
Abstract
A dynamic heterogeneous and multihop (DHMH) wireless health monitoring system (WHMS) as a three-tier semi-self-organizing health monitoring network was presented. From bottom to top, the first tire of the network is the mobile data acquisition layer (DAL), the second tire of the network is the data transporting layer (DTL), and the third tire of the network is the data collection layer (DCL). A RF power control based topology management mechanism is proposed to balance the network load and to improve the network throughput. A lightweight hierarchical routing protocol (LHRP) was designed to reduce the transmission delay and improve the network throughput. For the mobile DAL nodes, the seamless mobile access mechanism (SMAM) was designed to ensure the low packet loss ratio. To evaluate the network performance, the end-to-end delay, the averaged reception ratio, and the network throughput of the DHMH were tested and the results proved that the network performance of the DHMH was improved.
1. Introduction
Long-term and continuous health monitoring of people is increasingly popular as there are more and more aging people and subhealth persons. Motivated by the above requirement and promoted by the development of the wireless communication technology, the MEMS sensor technique, and the integrated circuit technology, wireless health monitoring system (WHMS) is advent and fast developed. In this paper, we designed a semi-self-organizing, dynamic, heterogeneous, and multihop (DHMH) WHMS for indoor healthcare aimed at monitoring the aging in the nursing homes and the white collar workers in the office buildings. By the referred “semi-self-organizing” we mean that the nodes in the DTL are non-self-organizing while the various kinds of HMNs in the DAL are self-organizing. The stationary DTL of the network makes the health monitoring system much more stable, while the mobility of the HMNs could enable the people being monitored to live normal lives without losing freedom.
Wireless communication standards used in the WHMS are many, such as Bluetooth, WiFi, ZigBee; Bluetooth is a common used technology for it is easy to connect with the-state-of-the-art Bluetooth devices such as mobile phone. However, Bluetooth is peer-to-peer communication and unable to format large scale networks. Though WiFi has a large coverage, the cost to build a WiFi network is comparatively high. ZigBee is a networking standard sponsored by the ZigBee Alliance and developed for low-data-rate, low-cost, and low-power-consumption wireless communication [1]. As health monitoring devices used in the WHMS are often featured with small size and resource limited, ZigBee is more suitable for the design of DHMH.
The advantages of the system proposed in this study can be summarized as follows. (1) According to the specific functions of the devices in the DHMH, three different types of devices were designed to carry out data acquisition, data transmission, and data collection, respectively. (2) The fixed network backbone made of the DTL nodes makes the system more stable and reliable in data transmission. (3) The end-to-end delay of the system is reduced by the lightweight hierarchical routing protocol (LHRP) that was specially designed for DHMH. (4) The seamless mobile access mechanism (SMAM) proposed in our system enables the HMNs to move freely with a much smaller packet loss ratio.
2. Related Work
Nowadays, many studies on WHMSs have been conducted. Guo et al. present a fundus image analysis based computer aided system for automatic classification and grading of cataract, which provides great potentials to reduce the burden of well-experienced ophthalmologists and help cataract patients in underdeveloped areas to know timely their cataract conditions and obtain treatment suggestions from doctors [2].
Oresko et al. designed a smart phone based cardiovascular disease monitoring and assistive diagnosis platform [3]. The authors united the portability of Holter monitors and the real-time processing capability of state-of-the-art resting ECG machines to provide an assistive diagnosis solution using smart phones. However, the smart phone based platform they designed is a single user monitoring system, which cannot be scaled up easily.
ColdBlue described in [4] is an indoor healthcare platform aimed at monitoring the patients in hospital. It uses the commercially available health monitoring nodes and is based on the “flat” network, in which all the nodes except the coordinator perform the same function, without special router nodes to relay data. Since there are no specialized router nodes to relay data, the data transmission performance decreased with the increase of the health monitoring nodes. Besides, the ColdBlue does not use the end-to-end delay of data transmission which is a critical problem for practical applications. Besides, to improve the reliability of the data transmission, redundant transmissions and coding techniques are adopted by ColdBlue, resulting in the valuable bandwidth waste.
In MEDiSN [5], the authors designed a two-tire network architecture including the network backbone and the mobile physiological monitors. For the routing protocol, the traditional collecting tree protocol (CTP) was used for the backbone layer of the MEDiSN. Although some adjustments were made to the CTP to improve the network throughput and the data transmission reliability, the computation complexity of the protocol was increased dramatically. Besides, to buffer various kinds of data, the nodes in MEDiSN needed to have relatively large storage capacities. Experiments on the average reception ratio and the PM's energy consumption were conducted in detail. In addition, the MEDiSN did not consider the transmission delay which in some critical moments may cost human lives.
