed in their interpretation of the resulting patterns of effects. Nevertheless, there is enough cumulative evidence that perceived discrimination is a psychosocial pathway, which could at least partly explain why belonging to multiple social minority groups is associated with adverse health outcomes.
Current study and hypotheses
In the current study, we focus on intersections of older age, female gender and ethnic minority and examine how they are related to individuals’ subjective health taking also into account the societal context. We then also examine whether PD mediates the (multiple) jeopardy-health link. Following the review above, we expected that each of these social minority statuses is related to poorer health compared to the non-minority (privileged) group (H1). It is noteworthy that old age is naturally associated with health issues, which renders the age comparison somewhat trivial. We treat the main effect of age pro forma, yet our main interest about age concerns testing the intersectionality hypothesis, that is, whether health outcomes are worse if old age is intersected with other social minority statuses.
Based on theories of intersectionality (e.g. Bowleg, 2008), we propose the multiple jeopardy hypothesis, that is, that the specific combinations of social minority statuses result in unique health outcomes, which are not a sum of the separate factors. Therefore, we hypothesized that the combinations of effects of multiple social minority statuses are more complex than additive, meaning that their effects interact with each other (H2). Given the dearth of previous research in this area, we did not hypothesize a specific direction of these interactions (i.e. if these are exacerbation or inurement effects).
Given the importance of the socio-economic context for individuals’ minds and behaviour (Oishi and Graham, 2010), we expected that the multiple jeopardy effect is exacerbated in poorer countries compared to wealthier ones. In other words, we hypothesized a cross-level interaction in that lower levels of socio-economic development demonstrate an exacerbating effect on the link between social minority status and health (H3).
We also expected that perceived discrimination was a psychosocial pathway for the multiple jeopardy effect. Therefore, we hypothesized that PD mediated the effect estimates of single and multiple social minority statuses (H4).
Data and methods
Data and measures
We used data from the European Social Survey, round 4, collected in 2008, which is the only round that included continuous variables of perceived discrimination based on age, gender, and ethnicity/race (European Social Survey, 2018). The initial sample consisted of 56,752 individuals from 29 countries, which decreased slightly (4% of the data) after removing missing values listwise (see Appendices A for descriptive statistics, and the ESS website for the detailed methodological reports). Due to issues with measurement invariance described below we dropped data for Bulgaria. The final sample size included 53,161 observations in 28 countries.
The criterion variable is subjective health measured on a 5-point Likert scale with the question “How is your health in general? Would you say it is very good (1), good (2), fair (3), bad (4), or very bad (5)?”. This measure showed a high reliability and validity across countries (Baćak and Ólafsdóttir, 2017) and is a good proxy indicator of the diagnosed health problems (Idler and Benyamini, 1997). The responses were recoded so that the higher scores reflected better health.
Multiply disadvantaged social statuses included older age, female gender and belonging to an ethnic minority. There is no general agreement on defining old age. We decided to categorize individuals of 60 and older into the social minority old age category (0 = younger than 60, 1 = 60 and older) because this age boundary was close to the average healthy life expectancy in Europe in 2008. 2 Ethnic minority status was assessed through the following question: “Do you belong to a minority ethnic group in [country]?” (1 = Yes, 2 = No) with “belonging” being defined as referring to attachment or identification. The responses were recoded as 0 = do not belong and 1 = belong. Gender was assessed via the interviewer's report of respondent's sex (0 = male, 1 = female) and we considered females to be a social minority.
Discrimination experiences were measured with the following question: “Using this card please tell me how often, in the past year, anyone has shown prejudice against you or treated you unfairly because of your [age/sex/your race or ethnic background]?”, with the response scale ranging from 0 (Never) to 4 (Very often). We opted to use a generalized perception of discrimination since individuals are not always able to identify the sources or grounds they were discriminated against (Bauer and Scheim, 2019). Moreover, the average within-country correlation between the three items is .47 suggesting that participants did not neatly differentiate between the different sources of discrimination. The fact that some people cannot identify the source of discrimination against them does not imply that they cannot recognize discrimination itself. This is in line with major contributions to the literature that relied on the generalized (everyday) discrimination scale (Williams et al., 1997). Hence, we used the three variables of ageism, sexism and racism to indicate a latent variable of overall discrimination. 3 This measure demonstrated measurement invariance across all countries, except for Bulgaria in which the model estimated negative variances. Hence, Bulgaria was excluded from the following analysis. In further analysis we used factor scores predicted by the partial scalar model. Table 1 lists the sample descriptive statistics by country.
Distribution of respondents by multiple minority status.
