
Abstract
We have conducted a critical review on the development of rehabilitation robots to identify the limitations of existing studies and clarify some promising research directions in this field. This paper is presented to summarize our findings and understanding. The demands for assistive technologies for elderly and disabled population have been discussed, the advantages and disadvantages of rehabilitation robots as assistive technologies have been explored, the issues involved in the development of rehabilitation robots are investigated, some representative robots in this field by leading research institutes have been introduced, and a few of critical challenges in developing advanced rehabilitation robots have been identified. Finally to meet the challenges of developing practical rehabilitation robots, reconfigurable and modular systems have been proposed to meet the identified challenges, and a few of critical areas leading to the potential success of rehabilitation robots have been discussed.
1. Introduction
The progress on the studies of rehabilitating robots has been significantly lagged in contrast to the emerging society needs. On the one hand, the population who needs assistance and rehabilitation is consistently increasing; on the other hand, the existing rehabilitation robots have the limited capabilities of personalization and yet they are too expensive for the majority of patients. The performances of existing robots have been proven unsatisfactory [1, 2]. The innovations in the development of the next-generation rehabilitation robots can lead to significant benefits to human beings. In this paper, a critical literature review is conducted to identify the limitations of existing works and clarify the prosperous research directions in the development of assistive robots. In the next sections, the needs of assistive technologies in the healthcare industry are introduced.
1.1. Population of Elderly and Those with Disabilities
The technologies of rehabilitation robots are mainly driven by the increasing demands from vulnerable people with elderly or disabilities population. The number of aged persons prone to need assistance has been increasing at a high rate. The United Nations estimated that today around 500 million people are of age 65 and over, accounting for 8 percent of the world's population [3]. This percentage is consistently increasing. As shown in Figure 1, the proportion of the population aged over 65 years in the United States was predicted to be increased from 12.4% in 2000 to 19.6% in 2030, and the number of the persons aged over 65 years was expected to be increased from approximately 35 million in 2000 to an estimated 71 million in 2030. The elderly tend to be disabled; the relationship between the rate of disabilities and age groups was illustrated in Figure 2 [4]. The number of the population aged over 80 years was expected to be increased from 9.3 million in 2000 to 19.5 million in 2030 [5]. The demands of the handicapped and the elderly are more and more being recognized by politics, industry, and science.

Percentage of US population over age 65, 1950–2050 [4].