Mercury [6] is a wearable, wireless sensor platform for motion analysis of patients being treated for neuromotor disorders, such as Parkinson's disease, epilepsy, and stroke. In contrast to previous systems intended for short-term use in a laboratory, Mercury was designed to support long-term, longitudinal data collection on patients in hospital and home settings where the core challenges of long battery lifetime and high data fidelity for long-term studies were addressed. This requires the optimization of sensor operation and data transmission.
Reliable clinical monitoring using wireless sensor networks designed in [7] introduced the hardware design and the network architecture of the system, where the longtime reliability of the system was tested in a hospital located in the downtown area. The authors pointed that the unreliability of the system is mainly caused by the malfunction of the HMNs, which is consistent with our results.
Medical Ad Hoc Sensor Network (MASN) [8] is a platform to perform real-time collection of healthcare data. The system has the capability of localization and ECG monitoring of the patients with cardiac disease. The implemented communication protocol is based on a cluster organization, where patients carrying ECG sensors are grouped in clusters, and the information from cluster nodes is aggregated and relayed to the ECG server.
The activity of daily life monitoring of the elderly is a popular field of research. The ViCare proposed by Hossain and Ahmed in [9], the Alarm-Net proposed by Wood et al. in [10], and SATIRE introduced by Ganti et al. in [11] are wireless sensor networks used for assisted-living and residential monitoring. Networks for these applications are generally deployed in one room and less data need to be transmitted, so they are featured with small coverage and low transmitted data rate.
Authors in [12, 13] presented the outdoor WHMSs for massive emergency situations where the rapid and robust ad hoc deployment networks were needed due to limited resources and emergent conditions.
Compared with the previous studies mentioned above, the system proposed in this study adopted the three-tier network architecture. Since the previously developed network protocols are very complex and need large memorization sizes, in this study, a light hierarchical routing protocol (LHRP) and a seamless mobile access mechanism (SMAM) were developed to reduce the end-to-end delay and the packet loss ratio of data transmission.
3. Hardware Design
The designed DHMH consists of three types of devices: the coordinator node (CN), the router nodes (RNs), and various kinds of health monitoring nodes (HMNs) (see Figure 1). The hardware of these three types of devices was designed based on the specific functions the nodes played in the network and the hardware design of these nodes was introduced.