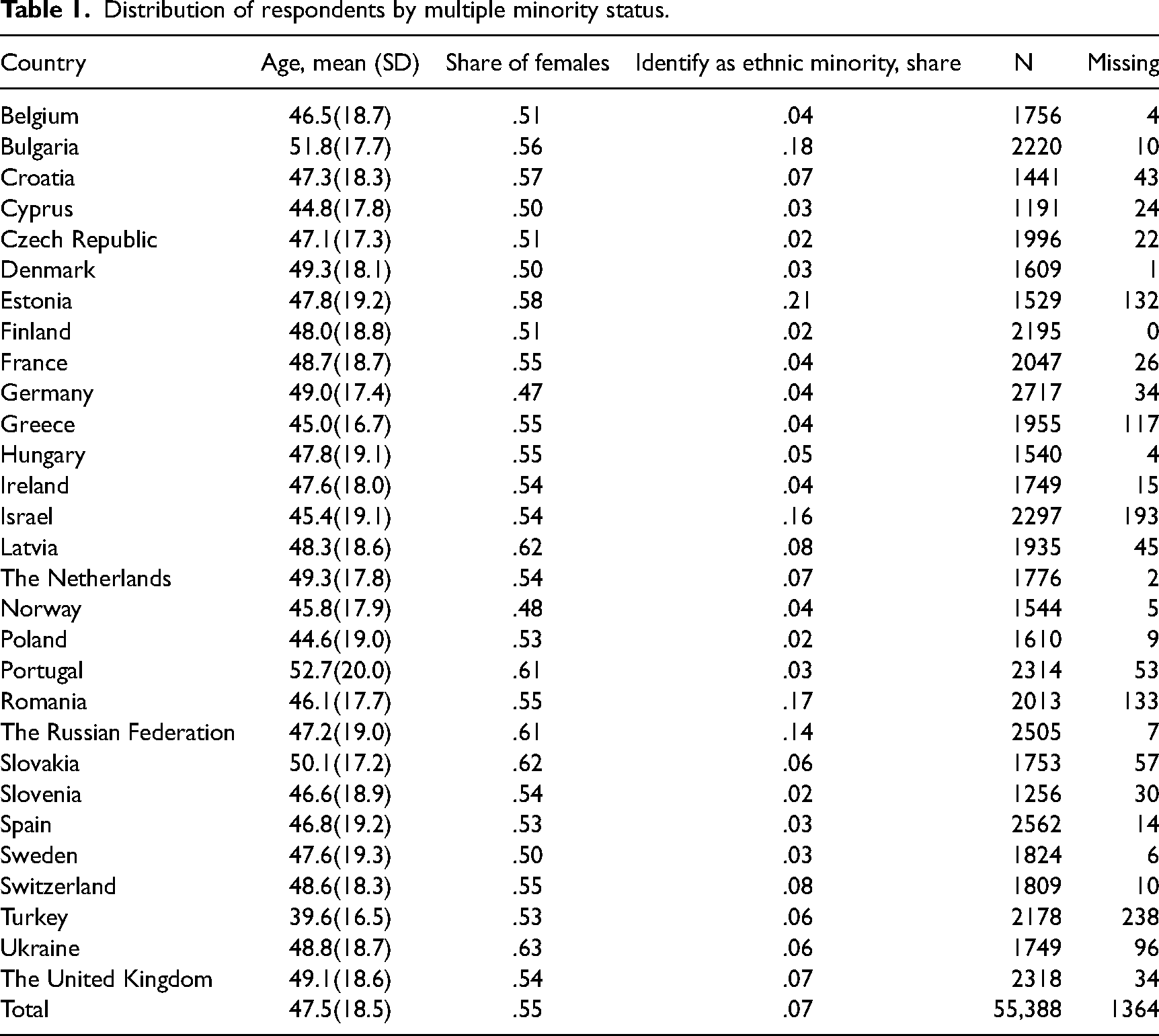
At the country level, we used GDP per capita based on purchasing power parity in 2008 (hereafter referred as GDPpc), which is indicative of the societal context in terms of a country's economic development.
Analytical strategy
Since the data come from a multinational survey in which individuals are nested within countries and multilevel hypothesis are proposed, we fitted a two-level structural equation model to test our hypotheses. To test H1, the model included the direct individual-level effects estimates of social minority statuses and perceived discrimination on subjective health. To test H2, we appended this model with the individual-level interactions of the different social minority statuses. A negative interaction would support an exacerbation effect (given the main effect is negative), a positive interaction would point to an inurement effect (again, given a negative main effect), and a non-significant interaction would point to additive patterns of effects.
H3 stipulates a cross-level interaction effect for the multiple jeopardy hypothesis, which implies the moderation by country socio-economic development. It involved three-way and four-way cross-level interactions that would point to an effect of an additional jeopardy status, namely living in a less developed country.
In order to test the mediation as postulated in H4, perceived discrimination was included as a mediator in the link between social minority statuses, their interactions and health. This allowed calculating the indirect effect estimates of multiple social minority statuses on health via perceived discrimination.
We employed a multilevel structural equation model (SEM) with a latent variable of perceived discrimination indicated by three polytomous items, as shown in Figure 1. The model was fitted with Bayesian estimator, using 16 chains, a minimum of 40,000 iterations combined with 10× thinning. The convergence was tested with potential scale reduction factor < 1.1 for each parameter as well as visually using trace plots. Autoregression was assessed for each parameter and effective sample size. All parameters showed good convergence and most did not show autocorrelation. An exception is the measurement parameter of discrimination (factor loading on sexism and its thresholds), which demonstrated high autocorrelation but at the same time the effective sample size was above 100, so we decided that this was not problematic. Trace plots and convergence-related summaries for each parameter are available in Supplemental materials.
