
Abstract
Monitoring patients who have noncommunicable diseases is a big challenge. These illnesses require a continuous monitoring that leads to high cost for patients’ healthcare. Several solutions proposed reducing the impact of these diseases in terms of economic with respect to quality of services. One of the best solutions is mobile healthcare, where patients do not need to be hospitalized under supervision of caregivers. This paper presents a new hybrid framework based on mobile multimedia cloud that is scalable and efficient and provides cost-effective monitoring solution for noncommunicable disease patient. In order to validate the effectiveness of the framework, we also propose a novel evaluation model based on Analytical Hierarchy Process (AHP), which incorporates some criteria from multiple decision makers in the context of healthcare monitoring applications. Using the proposed evaluation model, we analyzed three possible frameworks (proposed hybrid framework, mobile, and multimedia frameworks) in terms of their applicability in the real healthcare environment.
1. Introduction
Noncommunicable disease is one of the most severe causes for the dramatic increase in the number of dead around the world [1, 2]. Noncommunicable diseases which are also called chronic diseases such as heart disease, stroke, cancer, chronic respiratory diseases, and diabetes, all of which constitute concern not only for developing countries but also even to the first world countries, especially in economic terms where it cost huge amounts of money for patients’ healthcare.
In EU, the number of deaths due to deadly diseases (such as CVD) is accounting for over two millions deaths each year [2]. Moreover, in Southeast Asia, the expenses of Singapore's healthcare providers increase in one year, 2006, by 8.3% compared to 2005. As a report by WHO and WEF as in [1], it said that China alone will have a loss in productivity amounting to staggering 558US$ billion by 2015 due to the impact of these diseases [2]. See Table 1 for other countries.
The loss of national income of different selected countries in billions [1].

Many of the solutions are put in place to reduce the impact of these diseases. For example, they tried to take care of patients who have heart disease through programs that are mostly done in hospitals and health centers under supervision of medical staff [3–7]. Patients, due to limited time or long distance from treatment centers, have led to poor participation of these programs. With the purpose of addressing the aforementioned apprehension, there is an increasing need for continuous monitoring of patient's health. Mobile healthcare is one of the most important solutions that enable constant monitoring and help reduce the expenditures [8].
Mobile healthcare (m-health) provides the bilateral solution: the empowering of the individual monitoring of chronic care and the effective cost of health care services at all economic levels, as the proceedings of the m-health summit at the WEF confirmed [9]. M-health systems can be used for diverse, unobtrusive monitoring types; the chronic diseases monitoring is one of them [5]. Moreover, m-health technologies offer real-time monitoring and detection of changes in health status, support the adoption and maintenance of a healthy lifestyle, provide rapid diagnosis of health conditions, and facilitate the implementation of interventions ranging from promoting patient self-care to providing remote healthcare services [10].
A big challenge is how to enable constant monitoring while the patient is out of the hospital/clinic and practicing his daily living activities at/in his own environment. In addition, how can we facilitate low-cost small devices for continuous 24 hours a day and any-place health, mental, and activity status monitoring. We can summarize our contribution in the following.
We proposed a solution that utilized the benefits of cloud computing, mobile health applications, wireless body sensors, and media healthcare services in one hybrid framework. Users anywhere and from any device, at any time, could access their services and applications. Our framework can facilitate effective processing of complicated multimedia services and applications from anywhere, at any time, and on any device. Multimedia services and applications enable doctors and other healthcare professionals to have fast access to m-health information for effective decision making along with well cure. Patients multimedia information (such as video, images, and text) that are monitored will be sent through mobile devices (such as smart phone and wearable sensor) to the cloud in order to be processed and formed to be ready in use by another party (i.e., doctors, therapists, caregivers, or other patients) to make a decision or to share this information.
We proposed a novel evaluation model based on Analytical Hierarchy Process called Cost-effective, Health support, Operational and Functionality (CHOF). This model helps evaluating any system/framework/tool that monitors patients with a chronic illness. This model consists of four main criteria and fifteen subcriteria.
We analyzed three possible frameworks (proposed hybrid framework, mobile, and multimedia frameworks) in terms of their applicability in the real healthcare environment.
The remainder of this paper is organized as follows. Section 2 describes related work; then Section 3 presents our proposed model in details. Section 4 shows the evaluation process, which represents analysis and results, and finally concluding remarks are made in Section 5.
2. Literature Review
There has been a lot of research on mobile healthcare and remote monitoring in the past decade. They emphasized that constant patient monitoring has led to 50% drop in hospitalizations, 73% reduction in emergency room visits, and 51% reduction in patient cost. Also, it provides decreased cost, higher revenues, and ability to take on higher caseloads for caregiver [11].
Since our framework consists of three parts (the multimedia services in healthcare, cloud computing for healthcare, and mobile healthcare), this section will try to study the literature from three points of view.