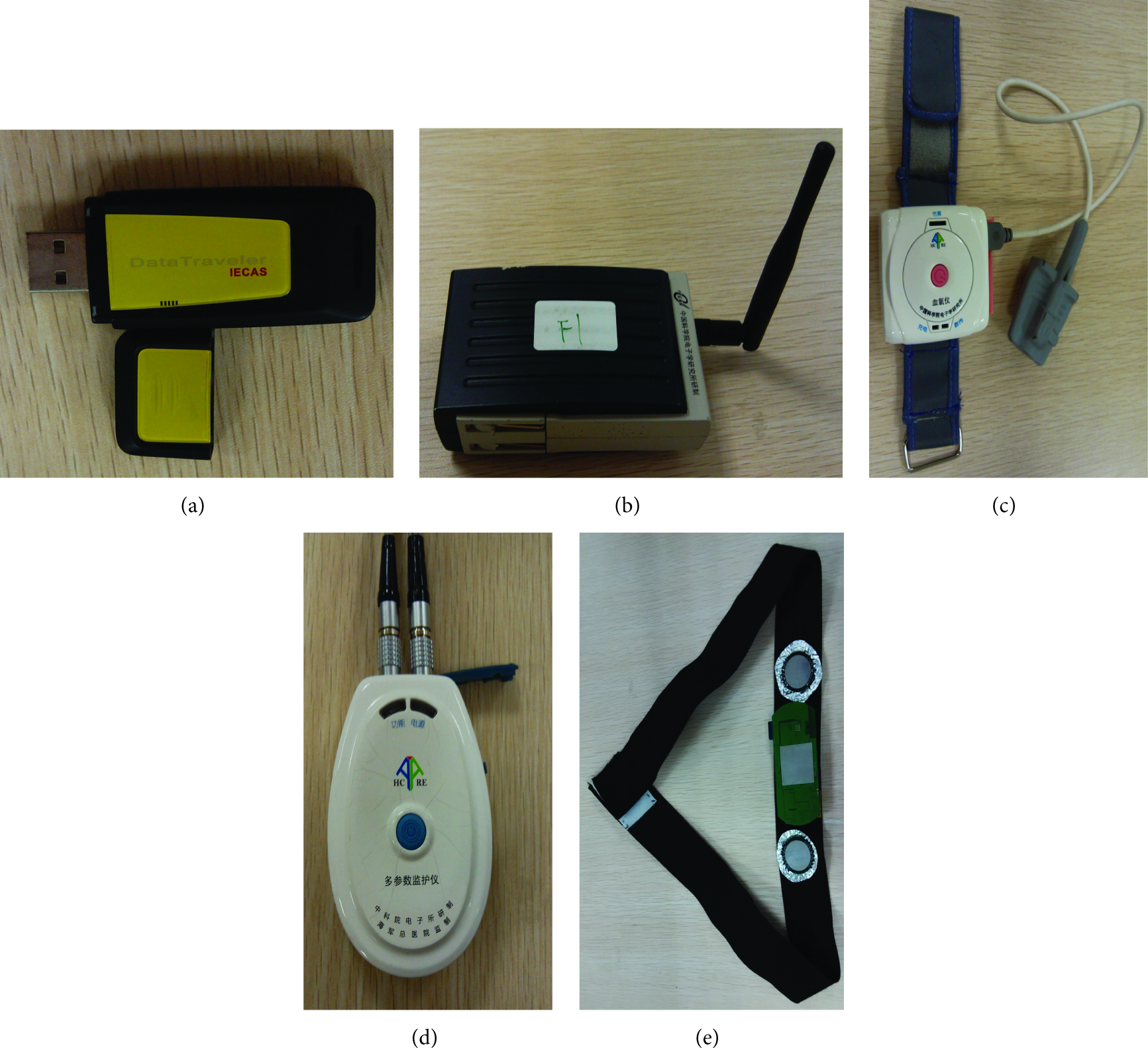
The picture of the nodes designed for the system. (a) A CN with USB interface. (b) A RN with P-H-T sensing. (c) A wrist worn SpO2 monitoring device. (d) An integrated ECG, SpO2, respiration rate monitoring device. (e) A noncontact ECG monitoring belt.
The CN is a small size wireless data collector with a USB interface (see Figure 1(a)). The CN is connected with a computer through the USB interface where the computer then sends the collected data to the medical center through the internet.
The RN was developed as shown in Figure 1(b) to specially relay different kinds of physiological signals for the healthcare networks. The adaptive RF power adjustment mechanism designed in the RN enables the power control based network topology management. Moreover, the atmospheric pressure, humidity, and temperature (P-H-T) sensors were integrated in the RN which not only provides the environment information to the supervisor for disease diagnosis but also functions as a reminder to people being monitored for more healthcare practices. Besides, the RN designed in this study can be powered by three modes: Li battery, 220 V civil electricity, and USB power. For daily use, the RN can be plugged in the power supply flapper. In case of accidental civil electricity power failure, it can automatically switch to the lithium battery power. In addition, the USB power interface enables the router to be powered or charged by large-capacity mobile power sources. As a result, this multipowered mode could guarantee that the router can work in a continuous and reliable mode. The hardware design of the RN has been described in detail in [14].
Health monitoring nodes are responsible for collecting various kinds of important physiological parameters of human beings. The hardware of health monitoring nodes generally includes a sensing module, a signal processing module, a microprocessor module, a data storage module, a wireless transceiver module, and a power management module. The key components of the sensor module are ECG electrodes (dry electrodes [15, 16], Ag/AgCl electrodes), blood oxygen probes (reflection type and transmission type), or temperature sensors. The signal processing module includes the signal amplification, filtering, and A/D conversion and the micro controller module is responsible for the coordination and control of all the modules. The wireless communication module includes ZigBee communication and Bluetooth communication and memory for data storage. Figures 1(c), 1(d), and 1(e) present various kinds of HMNs designed in this study such as an integrated ECG, SpO2, and respiration rate monitoring device, a noncontact ECG monitoring belt, and a wrist worn SpO2 monitoring device. Figure 2 shows the physiological information sampled by the HMNs designed in our library.