Relationship of age groups and the rate of disabilities [4].
Besides the elderly, the persons with disabilities usually need rehabilitation or assistance. The number of the disabled people is rising largely in the world. Disease, accidents, wars, and care improvement contribute to this increase. Take an example of the disease factor; it has been reported that a total of 750,000 individuals are affected each year and the prevalence rate is about 200 to 200 patients per 100,000 inhabitants [6]. Although the prospective epidemiological studies are lacking, the findings of several longitudinal studies indicate that 30% to 66% of hemiplegic stroke patients were not able to recover in 6 months, where only 5% to 20% demonstrate complete functional recovery [7].
1.2. Needs of Rehabilitation Robots
Rehabilitation is to restore a patient's useful life. Rehabilitation is often required for a patient who has been in an accident or just experienced a medical problem. Rehabilitation could help patients recover normal daily functions via different recovery techniques. However, it is important to follow a rehabilitation process carefully. The rehabilitation activities must be progressive in nature and done on a regular basis. Failure to try to improve in both strength and flexibility may cause continued weakness and inability to function.
Robots can provide both the movement controllability and the measurement reliability, which makes them ideal instruments to help neurologists and therapists address the challenges facing neurorehabilitation. Rehabilitation robots need sensors that record the movement data such as the position, velocity, and force/torque of joints. They are equipped by actuations to move the subject's limb, and they are designed to make the compensations of physical capabilities of patients. Rehabilitation robots can be classified into actuated robotic limbs and the robotic suits that enclose the affected limb like an exoskeleton frame [8].
Rehabilitation robots are expected to benefit the groups of elderly, injured, disabled, or even average people [9]. In this figure, a curve with light gray shows the trend of physical capacity of a person, a curve with dark black shows the trend of physical capacity when an assistive rehabilitation device is applied, and a blue area shows the improvement of physical capacity for elderly, injured, disabled, or normal people. The development of rehabilitation robots has been stimulated by the scientific advance on cerebral plasticity and functional recovery.
Robots are very helpful to serve various purposes of rehabilitation. For the patients with severe paresis, robots can provide the passive movement of the upper limb. Passive movements activate cerebral areas involved in active movements. For the patients with some movement capacity, robots can support the weight of the limb against gravity or due to the physical interaction between the robot and the subject. A robot and a patient can exchange forces or share position based on the type of control system. This provides a greater opportunity for movement than the patient might otherwise have. Rehabilitation robots aim to help therapists by increasing the duration of rehabilitation exercises, but especially their variety, quality, and adaptation to the patient's individual state [10]. It has been demonstrated that the potential recovery following stroke has been previously underestimated [11]; moreover, the constraint induced therapy has shown that functional improvements are possible even several years after stroke [12].
Studies have shown that therapy should be intense and repetitive in order to achieve the maximum benefit. In order to provide such training, rehabilitation equipment must be activated. Rehabilitation robots are tireless in contrast to human-being trainers. Besides, because of their sensors, robots can monitor movement quality as well as progress constantly, providing highly specific feedback to patients to aid learning. The benefits of robots for rehabilitation are therefore multiple: they can produce repetitive high quality movements, allowing increased intensity of rehabilitation; they can provide a large variety of exercises for the therapist to choose from; they provide a man-machine-interaction which allows an objective measure of progress, which itself can condition changes in the interaction by altering control parameters [10].
1.3. Significance of Research
All industrialized societies are facing similar problems centered on the issue of disability. Rehabilitation robots are promising in terms of addressing these problems. Rehabilitation robots provide the medical and nursing staff with robotic aids that allow them to accomplish their tasks in more time efficient manners. If a patient can be operated on more safely and with minimal recovery time, a surgical facility can accommodate more patients. Robots in the medical and healthcare fields address a variety of areas including surgery, rehabilitation, and mobility, while increasing the quality of service to the patient. Technology-Related Assistance for Individuals with Disabilities Act has also stimulated assistive technologies to create these devices through state and federal efforts. These US laws increased the awareness for the need for assistive devices and services to improve the quality of life, as these devices also would minimize the cost to the individual and society [13].