2.1. Multimedia Services in Healthcare
Multimedia is a complex collection of elements changing overtime such as motion graphics animated type, 3D generated elements, video, and sound, combined all together and distributed in a sort of interactive mechanism. Nowadays, multimedia services in m-health are getting a great deal of attention since medicine is a very visual field; the structure and function of the human body, how the diseases are caused, how body react to disease, how a particular drug works, and how a procedure should be done can best be explained through media. Media files can be streamed seamlessly through internet, intranet, and related technologies [12].
Many researches prove that multimedia play an important role in e-health services, especially in educational software. Multimedia improves the way of designing and implementing the educational materials to make it easy for learners to understand information in an interactive environment. It would be a far more effective educational method to use an image or an animation along with the textual description of a biomedical image or the textual description of a clinical action [13]. Authors in [14] eliminated the need the 20-minute trips previously required to manually transport radiology images, test results, and other medical information. Besides, wireless web cameras installed at the remote site allowed medical staff in the field to run real-time video consultations and patient reviews with their colleagues in the hospital. They demonstrate the transmission of medical data over a standard network, with no effort to tailor the characteristics of the transmission system to the specificity of the transmitted data. In [15] authors exploit personalized healthcare information for elderly to learn and improve their healthcare knowledge. The provision of multilingual video clips of stroke-precaution knowledge could help those elderly conquer the reading comprehension as well as the illiterate problems.
2.2. Cloud Computing in Healthcare
The term cloud computing refers to computer resources that are available on demand through which computing infrastructure, applications, and business processes can be delivered to users as a service wherever and whenever they need. With the advent of cloud computing, the long-held dream of computing as a utility has become true [16, 17]. We can equate cloud computing to the source of electricity and gas so customers are only charged based on the usage of the provided services and resources. Everything has rolled up in predictable monthly subscription; thus one only pays for what he uses [17, 18]. With respect to the m-health domain, many previous studies identified the future of cloud computing and offered various frameworks to enhance healthcare service [18–21].
In [22] authors proposed a cloud-based system to computerize the approach of gathering patients’ crucial information through a system of sensors linked with legacy medical devices and to convey the information to the cloud of the medical center for storage, manipulating, and delivery. The major prosperities of the system are that it gives clients 7-day-a-week continuous information gathering, wipes out manual work, and is free of errors.
In [23] authors described a cloud computing protocol management system that provides multimedia sensor signal processing and security as a service to mobile devices. The system has relieved mobile devices from executing heavier multimedia and security algorithms in delivering mobile health services. This will improve the utilization of the ubiquitous mobile device for societal services and promote health service delivery to marginalized rural communities.
Authors in [24] identified a pervasive cloud initiative called Dhatri, which leveraged the power of cloud computing and wireless technologies to facilitate physicians to access patient health information at anytime from anywhere. In [25] authors described a cloud-based prototype emergency medical system that can be accessed by Android-enabled mobile devices. They integrate the emergency system with personal health record systems to provide physicians with easy and immediate access to patient data from anywhere and via almost any computing device while containing costs.
2.3. Mobile Healthcare
In the recent two decades, there has been a relentless decrease in the amount of patients getting treated in doctor's facilities because of the impact of mobile healthcare. Long-term monitoring of patients’ physical, cognitive, behavioral process is vitally important for those with chronic diseases. WHO defined m-health as “medical and public health practice supported by mobile devices, such as mobile phones, patient monitoring devices, personal digital assistants, and other wireless devices” [26]. An overview of health monitoring architecture with a smart phone was introduced in [27] which has links to external wireless sensor devices, such as a blood pressure monitor and weight scale, to collect periodically health data. These external devices have sensors, which are Bluetooth-enabled. The smart phones running healthcare apps monitor the wellbeing of the patient and transmit the data to the healthcare data server maintained by the hospital via the internet [3].
A mobile embedded with sensors using different information about the monitored person like position and temperature, to do a precise analysis in a cloud [5]. The medical personnel access the data server via a secure internet connection to monitor the patient's health remotely. Some of existing systems are mostly stand-alone and are not yet integrated with existing electronic health systems, which could critically limit their large scale employment [1, 2, 9].
Authors in [28] designed and developed a new Home Monitoring System with full functions, small device, low power consumption, low cost, and easiness to use based on distributed database storage. Only few systems can deal with multiple devices. All the examined systems connect to a remote server to store the patient data; none supported distributed data storage. Many m-healthcare systems have some limitation (closed systems, does not provide clinical data integration services that may come from different sources when it requires more than a professional).
In [29] authors tried to propose a new m-healthcare system based on SOA called SOAMOH that enables the integration of the clinical data, supporting HL7, and helps people to attain healthcare service whenever and wherever they are, using their mobile devices that are connected to wireless networks. However, they did not implement or test this system.