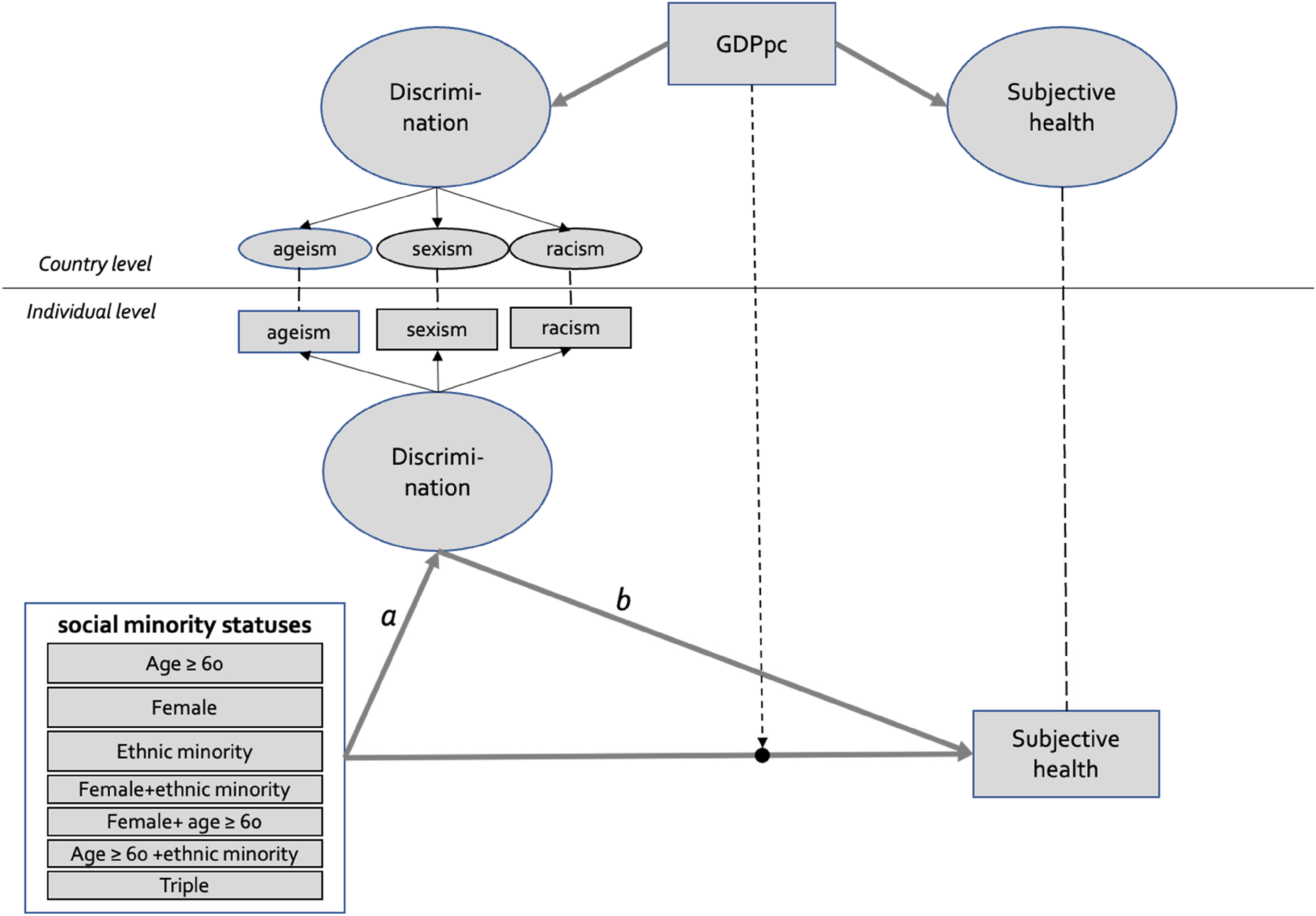
The multilevel structural equation model constructed for estimation of direct, indirect and moderated effects of social minority statuses on health.
The analyses were run using R 4.1 4 and Mplus 8.3 software. The models, tables and figures can be replicated using the Supplemental materials at https://osf.io/mrwt7.
Results
Multiple jeopardy hypothesis
Figure 2 shows the mean levels of health for the majority and social minority groups in all possible combinations. Health rates were substantially lower for older age whereas individuals belonging to other social minority groups as well as their combinations had only slightly worse health than those not belonging to any social minority groups (referred to as ‘no disadvantage’ in the figure). Figure 2 also shows to what extent individuals belonging to the various social minority groups reported being discriminated against. Single social minority group membership related to ethnicity only and its combination with female gender showed the highest rates of discrimination, even higher than the triple jeopardy of old age, female and ethnic minority status. The lowest discrimination rates were reported by older people (both males and females).