Another critical issue related to today's health care system is the ever-increasing cost. New efficient techniques, partially applying mechanical and robotic aids can help reduce the costs and ensure the survival of public health care systems. The main scientific challenges are identified in the field of assistive technologies to support elderly and handicapped persons in their home environment; in surgery and in rehabilitation. Further development of medical and surgical robotics is one of the key trends to track the scientific community in order to address the societal changes in the next few decades. Existing robots have the critical issues of capability of personalization and high price and performance ratio. The proposed idea can be expected to address these issues and stimulate the application of rehabilitation robots in healthcare industry greatly.
There are significant social implications for the increased use of robots in society. A range of different research disciplines has to work with industry and involve both clinical staff and end users, if the research is to be successful in moving to the mainstream [14]. One recent review has drawn a similar conclusion that robotic rehabilitation improves motor function of the impaired arm as well as strength but these improvements do not transfer into activities of daily living [15]. The robotic therapy is effective although the benefit has not been illustrated when the same intensity is delivered as traditional therapy. The robots were principally used for their abilities to provide a large number of repetitions. Coupling of rehabilitation robots with fun, motivating, virtual reality interfaces is an excellent manner to increase intensity of rehabilitation. This has important implications with regard to the capacity of therapy services to deliver higher intensity therapy. If robots are as good as therapists and can provide a means to deliver more therapy, this has obvious advantages for patients [10].
2. Examples of Rehabilitation Robots
Rehabilitation robots were studied primarily in motor relearning and recovery of the upper limbs. Those robots provide high-intensity, repetitive, task-specific, and interactive exercises of the impaired upper limb. An example of the upper-limb rehabilitation robots is the MIT-Manus. It was developed for shoulder and elbow training [16]. The clinical trials of MIT-Manus have shown that the robot-aided neurorehabilitation had a positive impact, reducing impairment during both the subacute and the chronic phases of stroke recovery [17]. Since then, many other robots have also been developed. The Lokomat was used as a bilateral computerized gait orthosis used in conjunction with partial body weight support treadmill walking. It did not provide active assistance at the ankle, and the foot drop is counteracted by a spring-loaded mechanism to support dorsiflexion during the swing phase of gait [18]. Another two lower limb rehabilitation robots are Hesse's Gait Trainer I and Active AAFO [19, 20]. Ankle joint perturbators were developed to introduce ankle joint rotation to stretch ankle extensors [21, 22]. A Stewart platform-type haptic interface called “Rutgers Ankle” was introduced to measure foot position and orientation. The system uses double-acting pneumatic cylinders, linear potentiometers, and a 6-DOF force sensor. It provides resistive forces and torques on the patient's foot, in response to virtual reality-based exercises [23]. Based on the differences of functions, Tejima classified the rehabilitation robots into four types: augmentative manipulation (wheelchairs, workstation, power-feeder, mobile robots, robotic orthoses, and robotic room), augmentative mobility (robotic wheelchairs, mobility aids for visually impaired people, and walking support systems for the elderly), therapy robots, and robots for help care-givers [24].
Rehabilitation robots can be distinguished by the mechanism of human-robot interaction and the number of segments which the robot can directly control. From the point of view of human-robot interaction, some robots are adapted from industrial robots with more or less degrees of freedom but only one point of physical contact between the distal end of the upper limb and the extremity of the robot. Two types of robot in this category are traditional manipulators and cable robots. MIT Manus resembled a traditional industrial manipulator. The examples of cable robots are NERbot, Maribot, Kinehaptique, and Gentle/s [10]. Cable robots impose forces or positions or provide assistance at the point of contact between the patient and the machine but only at this point. They cannot, therefore, directly control the different movement synergies used by patients in order to achieve the displacement of the end-point. A new category of recent rehabilitation device is robotic orthoses. These orthoses allow contact at several key points of the upper limb and can therefore control the different segments of the limb. This implies that they can influence coordination patterns and/or better follow the particularities of the patient's postures or movements. Examples of robots in this new category are (i) anthropomorphic robots, which are in contact practically with the whole limb such as ARMin and RUPERT, and (ii) the robots which have discontinuous contact with limb such as ARMguide and Dual Robotic System [10].
Figures 3, 4, 5, 6, 7, and 8 have illustrated a few examples of the structures used for rehabilitation robots. All of them have a certain number of actuators to provide assistive motions to the subject, but the system topologies are so different from one to another. However, it is unnecessary to have so many variations of components, from where different rehabilitation robots can be assembled. The study on reconfigurable and modular architecture for rehabilitation robots is lacking. It has also been discussed that existing rehabilitation robots have two critical issues of the limited capability for personalization and the high ratio of price and performance.