In [4] they made a system to measure and record heart rate of patients using software tools on a mobile phone platform. This allows patients to do a home-based cardiac rehabilitation exercise program using a mobile application called TuneWalk. Two of the authors had participated as test subjects in the evaluation. TuneWalk recorded the heart rate variability and activity data that was measured by WBA. TuneWalk's MET estimation with the test subjects was found to be fairly accurate at walking speeds. However, when the subjects ran the results become unreliable. This should not present a major problem, since in the proposed home-based CR program exercises subjects are required to walk and not run. The authors in [6] introduced a mobile healthcare-based heart failure monitoring architecture. The framework consists of various sensors to measure physical quantities; processors to process those quantities and smartphones acting as a hub, to deliver these data to appropriate users or caregivers.
Authors of [8] proposed a predicative and preventive device that is capable of predicting heart rate abnormality, and possibly tachycardia, in advance by using an advanced prediction model to estimate the heart rates of selected patients. This is done by sending alerts to the medical professionals for appropriate action to be taken when the estimated heart rates exceed a certain threshold.
In [9] they proposed architecture to integrate the data of personal health monitoring systems within an electronic health care network using extending the traditional Service Oriented Architecture (SOA) approach to business-to-business networks with support for processing the complex event and realizing the context.
In [30] the developers have proposed wearable blood pressure sensors which monitors patients’ health and allow effective treatment of hypertension at home or in out-of-hospital environments.
Author in [10] introduces a novel architecture called HERA project which aims to build an AAL system to provide low-cost services to improve the quality of life for the elderly that suffer from the early stages of the Alzheimer disease and/or other diseases (i.e., diabetes or cardiovascular problems). The HERA system developers have a complete methodology and architecture and have planned the evaluation process. However, they are yet to implement their plans. Therefore, there are currently no results to see whether the system actually works. Some of the researches discussed this issue from the hardware view.
Work in [28] presents a handoff protocol that can be readily implemented by Wireless Body Area Sensor Networks (WBASNs) coordinators and APs when the RSS of the former falls below acceptable levels. For this, they promote employing multiple radio channels in order to leverage the system's capacity, which allows monitoring multiple users in a deployment setting with several rooms. They tried to build a reliable and efficient health monitoring application based on WBASN and using their protocol that enables continuous monitoring of ambulatory patients at home. The processing in [28] was conducted on an offline data collected via Bluetooth from a small size wearable electrocardiograph (ECG) device since processing an online and real-time data is difficult [21, 31]. This issue was addressed in [31] using a software framework for body sensor network (BSN) called SPINE (signal processing in-node environment). This software enables emulation of a set of nodes forming a WBSN and requires a data set for each node.
Different healthcare systems are introduced in the literature [3–20, 22–27, 30, 32–37]. Despite considerable progress in health monitoring research over the last decade, today's health-monitoring systems are not fully capable of monitoring noncommunicable diseases patients while doing their daily living activities. In most of the systems, a patient or a user is restricted to his/her room or home or to an area within the range of installed wireless body sensor network [11–27, 31, 33–37]. If the user goes outside this range, monitoring device fails to relay recorded information to the gateway device and, as a result, some information is lost. In addition, many old systems use PCs or some other hardware as a gateway platform, which again limits the mobility. Moreover, an important service less discussed in most of the related studies is patient's ability to view his/her medical data trends anywhere and anytime with minimum additional hardware requirements.
3. Proposed Work
The proposed work presented in this paper consists of two dimensions: firstly, to unify the aforementioned concepts in one framework, as a solution of real-time monitoring for noncommunicable diseases patient; secondly, an evaluation model that helps appraise the proposed framework and other various alternatives of similar solutions and frameworks.
3.1. Cloud-Based Multimedia Framework
The proposed framework is shown in Figure 1; it depicts the system architecture of cloud-based multimedia framework healthcare. The media cloud computing physically separates the user interface from the media application logic. The user device (e.g., smart phone, laptop, IP camera/webcam connected to PC, etc.) executes only a viewer component (e.g., a web browser or mobile application) operating as a remote display for the m-health media services and applications running on distant servers in the cloud.

The architecture of the proposed model.
The multimedia cloud providers deploy powerful cloud virtual machine resources such as the CPU, memory, GPU, and network bandwidth on demand, while utilities first process and manage heterogeneous m-health multimedia requests and then deliver computing results or m-health media data to the users. By employing a multimedia cloud service, mobile users do not need to pay for costly computing devices. Instead, they can pay for the utilized resources based on time.