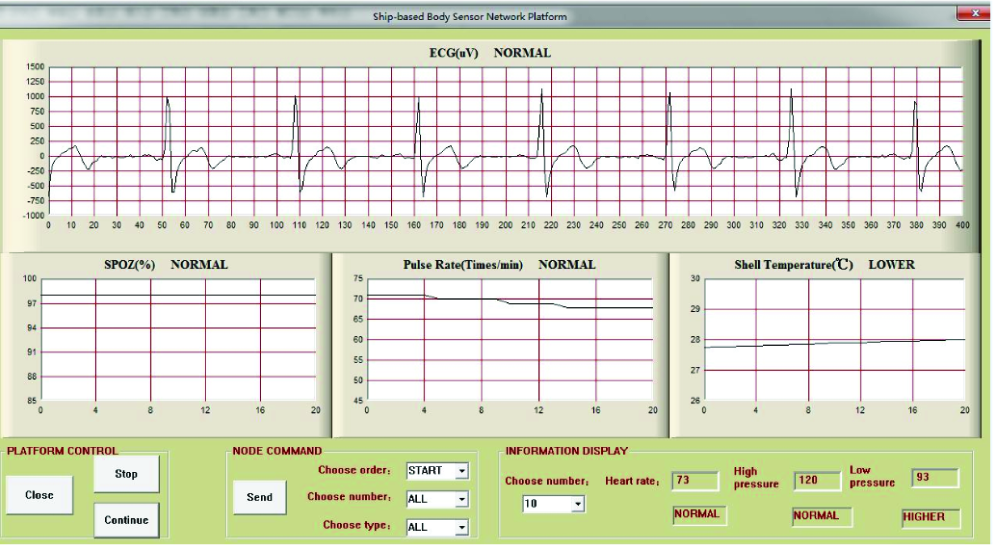
Windows based health monitoring interface.
4. Network Topology
The DHMH is a three-tier semi-self-organizing health monitoring network. The architecture of the DHMH is shown in Figure 3. From bottom to top, the first tire of the network is the mobile data acquisition layer (DAL), which consists of various kinds of wearable health monitoring nodes (HMNs) to sample the physiological signal of the people being monitored. The second tire of the network is the data transporting layer, which is formed by the specially designed router nodes and composed of the main routing path of data transmission. The third tire of the network is the data collecting layer (DCL), which is formed by the coordinator node (CN), which is connected to a personal computer to enable data collection and remote transmission to the backend sever. The DTL and the DCL nodes are the backbone of the network, and the deployments of DTL and DCL nodes are stationary and well-designed according to the indoor wireless signal propagation attenuation through different obstacles. People wearing the HMNs have the freedom to walk arbitrarily in the coverage of the network without the physiological data loss. For DTL, the RNs join the network through the assigned parent nodes and the network topology is optimized according to the practical application scenario. After the construction of the network backbone, the HMNs choose the RN/CN with the best LQI to join the network based on the active channel scanning. The functionality division between acquiring and relaying data enables the HMNs to work with a low duty cycle to save energy, while allowing the RNs to provide reliable data transmission.

The architecture of the indoor WHMS.
4.1. Network Formation
The network was constructed from top to bottom according to the following 5 steps. Step 1: according to the application scenario, choose the proper location for the CN where the center of the monitored area is preferred. Step 2: according to the RF power of the RNs and the obstacles in the practical application scenarios, optimally deploy the RNs in the building. Step 3: according to the specific physical location of the RNs and CN, design the optimized routing paths, and according to the parent-child relationship, we preconfigured the CN and each RN with the addresses of all its direct children RNs to the flash. Step 4: initiate a network by the CN and then join the RNs into the network through the assigned parents. Step 5: join the HMNs into the network based on active channel scanning.
Due to the complexity of the indoor environment, the wireless signals are susceptible to being interfered by indoor furniture and other wireless communication devices. In order to select the most suitable location for the router, the wireless signal propagation attenuation through different obstacles was studied. The power attenuation of the RNs when the RF signals transmitted through different obstacles was analyzed with the practical test result listed in Table 1.
Wireless signal propagation attenuation.

Join the Network through the Assigned Parent. In this case, the parent CN/RN is preconfigured with the 64-bit address of the child device. The procedure for a CN/RN to directly join a device to its network is initiated by issuing the NLME_DIRECT_JOIN.request with the device address parameter set to the address of the device. When this procedure is initiated, the NLME (Network Layer Management Entity) of the parent shall first determine whether the specified device already exists on its network. To address this issue, the NLME shall search its association table (AT) in order to determine whether a matching 64-bit, extended address can be found. If a match is found, the NLME shall terminate the procedure and notifies the next higher layer that the device is already present in the device list by issuing the NLME_DIRECT_JOIN.confirm primitive with the Status parameter set to ALREADY_PRESENT. If a match is not found, the NLME shall, if possible, allocate a 16-bit network address for the new device as well as a new AT entry. This procedure does not require any over-the-air transmissions.