Mirror image movement enabler system [48].

Wrist assistive rehabilitation device [49].

MIT's ankle robot system [17].

Lokomat robotic gait orthosis [8].
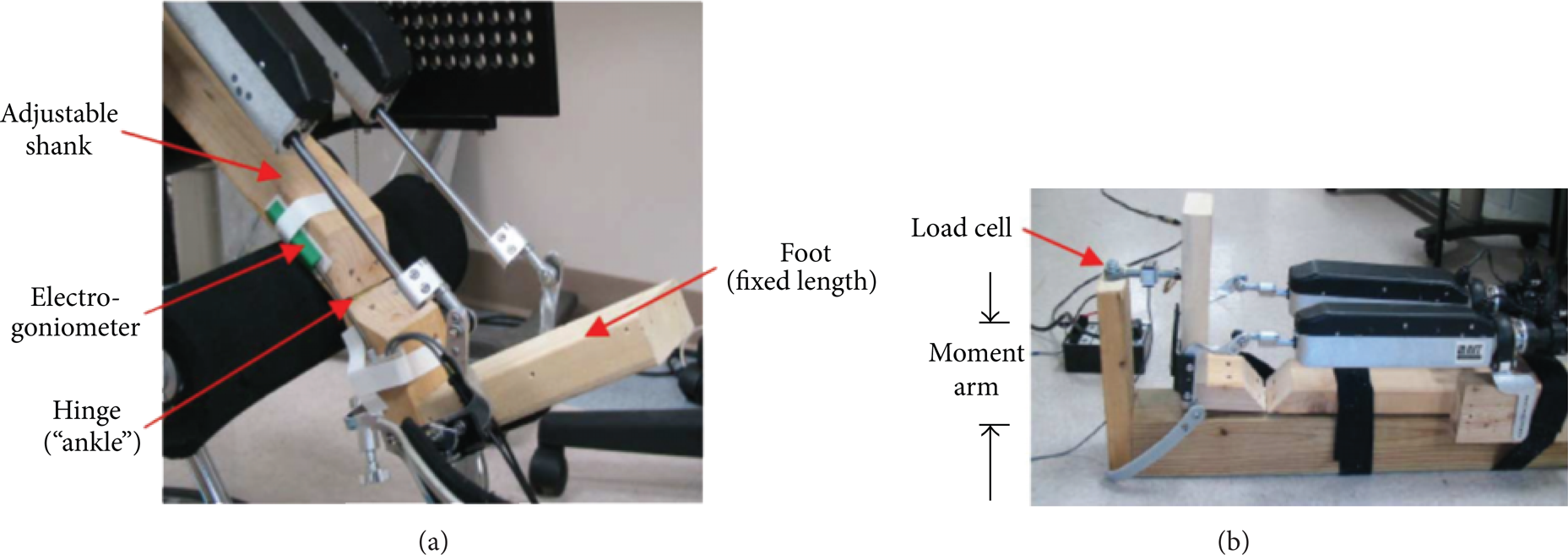
Ankle rehabilitation [17].