As shown in Figure 1, the users (e.g., patients, doctors, caregivers, etc.) can obtain different m-health media services from cloud media server. We do not need a traditional media streaming server for progressive download or for HTTP-based adaptive streaming technologies such as Apple HTTP Live Streaming (HLS) or Microsoft Smooth Streaming. We actually need a media server to stream live or on-demand media and to run a streaming server. Streaming servers are necessary if the client wants to protect their streams with encryption, deliver data via peer-to-peer or multicast, or serve multiple targets.
There are three basic options: the Adobe Flash Media Server line of products, Microsoft's IIS Media Services, and Wowza Media Server. There is also an open-source streaming server called Red5 that uses some secure protocols for data streaming to Flash, but it does not currently convert streams for delivery to iOS or support any adaptive streaming technology. The cloud media server will introduce many media services, such as media storage service, transcoding service, analysis and sharing service, and streaming service, and request for their different compositions through a web browser or mobile application interface. The users’ composite service requirements are then sent to the cloud system manager, which finds out the suitable configuration of VM resources that are based on SLA.
The resource allocation manager then allocates the VM resources to a set of physical machines to run the mobile media service tasks. The mobile media service tasks outputs (i.e., display updates, composition results, etc.) are finally transmitted to the user through the web browser or mobile application. After the media applications or services are started, the system monitoring and metering function tracks the VM resource usages that are attributed to users. It can also notify the resource and system managers for a quick response and the resource configuration to assure that the correct VM resources are distributed to suitable mobile users. Therefore, in order to correctly allocate resources and to deploy VM images, an efficient, cost-effective, and optimal VM resource allocation algorithm is necessary for a resource manager.
3.2. Evaluation Model
The proposed framework in previous section provides three different possible implementations: mobile, multimedia, and hybrid solutions.
Mobile systems are those systems which use the smart phone healthcare applications (apps) to monitor healthcare either by using standalone applications or by applications connecting to wearable sensors and working as a gateway of body sensor network (BSN) [30]. This solution may have data limited to text and set of biosensors signals.