The HMNs join the network through the active channel scanning and choose a RN/CN with the best LQI to join the network. Once a network is selected, it shall then issue the NLME_JOIN.request with the Rejoin Network parameter set to 0x00 and the Join_As_Router parameter set to 0x00 indicates that the device wants to join the network as an end device.
4.2. Network Topology Management
For the WHMS, the network topology control and optimization is a very important factor for network performance such as connectivity, coverage, and life-span. For the cluster tree topology, in order to improve the network throughput, it is better to balance the network load. In this paper, a network topology management mechanism was designed based on the adaptive RF power adjustment function of the RNs.
The network topology management was realized based on the power control. In order to balance the network load, the number of children one RN has was controlled based on the transmit power adjustment. Assuming that the present children HMNs number of one RN is nodenum, and if nodenum is higher than the threshold number nodemax, the transmission power of the RN will adjust from 

5. Software Design
Wireless health monitoring systems require higher reliability than a simple best effort service. Classical reliable transport protocols like Transmission Control Protocol [17], Hierarchical Routing Protocol (HRP) and its improved version [18–20], and AODV [21] are not well suited for wireless health monitoring networks due to characteristics of the network nodes (low computing power, strong energy constraints) and the main applications running on these nodes (low data rates). Thus, in this paper, an improved routing protocol (LHRP) was introduced. Besides, the SMAM was designed to reduce the packet loss ratio of the system when the HMNs are moving and changing their parents.
5.1. LHRP
Due to the life threatening situations, timely data sending is essential in the WHMS. For data to reach the health care center, there must be a proper way of sending data through reliable connection and with minimum delays. As the DHMH designed in this study was aimed at monitoring the aging people in the nursing home or the white collars in the office, the network backbone was fixed and the locations of every backbone nodes were predetermined and well-designed. Based on these features of the network, the Lightweight Hierarchical Routing Protocol (LHRP) was proposed.
The communication within the WHMS possesses some special features which can be summarized as follows. (1) There is no information transmission among HMNs. (2) The HMNs only communicate with their parent RNs while there is no communication among the HMNs and other RNs except their parent RNs. (3) There are no communications among the RNs except those with parent-child relationship. (4) The HMNs send the sampled physiological data to the CN through the parent-child relationship relay and this definitely is the shortest path to the CN. According to the communication features of the DHMH network, we improved the HRP and made it more simple and efficient. The time complexity of the LHRP is
Address Assignment. The CN has the fixed address 0x0000, and the broadcast address is fixed as 0xFFFF. For the other nodes in the network, the stochastic addressing mechanism is used, which can effectively avoid the room waste problem caused by the Distributed Address Assignment Mechanism (DAAM) [22, 23]. Each node maintains an up-to-date two-dimensional table (Association Table (AT)), which contains the network information such as network address, relationship, and LQI, RSSI for all the nodes.
As HMNs, they need to send the sampled physiological data to their parent nodes with direct addresses of their parents and destination addresses of the CN. When needed, the CN broadcasts command frames to all children nodes. For the routers, when they receive a data packet with a destination address of the CN, they just need to forward the packet received to their parent nodes according to the network address stored in the AT. If the router receives a broadcast packet, it will forward the packet to all its children nodes. The packet processing procedure of a RN is shown in Figure 4.

The LHRP routing process and the SMAM process.
In this way, the data can be transmitted directly and need few computations and extra communication overhead. Thus, this protocol largely simplifies the routing algorithm and reduces the end-to-end delay. In Section 4, the experiments were conducted and the results were given and compared with the HRP.
Failure Restoration. As the routing path is fixed, if there is any functional failure in one of the RNs, the data transmission of all its children nodes can be interrupted. To solve this problem, the fault detection and recovery mechanism were designed in this study. If the HMNs and RNs do not receive the ACK frame continuously for N (here we set
5.2. Seamless Mobile Access Mechanism (SMAM) for HMNs
Delivery failures constantly occur in WHMS applications due to node movements and network topology changes. The conventional route reconstruction method designed to address this issue consumed a large amount of resources [23, 24]. In this study, the seamless mobile access mechanism (SMAM) was studied, which uses the “join-before-exit” mechanism to guarantee the seamless switch when the HMNs move from one RN/CN to another RN/CN.