CPMs for lower limbs [50].
3. Issues to Be Addressed
Over the last decade, the introduction of robotic technologies into rehabilitation settings has progressed from concept to reality. The studies have demonstrated the efficiency and advantages of rehabilitation robots for assessing and treating motor impairments in both the upper and lower extremities [25]. Several surveys have agreed that the high intensity repetitive movements constitute an important contributor to the effectiveness of robot-assisted therapy [26]. However, there is a significant gap between the outcomes of rehabilitation robots and people's expectations. Equipment to improve the quality of physical therapy is scarce [27, 28].
One issue is the difficulty of personalization. It is desirable to provide the robotic assistance to patients in such a manner that the resulting interaction between the robot and the patient is smoother. The level of assistance should be tuned according to the patients' residual abilities [29]. Every patient has his/her specific abilities, functional needs, and interests. An emphasis on more autonomous use of robotic therapy systems makes the personalization of the human-technology interface very important [30]. There are two key components of the personalized interfaces: the physical interface (e.g., the device itself, its physical settings, and the range of operation of a device relative to the user's torso) and the communication interface. The greater research challenge relates to what and how to personalize and how to customize and adjust the focus of therapeutic intervention, especially when a patient demonstrates some improvement. This suggests the importance of a training protocol that is easily varied, in terms of use of both the full “ability” workspace and the types of tasks performed within the workspace. The design of robot dedicated to person with disabilities necessitates users' implication in all steps of the product development: design solution, prototyping the system, choice of users' interfaces, and testing it with users in real conditions. Before any design of any system, it is necessary to understand and meet the needs of the disabled users [31].
Cost is another major issue to promote rehabilitation robots. The price/performance ratio is rather dissatisfactory due to the high cost of development combined with a relatively low benefit for patients and clinics. As surveyed by Elarbi-Boudihir [32], the assistive robotic products developed to date have varied in price from about $9,000 to $100,000. Despite a large number of rehabilitation robots being under investigation, a very small portion of the developed rehabilitation robots have been commercialized; until 2004, about 225 devices had been sold, which relates merely to total sales of US$4.64M [32].
As a summary, rehabilitation robotics is penetrating the market very slowly and is still seen to be a “future technology.” The critical problems are the difficulty of personalization and high cost. For low-income and middle-income classes, only 5%–15% of people who need assistive devices and technologies have access to these technologies. There is a shortage of personnel trained to manage the provision of such devices and technologies. Furthermore, research and development projects in rehabilitation robotics are seen as particularly critical in terms of outcomes and results. However, the research and development on rehabilitation robots are emerging due to the fact that the cost of excluding people with disabilities from taking an active part in community life is high and has to be borne by society, particularly those who take on the burden of care. This exclusion often leads to losses in productivity and human potential [33].
4. New Concept: Reconfigurable Modular Architecture for Rehabilitation Robots
Each potential patient or client has different abilities, functional needs, and interests. This suggests that the personalization of a prescribed therapeutic program is essential to an assistive device. An emphasis on more autonomous use of robotic therapy systems makes the personalization of the human technology interface very important.
There are two key components of personalized interfaces: the physical interface (e.g., the device itself, its physical settings, and range of operation of the device relative to the user's torso) and the communication interface. Perhaps the greater research challenge relates to what and how to personalize and routinely customize and adjust the focus of therapeutic intervention especially as a client demonstrates improvement. This suggests the importance of a training protocol that is easily (and often purposefully) varied, in terms of use of both the full “ability” workspace (including force assistance to gently expand this ability space) and the types of tasks performed within the workspace. The design of a robot configuration dedicated to person with disabilities necessitates users' implication in all steps of product development: design solution, prototyping the system, choice of users' interfaces, and testing it with users in real conditions. Before any design of any system, it is necessary to understand and meet the needs of the disabled users.
However, the requirements of personalization bring the challenge to generate a large number of robotic configurations at a low cost. Two major hurdles for the promotion of the rehabilitation robots in real life are the lacking of personalization and high price/performance ratios. Significant research and social contributions can be made when this research leads in the right solution to address these two issues. A proven method to make a trade-off for this conflict is to use reconfigurable and modular architecture.
The benefits of reconfiguration and modularization to product variations and the cost reduction have been well accepted by manufacturing industries. The international standards had been established to standardize the design and fabrication of modular units in the seventies. Modular machine tools have been on the market over a decade. Many workers have studied different modular machine tools. For example, the modular synthesis of advanced machine tools has been proposed to customize the configurations of modular machine tools. However, modular machine tools are majorly used to increase product variants by the machine-tool producers. End-users often purchase machine tools with a specific configuration, and these machine tools are rarely reconfigured after their installments. Parallel kinematic machines are another type of reconfigurable machine [34]. Conceptual reconfigurable machine tool has been studied at the University of Michigan to meet the requirements of modularity, integrability, customization, convertibility, and diagnosability, so that the machines can reconfigure frequently in the fast-changing environment [35, 36].
A comprehensive review on existing modular machining tools was conducted [37]. A few examples of reconfigurable tools have been illustrated in Figures 9–13. Figure 9 has shown an apparatus for constructing a composite structure [38]. It is comprised of a matrix of threaded pins with pivoting ends attached to a flexible layer. The position of the flexible layer could be adjusted according to a configuration suitable for constructing the composite structure. More specifically, the flexible layer had internal reinforcing elements for added strength and durability. Figure 10 is a reconfigurable die consisting of an array of the pins. Each pin in the die was a simple hydraulic actuator outfitted with an inline NC solenoid valve to control its vertical position. Once the pins were set, the entire matrix was clamped into a rigid tool [39]. Figure 11 has shown a reconfigurable fixturing system developed at the GM. The system consisted of locating and supporting modules which could be placed on the magnate base. Modules were kept in the chunks of the tool storage. Different modules could be selected for different products. The system was automated on a CNC machining center or setup machine. A system was applied in fixturing and machining of aluminum engine cylinder heads of different designs and machining operations [40]. Figure 12 has shown a modular system consisting of active and passive modules. A vision-guided robot was used to set up all modular elements. The number and distributions of the modules were determined by the requirements of the work piece [41]. In Figure 13, a flexible grabbing tool used the shape memory alloy wires for motive force. The clamp consisted of a 4 by 4 array of fingers, which could be locked by the squeezing action of heavy-duty Belleville springs [37].