Multimedia systems in m-health monitoring are those systems which provide services contains elements changing overtime such as motion graphics animated type, 3D generated elements, video, and sound. Many tools such as IP and web cameras and applications such as Voice over IP (VoIP) and streaming audio and video are used in multimedia health services by using wireless architecture [14].
The hybrid systems are those which benefit from the two other systems together, mobile and multimedia in a unique system.
Here we will study the three solutions to find the best one among them to be selected. We will compare the three systems based on different criteria and based on Analytical Hierarchy Process (AHP) [38]. The first step is the preparation of an evaluation task which considers user needs, assumptions, and constraints relevant to the three solutions. The second step is to identify and select the evaluation criteria, with respect to these solutions. In this respect, we build four main criteria and fifteen subcriteria, as illustrated in Figure 2. The description of each criterion is shown in Table 4.
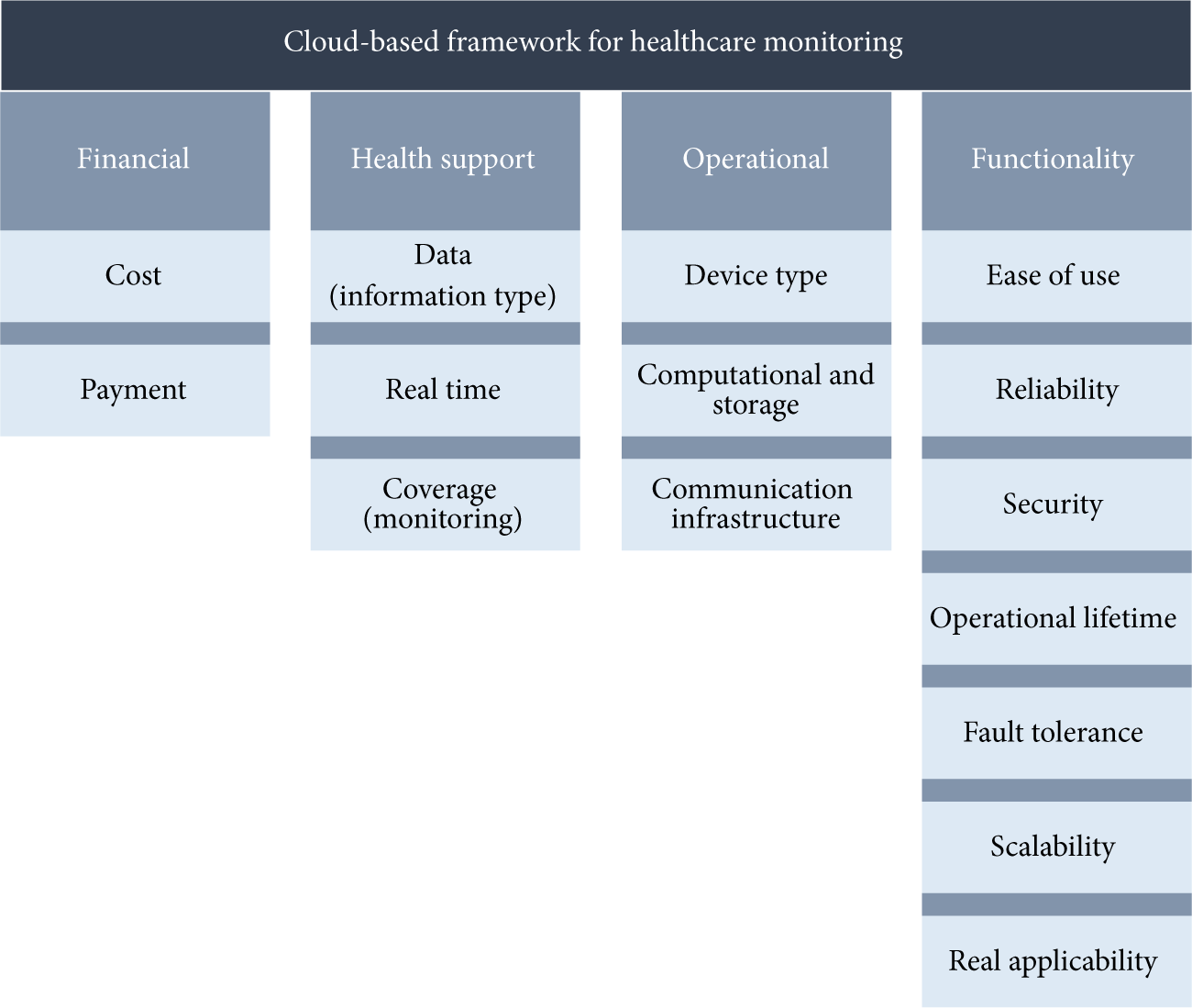
Evaluation criteria regarding the three solutions.
We used multicriteria decision making (MCDM) techniques. Number of MCDM techniques can be applied to our selection problem; however, here we used AHP. Moreover a number of additional features working in favor of selecting AHP for the selection process have also been considered. AHP is appropriate technique to use, when limited number of alternatives needs to be evaluated.
3.3. Analytical Hierarchy Process (AHP)
The Analytical Hierarchy Process (AHP) is an MCDM technique, developed by Saaty [38]. AHP decomposes a complex MCDM problem into a hierarchy. It generally consists of selecting a goal, listing criteria, listing sub-criteria, determining the alternatives, building hierarchy, assigning priorities, calculating weights, checking consistency, getting results, and making final decision. AHP technique has been implemented according to the following steps.
(1) Modeling the Problem. AHP decomposes a complex MCDM problem into a hierarchy model as shown in Figure 3, with the goal (evaluating and selecting suitable solutions for cloud-based framework) at the top, the alternatives (Mobile, Multimedia, Hybrid) at the bottom, and the criteria (Cost-effective, Health support, Operational and functionality) and subcriteria (cost-provider-side, cost-consumer-side, information type, real time, coverage, etc.) in the middle.
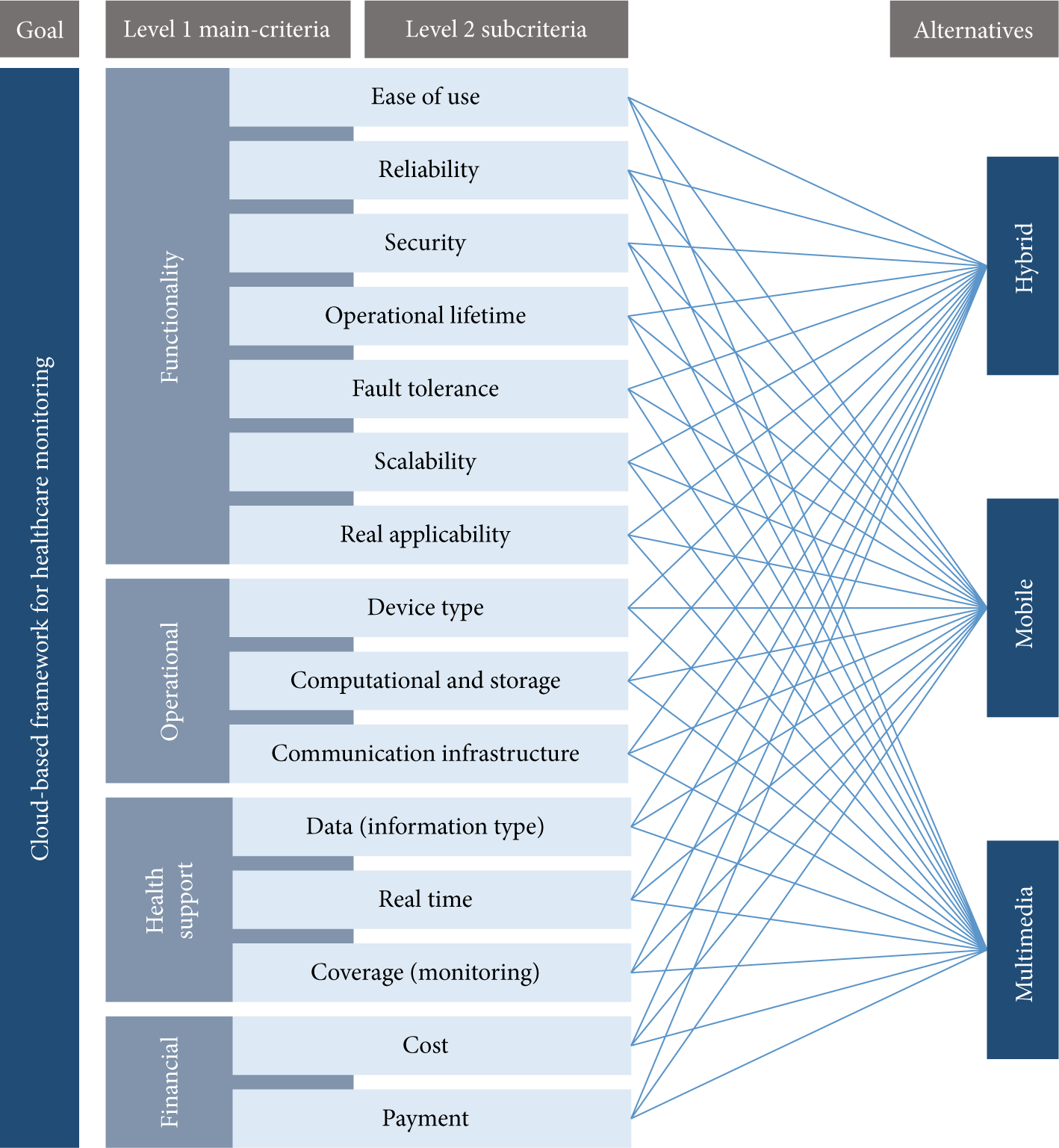
Hierarchy model for selecting the best solution.