In this study, routers that are composed of the network backbone are static and supplied by reliable powers. As the power consumption is not a constraint for RNs, the RNs can maintain the listening state all the time. If a router node RN02 detects that the LQI_NewParent of HMN01 which is now a child of RN01 is bigger than the LQI_threshold, the RN02 can proactively ask the HMN01 to join the network as its child. The HMN01 decides whether to switch parents by comparing the LQI_CurrentParent of its current parent with
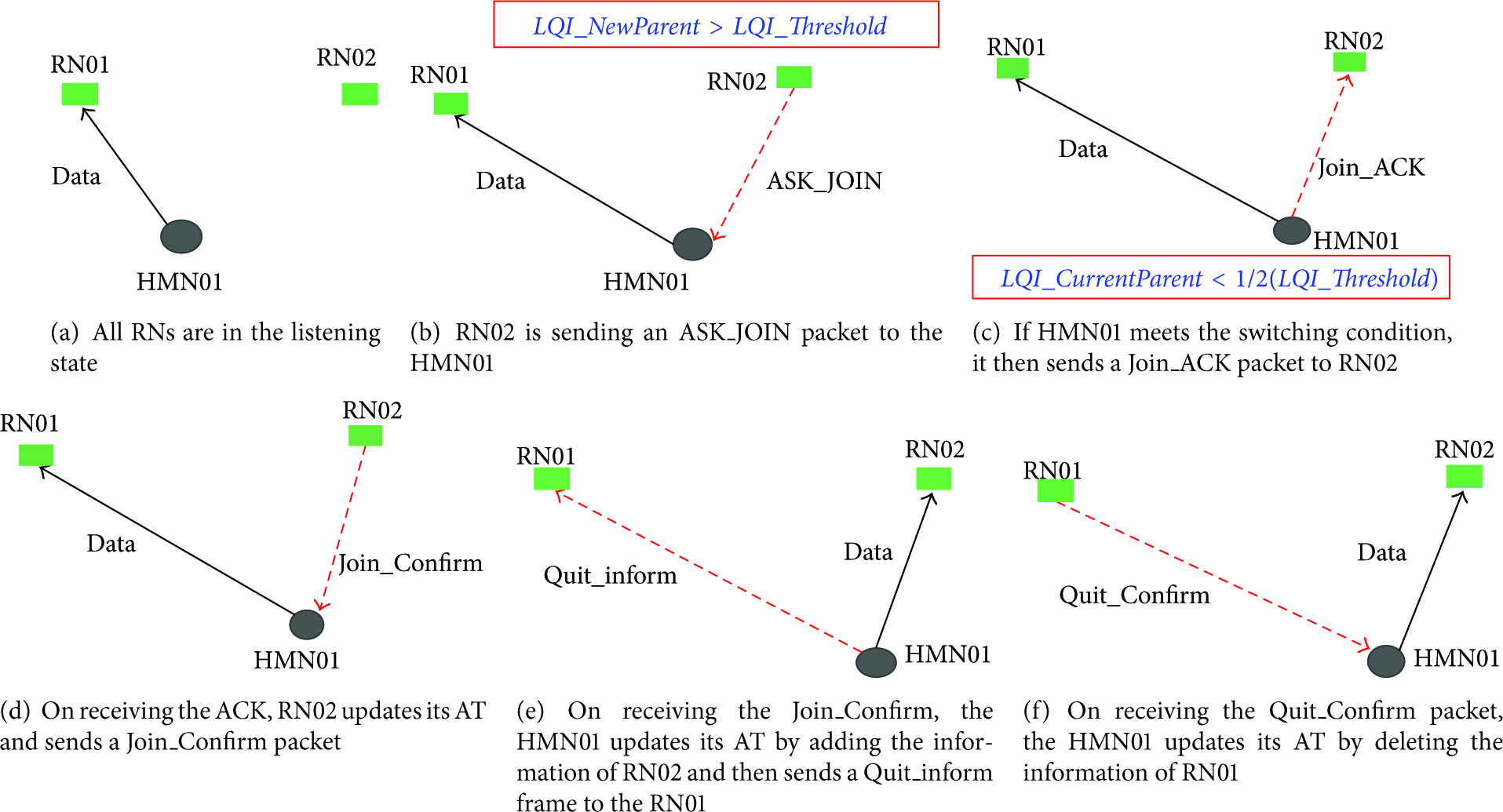
The parent switching process of SMAM.
5.3. Congestion Control and Data Recovery
A reliable WHMS requires that all physiological data sent by the HMNs arrive at the CN. Missing segments that may be lost in the WHMS should be recovered by reliable schemes. Congestion occurs when the data packets generated by HMNs exceed the network capacity. When the networks are congested, intermediate RNs may lose packets, leading to retransmissions of the lost packets and thus a waste of energy that is a very important factor for HMNs to function in the energy limited environments. In the following, a congestion control and data recovery mechanism for the DHMH was presented.