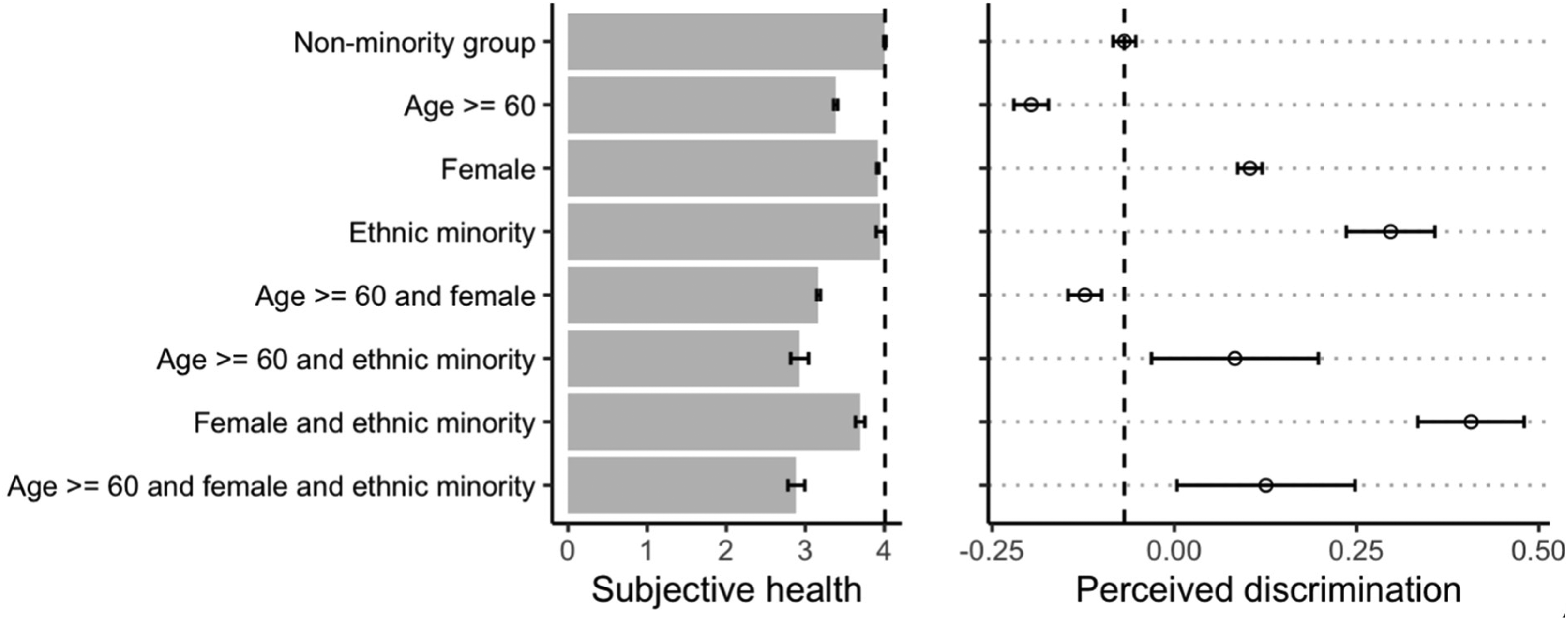
Mean subjective health and perceived discrimination across groups of social minority statuses (pooled sample weighted by population size). The bars show 95% confidence interval of means. Dashed line is the average health/discrimination for the non-minority group.
Next, we estimated the multilevel SEM model in order to test whether these effect estimates are significant. The estimates are listed in Table 2.
Direct, indirect and total effect estimates and interactions of disadvantaged statuses on health as estimated by the multilevel structural equation model.
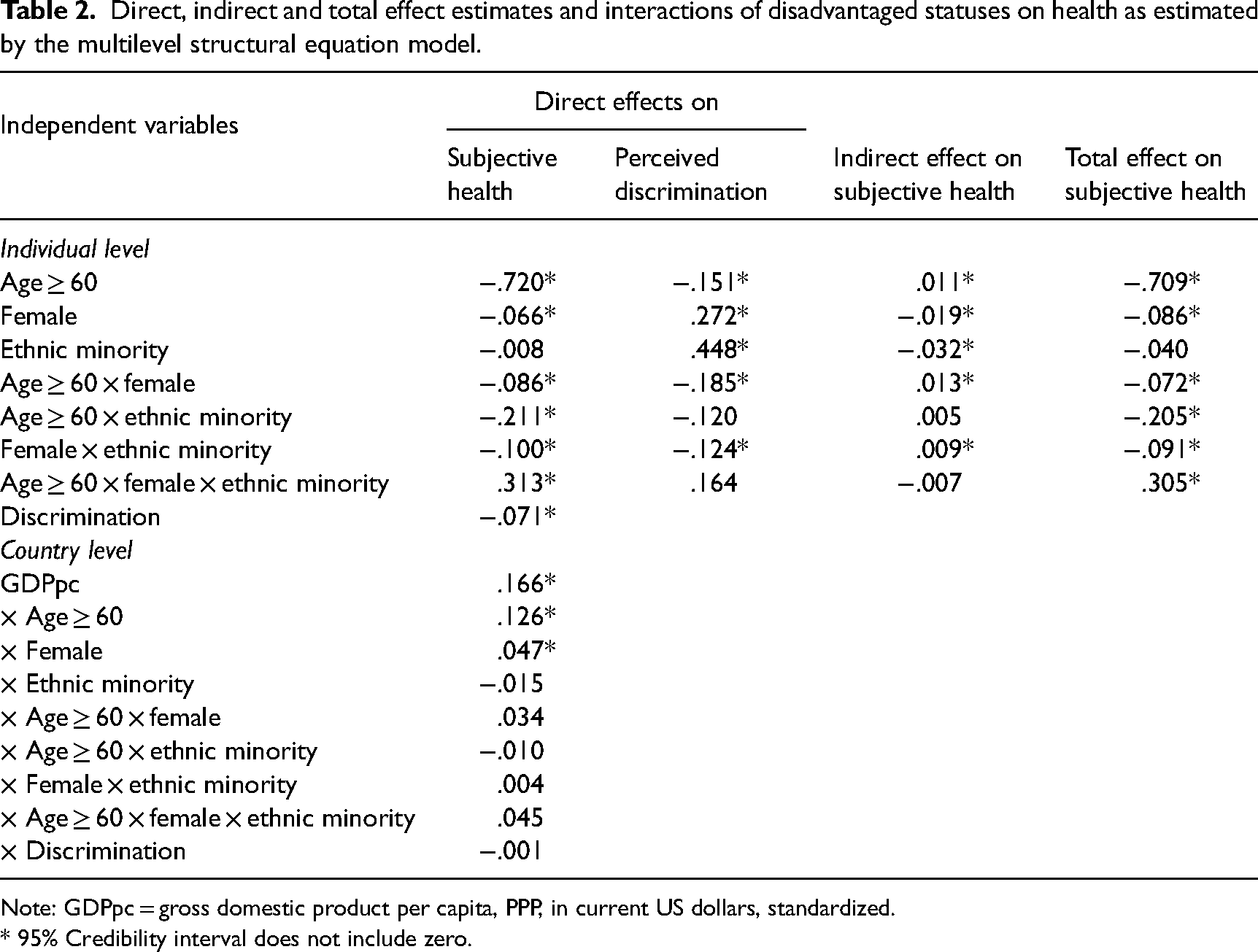
Note: GDPpc = gross domestic product per capita, PPP, in current US dollars, standardized.
* 95% Credibility interval does not include zero.
Effect estimates on health
Supporting hypothesis 1, the main effect estimates of social minority statuses regarding old age and female gender were significant and negative predictors of health. Given that the social minority statuses were dummy coded, their regression coefficients can be directly compared. The model shows that old age has the largest negative effect estimate on health: the health disadvantage for the older (60+ years of age) compared to the younger age groups (<60 years of age) is 0.720 units on the 5-point scale, whereas it is 0.066 units for females relative to males. Most importantly, all two-way interactions involving age were negative: the effect estimate of old age was exacerbated by being female, as well as by belonging to an ethnic minority. The three-way interaction, reflecting an additional health effect of triple jeopardy, turned out to be positive suggesting an inurement effect. This means that the triple combination somehow reduced rather than further exacerbated the single and double disadvantages on health.
Unexpectedly, the main effect estimates of ethnic minority status on subjective health were non-significant, while its interaction with older age and female gender were highly significant and negative. It means that ethnic minority status has health effects only when intersected with other social minority statuses whereas it does not relate to health on its own.
Multiple jeopardy and cross-level moderation by GDP
The main effect estimate of GDPpc on the level of subjective health was positive. Effect estimates of older age, female gender, ethnic minority and their interactions were treated as random in order to test for a cross-level moderation by GDPpc. The results show that while the main effect estimates of older age and female gender were significantly negative, their interactions with GDPpc were positive. In other words, lower GDPpc exacerbated the detrimental health effects of older age or female gender. However, GDPpc did neither significantly modify the effect estimates of ethnic minority status, nor any combinations of the three statuses (see also Figure 3). It can be concluded that the results are only partly consistent with our hypothesis 3 by showing that a less developed socio-economic context exacerbates the health outcomes for those who are old or female, but not for ethnic minorities and any combinations of multiple social minority statuses.