(2) Applying Pair-Wise Comparison between Children of Each Level of the Hierarchy. This comparison generates a matrix of relative rankings for each level. This matrix is also called “judgment matrix.” The matrix satisfies the relation
The order of the matrix is dependent on the number of elements at its connected lower level. The pair-wise comparison is conducted based on Saaty scale described in Table 2 [38].
Saaty's scale for pair-wise comparisons.

(3) Computing Eigenvector. Once pair-wise comparison is performed, eigenvectors are computed. The eigenvector is computed by dividing each element of the matrix by the sum of its column elements. It may be mentioned that the eigenvectors represent the relative weights among the alternatives (mobile, multimedia, and hybrid).
(4) Computing Consistency Index (CI). Consistency index of matrix order n (the size of the matrix) is computed using the following, where

(5) Computing Consistency Ratio (CR). Consistency ratio is computed using (3). The consistency ratio compares the consistency index with the random consistency index (RI). As shown in Table 3, RI is generated from a sample size of 500 matrices:

If the value of consistency ratio is smaller than or equal to 10%, the inconsistency is acceptable. For n = 3, the threshold is set to 0.05 and, for n = 4, it is set to 0.08. For n ≥ 5, if the consistency ratio (CR) is greater than 10%, the judgment needs to be revised [38].
Random index values for matrices of different orders.

The description of the criteria of CHOF model.

(6) Computing Final Ranking. The final ranking is calculated by using the following:

where n is the number of criteria and m is the number of alternatives. The alternative with the highest priority value is considered as the most suitable solution for a decision problem of selection, while the alternative with the lowest priority value is the least appropriate for the given decision problem.
4. Analysis and Results
We attempted to apply AHP technique selecting one of the three solutions that we investigate in this research. We described the analysis through AHP.
As shown in Figure 3, the hierarchy model for the criteria of selecting cloud-based solutions consists of 4 levels. Level 0 is the goal of the problem, “selecting the best solution.”
Level 1 consists of 4 main criteria such as Cost-effective, Health support, Operational and functionality. Level 2 contains the subcriteria and the last level is the alternative solutions. The solutions are evaluated according to a reference model developed by Olla, Phillip, and Joseph Tan [36] in order to extract requirements, and then we used questionnaires to measure the relative importance of each criterion.