The congestion control mechanism is an essential component for a reliable transport protocol because the congestion leads to packet losses. For data congestion control, each RN can detect congestion based on the overflow of buffers and then it notifies its children HMNs to slow down their sending rates. For data recovery, HMNs use the sequence numbers of packets to signal packet losses, and a gap in the sequence numbers means packet losses. When a loss occurs, a RN receiver sends a NACK requesting the retransmission of the lost messages. Firstly, the one-hop neighbors process NACKs. Then, if one of the neighbors finds the missing packets in cache, it suppresses the NACK message and retransmits the missing packets to the CN. Otherwise, the NACK message is relayed to the next node toward the source.
5.4. Interference Avoidance
There are three kinds of mechanisms to prevent the interference from other technologies such as WiFi, ZigBee which share the same frequency band with ZigBee. (1) Clear channel assessment (CCA): the physical layer of the IEEE802.15.4 provides the CCA ability in the collision avoidance mechanism. (2) Dynamic channel selection: the CN performs a channel scan at the beginning of the network establishment and stores all the available channels scanned. If interference is detected in the communication process, the upper layer of the CN will automatically select a new channel from the stored channels. (3) The direct sequence spread spectrum (DSSS) technique used by ZigBee has stronger antijamming ability compared with the frequency-hopping spread spectrum (FHSS) used by many other standards.
6. Performance Evaluation
In this section, extensive experiments to test the end-to-end delay and the average data reception ratio of the DHMH are introduced. The experiments were conducted in the 11st floor of our office (Kedian building). In the experiments, 1 CN, 10 RNs were used and different numbers of HMNs were worn by the office colleagues. The CN was connected to a PC through the USB interface in the library room, and the RNs were plugged in the socket board whose locations are carefully chosen according to the environment of the library. The HMNs sample the ECG and the SpO2 signal of the wearers and send it to the CN (50 packets/second and 80 bytes in each packet) through one or more hops. The network coves the whole floor with an area of 26.4 m ∗ 52.8 m; the final established network topology in the 11st floor of Kedian building is shown in Figure 6. The experimental results were compared with the traditional HRP system without the mobile support mechanism.

The formed network topology in the 11st floor of Kedian building.
6.1. End-To-End Delay
We tested the end-to-end delay of the system when the sampled data was transmitted to the CN through different numbers of relay nodes. Firstly, we tested the end-to-end delay when one HMN transmitted data to the CN through different number of relay nodes. The HMN sends 50 packets/second and 80 bytes in each packet; the test results is shown in Figure 7(a).

End-to-End delay varies with number of hops (a) and End-to-End delay varies with the number of HMNs (b).
The results show that the improved data transmission protocol reduced the end-to-end delay to some extent. With the increase of the number of hops, the improvement is much more significant. When data transmitted through 10 hops, the averaged end-to-end delay was reduced about 13 ms compared with the result of the original HRP protocol.
And then, the averaged end-to-end delay variation with the number of HMNs was tested. We tested the averaged end-to-end delay when there are different numbers of HMNs sending data to the CN at the same time. Each HMN sent 50 packets/second and 80 bytes in each packet. The test result is shown in Figure 7(b). It can be seen that the LHRP significantly reduced the end-to-end delay compared with the HRP. When there are 30 HMNs sending data at the same time, the averaged end-to-end delay of the ZHMH using LHRP is 38.89% lower than the system using the traditional HRP.
6.2. Data Reception Ratio
We tested the averaged reception ratio when the HMN was moving at different speeds in the building. For comparison, we tested two scenarios with and without SMAM. In both scenarios the HMN sent 50 packets/second and 80 bytes in each packet. The testing result is shown in Figure 8(a). Compared with the results without SMAM, the reception ratio of the ZHMH was improved by 12.76% when the HMNs are moving quickly (running).
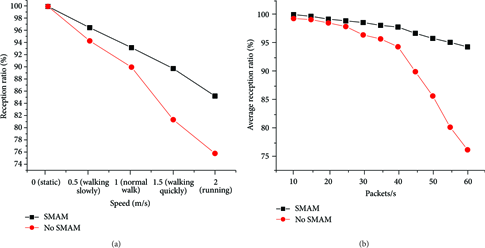
The data reception ratio versus the speed of the HMNs (a) and the averaged reception ratio varies with the data rates (b).