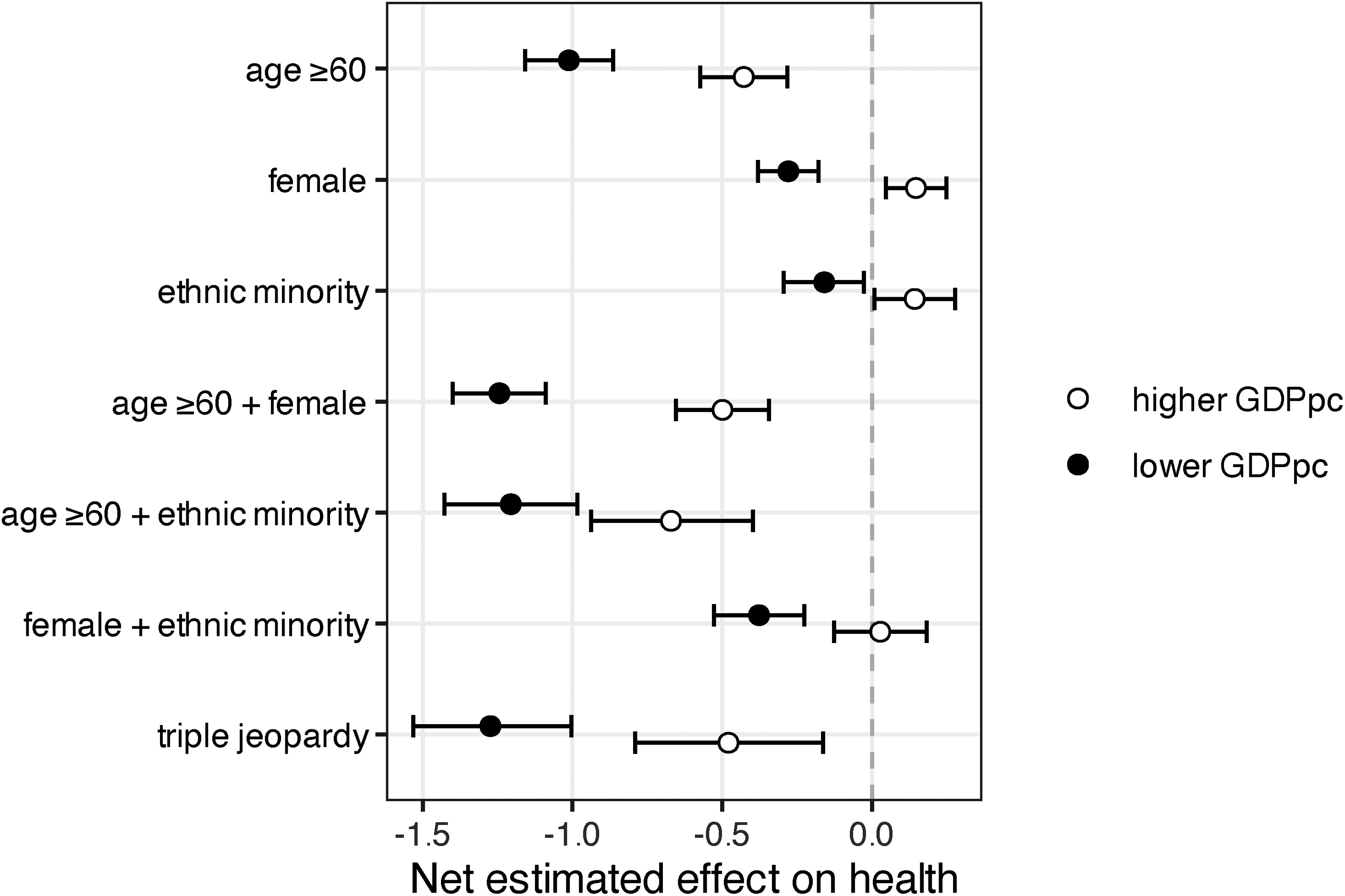
Net estimated effects of single and multiple social minority groups on subjective health across two levels of GDP per capita (average minus 1 SD and average plus 1 SD). Error bars represent 95% confidence interval. Zero represents health in the non-minority (privileged) group.
We used GDP per capita as a contextual variable because it assesses a (un)favourable context that is transversal for different social minority groups. Moreover, GDP per capita is highly correlated with other relevant macro-level indicators (e.g. with health expenditure at .96 for our national sample). There are also important limitations regarding the country-level sample size which does not allow testing multiple country-level predictors at once. Nevertheless, we probed into the robustness of the cross-level interaction of GDP per capita by conducting follow up analyses. The Supplemental materials (Table D and Figure E) show cross-level interactions with health expenditure, social inclusion expenditure, life expectancy, doctors per capita and the Gini income inequality index as contextual variables. The results for health expenditure (and to some extent social inclusion expenditure) are very similar to the results for GDPpc. The variables life expectancy, doctors per capita and Gini index do not produce reliable cross-level interaction effects.
Multiple jeopardy and mediating effects of perceived discrimination
Associations between (multiple) social minority statuses and subjective health (path a) were already reported above. We now turn to the question whether PD mediates these associations. We start with the link between PD and subjective health (path b). As expected, it was significantly negative as can be seen in Table 2. When examining the links between (multiple) social minority status and PD (path a), the results indicated that being female or belonging to an ethnic minority is, as expected, associated with higher perceived discrimination. However, older age is negatively associated with perceived discrimination, meaning that older adults reported less discrimination compared to younger ones. The interactions of female gender with older age and female gender with ethnic minority status were negative. It means that the positive effect estimate of female gender on PD was weaker among older adults or ethnic minorities. The other combinations of multiple statuses were not significantly associated with PD.
Finally, Table 2 lists all indirect and total effect estimates of social minority statuses on health through discrimination. Perceived discrimination significantly mediated the social minority status-health link in all cases, except for the dual combination involving old age and ethnic minority membership as well as the triple combination of old age, female and ethnic minority memberships. Interestingly, the indirect effect estimate of ethnic minority on health was significant, whereas the direct as well as total effect estimates were not significant. It implies that the ethnicity-related health risk is fully mediated by perceived discrimination. And more importantly, this is not the case for doubly or triply disadvantaged groups. Overall, these results supported our hypothesis 4.