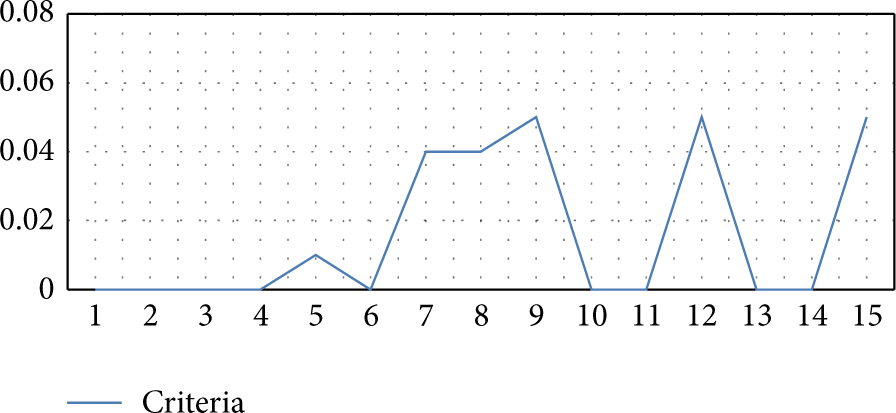
Figure 4 shows the ranking of cloud-based proposed solutions based on each subcriterion. As can be seen from the figure, the relative importance of each subcriterion in the solutions is shown by dots positions. For example, we notice that real-time required criterion has the highest value (RT > 0.15) which means that it is the most important criterion in hybrid solution followed by the coverage monitoring (CM) criterion and so on.
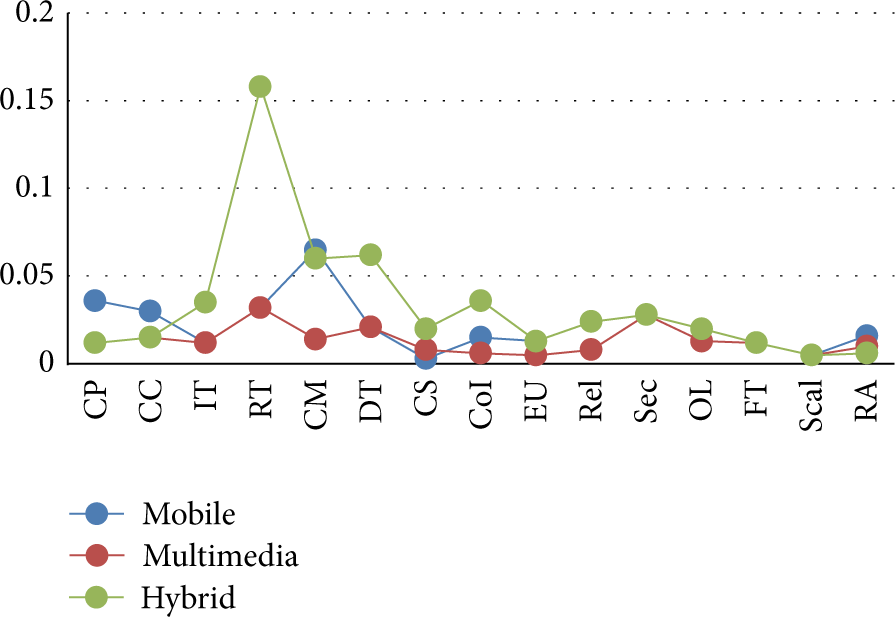
Ranking of cloud-based solutions based on subcriteria.
As shown in Table 5, the final ranking of the alternatives are as follows. Hybrid solution (50.4%) is the most preferable cloud-based framework for monitoring noncommunicable diseases, followed by the cloud-based mobile framework, with a priority vector of (29.5%). The cloud-based multimedia framework gets the third place with priority vector of (20%). The table also shows the relative importance of the main criteria and the subcriteria. The health support criterion is the most important one, which has the weight of 41.8%. The less important is the cost-effective factor (12%). In terms of subcriteria, we deal with global weights. In this regard, the most important criterion is the real-time (RT) with global weight equal to (22.1%) followed by coverage monitoring CM subcriteria (13.9%) and device type DT (9%). The last criterion is the scalability with relative importance equal to 1.5%.
Final ranking of alternatives with respect to the main and sub-criteria.