In order to quantify the performance of the SMAM when the data rates are different, the experiments were conducted to test the averaged reception ratio variation with the data rates. One HMN sent data to the CN at different data rates (80 bytes in each packet) when it was moving at the speed of 1 m/s. The test result is shown in Figure 8(b). Experimental results show that data rate increase leads to the improved averaged reception ratio of the SMAM by 19.14% compared with the results without SMAM.
6.3. Long-Term Reliability
To know the long-term reliability of the system, we have continuously tested the system for a week with 1 CN, 10 RNs, and 30 HMNs. And in the experiments, we experienced 5 times of HMNs failures in total. And 3 times of these failures are the HMNs running out of energy; HMNs power failures are caused by not charging the devices timely after they have work continuously for 4 days. And there are also 2 times of electrodes lead-off problems. However, the HMNs failures do not affect the function of the entire system, while, in the long-term and continuous experiment, we did not find the backbone malfunctions.
6.4. Network Throughput
We tested the network throughput of the DHMH when there are different numbers of HMNs when they are sending ECG signals to the CN. The sampling rate of the ECG signal was 250 samples/s, and there were 4 bytes in every sample. The ECG signal was sent once per second, and the data transmission rate was 1 kbytes/s. The testing results are shown in Figure 9. Compared with the HRP without the network topology management mechanism, the network throughput of the DHMH system was improved by 36.4%.
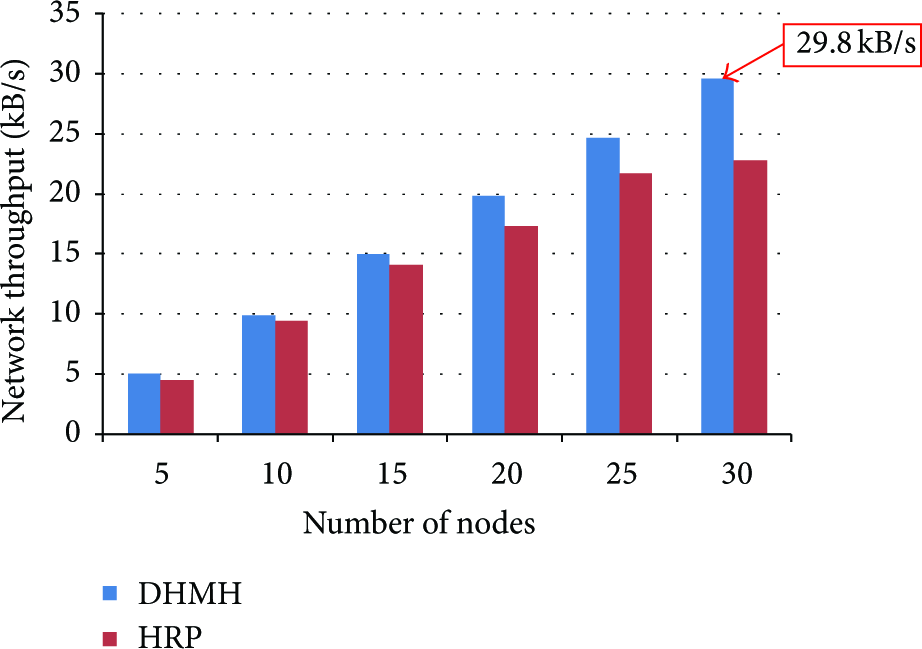
The network throughput varies with the number of nodes.
7. Conclusions
In this paper, we proposed a dynamic heterogeneous and multihop WHMS for indoor health monitoring. The three-tier semi-self-organizing network architecture including both the hardware and the software design was demonstrated. The lightweight protocol (LHRP) was developed to reduce the transmission delay and improve the network throughput. The seamless mobile access mechanism (SMAM) assured the low packet loss ratio when a HMN is moving away from its current parent to another RN/CN node. The health monitoring system characterized with mobile support, low latency, and the high reception ratio of data transmission in different scenarios were validated in experiments. Results showed that the averaged end-to-end delay was reduced by 38.89% when 30 HMNs were sending data at the same time and the averaged reception ratio of the SMAM was improved by 19.14% compared with the results without SMAM. The network throughput of the DHMH was improved by 36.4% when there are 30 ECG monitoring devices working in the network at the same time.
Footnotes
Conflict of Interests
The authors declare that there is no conflict of interests regarding the publication of this paper.
Acknowledgments
This paper was supported by funds of National High Technology Research and Development Program of China (863 program 2013AA041201), National Natural Science Foundation of China (no. 61302033).