In terms of its contributions to the total effect estimates of disadvantaged statuses, indirect effect estimates via discrimination showed very different patterns: for older age, the indirect effect estimate via discrimination was only about 1% of the total effect estimate, for female gender it was 22%, and for ethnic minority it was 80%, and for the combinations of multiple social minority statuses (interactions) it was always below 15%.
Discussion
A popular assumption in the literature on multiple health risks concerning social factors is that every additional social minority status or discrimination experience leads to proportionally worse health outcomes. In our review we showed that the empirical evidence for this is confined to particular social minority groups as well as to the specific societal context of a few countries (e.g. Grollman, 2012, 2014). Our study contributes to these important findings by examining how common they are across different societies and how the multiple health risks combine regarding various salient social categories. Hence, the aim of this study was to test the multiple jeopardy hypothesis for health outcomes at the intersections of age, gender and ethnicity while considering contextual boundary conditions and perceived discrimination as a psychosocial pathway. By doing so, we used a systematic conceptual and analytical approach to identify patterns of multiple effects. Generally, our results confirmed the hypothesis that belonging to (multiple) social minority groups and residing in poorer countries exacerbates adverse health outcomes, which is partially mediated by perceived discrimination. As such, the results are consistent with previous research showing that belonging to a social minority in regard to age and gender is related to lower levels of self-reported health, as well as that there is a detrimental impact of perceived discrimination on people's health (e.g. Levy, 2009). However, there were also some unexpected findings for specific social minority groups.
First, we found that residing in an unfavourable socio-economic context is an additional health risk, but only for women or older individuals. This points to an interesting avenue for future research examining structural intersectionality targeting specific social minority groups, such as women (see also, Homan, 2019). Moreover, old age had generally the largest negative effect estimate on health, which can be partly explained with the processes of biological aging. Furthermore, the main effect of ethnic minority status was only significant when combined with either female gender or older age. In other words, younger males belonging to an ethnic minority group reported the same level of health as did younger males belonging to the ethnic majority group.
Our study aimed to shed light on whether belonging to multiple social minority statuses exacerbates the health risk. Our results show that this is indeed the case for individuals belonging to double social minority groups (older women, older members of an ethnic minority and ethnic minority females). This is informative for policymakers and practitioners when it comes to designing more effective interventions to address health disparities and promote social equity. However, the triple social minority status pointed to an inurement effect: for example, we found that the subjective health of triply jeopardized participants was not as bad as a sum of all detrimental effects of belonging to the three social groups. The country-level results showed that lower levels of socio-economic development had an additional health disadvantage for older individuals and women. The socio-economic development of the country did not matter for the health outcomes of ethnic minorities as well as for the combinations of multiple social minority statuses. One of the reasons could be that ethnic minorities face general challenges, with implications for their health, that are unrelated to the socio-economic context of the country they reside in. For instance, some ethnic minority individuals might be limited in access to health services due to language issues or lack of information. Indeed, there is evidence that prosperous countries are not necessarily more accommodating to ethnic minorities in regard to responding to the needs of the immigrant patients (e.g. through linguistic support) than less prosperous ones (Meeusen and Kern, 2016).
We also found that perceived discrimination was not a great candidate for a psycho-social pathway behind the impact of the (multiple) social minority status on health. The only exceptions were being female (but only among younger and ethnic majority) and belonging to ethnic minority (but only among younger males); their effects were indeed mediated by PD but discrimination experiences themselves, compared to effects of (multiple) social minority statuses, showed weaker associations with health outcomes. This is an important result because it is often assumed that discrimination experiences are one of the main psycho-social pathways that can explain why individuals belonging to social minority groups show lower levels of health (Ferraro and Farmer, 1996). There is some support for this assumption, for instance, Grollman (2014) showed that discrimination experiences partially mediated the effect of social minority statuses on self-reported health. Yet, the weak mediation results suggest that self-reports of discrimination may reflect only a small share of discrimination that can affect health outcomes. Discrimination can occur at different levels (e.g. in terms of systemic discrimination regarding access to health services) and may not even be perceived or construed as a discriminatory experience by its victims but still have detrimental implications for individuals’ health (e.g. Krieger, 2014).
Our results also showed that older people reported less discrimination than younger ones, therefore, the indirect health effects of old age via discrimination experience were counter-intuitively positive. We explain this with the finding that discrimination is related to worse health, yet older adults feel less discriminated against; taken together these two variables create the somewhat counter-intuitive result of a positive indirect effect meaning that the mediating variable PD is transmitting the effect of age to subjective health in a positive direction. Therefore, it seems that older people are somehow immune to discrimination and this is beneficial regarding their health outcomes. But in general, their health is of course worse than the health of younger people.
Our findings also revealed a counter-intuitive indirect effect of old age on health through perceived discrimination. Surprisingly, older individuals reported experiencing less discrimination compared to younger individuals. Yet expectedly perceived discrimination was related to worse health outcomes. When we considered both variables together, the unexpected positive indirect effect emerged. In other words, perceived discrimination as a mediator appears to reduce the negative effect of age to subjective health. This suggests that older individuals may somehow exhibit a certain level of immunity to discrimination, which ultimately benefits their health outcomes. However, this small positive indirect effect was small, and the health of older people is obviously worse than that of younger individuals.