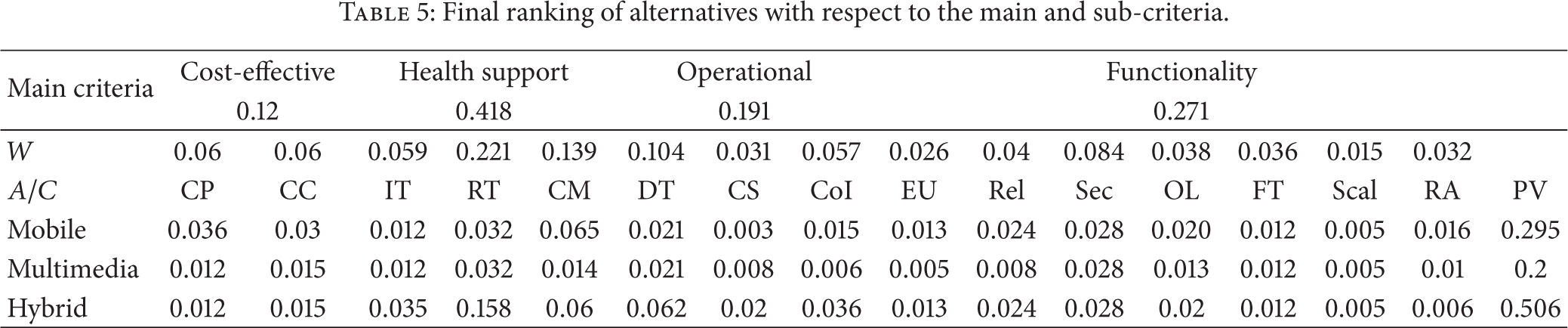
Figure 5 shows the ranking of the cloud-based solutions based on the main criteria. The priority vector for each tool is represented by the cyan bar. As can be noticed from the figure, the hybrid solution is the most suitable framework since it has the highest priority vector. The figure also shows the strength and weakness of each solution, which are based on the four main criteria. For example, the strength of the hybrid solution lies in the health support factor, as hybrid solution got the highest rank in the health support criterion which is 25.2 while this solution got the lowest rank in the cost-effective criterion which is 2.7.
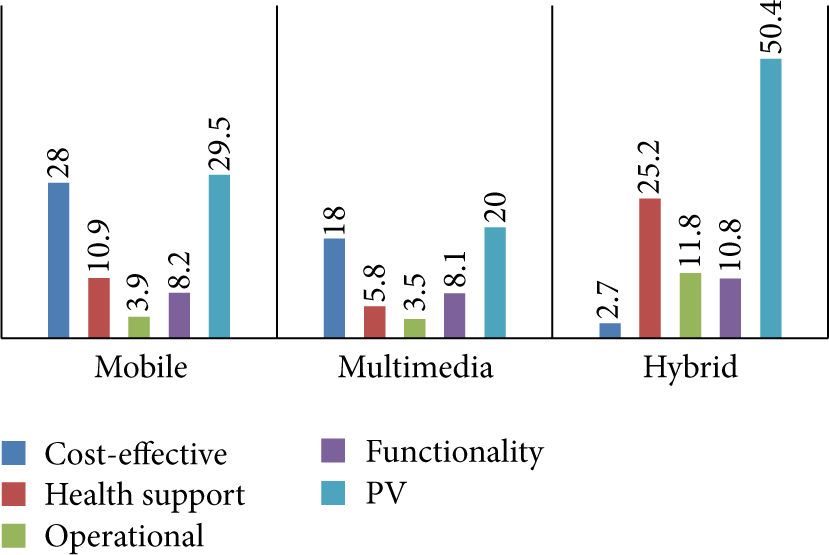
Ranking of cloud-based solutions based on main criteria.
We use ExpertChoice to calculate the final priority and check the consistency. Figure 6 shows the consistency ratio (CR) for the matrix of relative ranking at alternatives level, with respect to fifteen criteria. As the consistency ratios for the criteria and alternative judgment matrices are less than 6 percent, the response related to relative importance for each criterion from the participants is consistent. As can be seen from Table 6 and Figure 6, the hybrid solution is the appropriate one to select for building a cloud-based healthcare services framework to monitor noncommunicable diseases patient, as it gets highest ranking.
Overall ranking comparison AHP.

Consistency analysis.
5. Conclusions
For the period of the research and from the technological point of view, we realize that hybrid (mobile and multimedia) healthcare and cloud computing are such a natural fit for the monitoring patients with chronic diseases. The great benefit of using cloud computing to introduce media services is observable and need to be applied. We discussed some key concepts about what have been developed in the domain of healthcare monitoring using cloud computing and media services. In this paper, our primary focus is, firstly, to develop an architectural framework facilitate the process of getting healthcare services over cloud platform, efficiently and, secondly, to develop a new evaluation model to appraise and select the best solution depending on one of the most famous multicriteria decision making methods (MCDM), the so-called Analytical Hierarchy Process (AHP).
We analyze our proposed model in terms of three possible frameworks and find by results that the best alternative is hybrid framework which consists of both mobile and multimedia. The evaluation results attained from the MCDM technique showed the most appropriate framework that can be used for building healthcare monitoring system. It has been observed that AHP has potential method to solve the selection problem. Our plan in the future is as follows:
implementing a prototype of cloud-centric healthcare system application;
evaluating the performance of the proposed framework in terms of QoS guarantee and cost effectiveness.
Footnotes
Conflict of Interests
The authors declare that there is no conflict of interests regarding the publication of this paper.
Acknowledgment
The project was supported by King Saud University, Deanship of Scientific Research, Research Chair of Pervasive and Mobile Computing.