These results may be attributed to a cohort rather than age effect with younger cohorts being more sensitive to perceiving discrimination. Previous research has also found that younger people report the highest levels of age discrimination (Bratt et al., 2020). More research is needed to better understand perceptions of ageism across the life span and more attention should be directed to societal phenomena (e.g. #MeToo) and whether this renders individuals more sensitive to instances of discrimination, which might contribute to cohort differences in perceptions of discrimination.
When interpreting our findings, there are some limitations to consider. First, given the purpose of our study, we could not go into detail about specifics regarding every status and form of discrimination in every country, taking instead a bird eye view of the possible health effects. Consequently, we skipped potentially important aspects. Several other variables may explain why belonging to specific or multiple social minority groups is detrimental for people's health (e.g., access to health care services, social identification, language proficiency, acculturation, indirect discrimination at the individual and institutional levels). Yet, these indicators were not available in the data. In a similar vein, our dataset limited the focus to the three most salient forms of discrimination and to respondents from European countries only. Likewise, we did not examine the many possible individual-level mediators, such as social support, coping styles, social identification, sense of entitlement and personality characteristics. Future research may pay attention to other social groups’ experiences of discrimination, moderator and mediator variables, as well as a larger scope of societies.
Second, we would like to emphasize that this study is correlational by nature and does not imply (although suggests) causal relations regarding discrimination experience. The term ‘effects’ was used in a purely statistical sense with reference to the parameters in the regression models. Nevertheless, many studies have suggested causal mechanisms underlying the influence of discrimination on health using appropriate methods such as longitudinal designs (e.g. Bauer and Scheim, 2019; Pavalko et al., 2003).
Third, as with most major social surveys our outcome variable and experience of discrimination variables were each measured by single items. Yet, it is noteworthy that the ESS Central Coordinating Team initiates extensive pilot tests to ensure that the chosen indicators are reliable and valid. Moreover, Allen et al. (2022) recently argued that single item measures are not necessarily inferior to multi-item measures. Another limitation is that we used respondents’ sex, as assessed by the interviewer, as a variable for gender. While sex is based on biological and physiological characteristics, gender refers to an individual's social identity and the social characteristics and expectations associated with being female or male in a society. We decided to refer to gender instead of sex throughout the paper because the intersectionality framework argues that social identities shape an individual's experiences and opportunities. Moreover, the proportion of people for whom their gender identity does not align with their sex assigned at birth is very small (e.g. estimated to be 0.6% of the adult population in the United States; Flores et al. 2016). Yet, it is important to keep in mind that technically we cannot disentangle the health disparities that might vary as a function of biological differences between men and women or as a function of social norms, expectations and roles.
Finally, we used GDPpc as the sole indicator of the societal context. This variable is highly correlated with several other relevant country characteristics, such as health care expenditure. Hence, it might be that other variables are responsible for moderating the link between disadvantaged social statuses and health. For instance, it could be that it is the availability of better health care services in richer countries that buffer the detrimental health outcomes of belonging to social minority groups (see also our follow-up analyses in the Supplemental materials, Table D). The problem is that more specific variables are often not available for all countries and a small sample of countries does not allow testing many variables simultaneously. Moreover, the reality is likely to be a combination of factors for which the GDPpc (e.g. a better infrastructure to be able to access healthcare services) is generally a fair proxy indicator. Not surprisingly, cross-national studies examining similar hypotheses (e.g. on group conflict theory, Meuleman et al., 2018) also use GDP as a proxy variable to assess unfavourable macro-economic conditions.
To conclude, the results of this study provide new insights into the multiple jeopardy debate by using a systematic conceptual and analytic approach, examining the boundary conditions of the multiple jeopardy hypothesis in considering socio-economic development as an important contextual variable and testing perceived discrimination as a relevant mediating variables for adverse health outcomes. Several conclusions can be drawn from the findings: (1) social minority groups and their combinations cannot be equated with each other in regard to their health outcomes; (2) old age and gender, but not ethnicity, are related to adverse health outcomes, especially in poorer countries; (3) the combination of two social minority groups, but not three, exacerbates each other's harmful impact on health; (4) perceived discrimination can explain some of the (multiple) social minority status-health links; and (5) ethnic minority status shows idiosyncratic associations with PD by fully mediating the link with subjective health.
We hope that this study will stimulate more research to examine the well-being of intersecting social minority groups by using a quantitative psychological approach.
Supplemental Material
sj-docx-1-asj-10.1177_00016993231210650 - Supplemental material for Multiple jeopardy, national wealth and perceived discrimination: Subjective health of intersecting minority groups across 28 countries
Supplemental material, sj-docx-1-asj-10.1177_00016993231210650 for Multiple jeopardy, national wealth and perceived discrimination: Subjective health of intersecting minority groups across 28 countries by Christin-Melanie Vauclair and Maksim Rudnev in Acta Sociologica
Footnotes
Data availability statement
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Fundação para a Ciência e a Tecnologia (grant number IF/00346/2014).
Supplemental material
Supplemental material for this article is available online.
Notes
Author biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.