Adjustable fixture for composite structure [38].
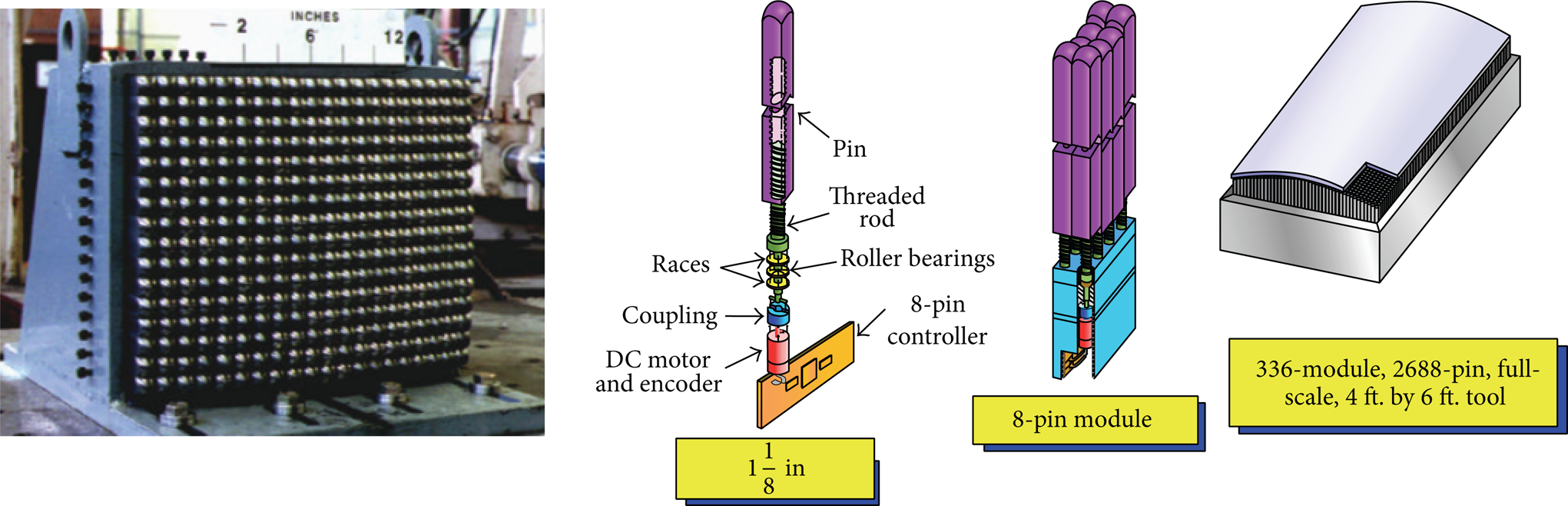
Reconfigurable dies [39].

GM magnate fixtures [40].

A PKM-based reconfigurable tool [41].

MIT conformable clamp [37].
To address the issues of existing rehabilitation robots, this study is proposed to develop a reconfigurable and modular robotic architecture. On one hand, a reconfigurable and modular architecture of rehabilitation robots will be developed. Under such architecture, a robotic system consists of a set of modules; a large number of robot configurations can be generated by selecting different numbers and types of modules and assembling the selected modules in many possible ways. Each of them can be applied to fulfill the specific need of an individual patient. Therefore, the performance of the robot in the application can be optimized to meet the needs of individuals. On the other hand, along with the personalization of a robot configuration, the modularization can reduce the cost of rehabilitation robots. The reduction of cost is contributed by three key factors. (i) There are limited types of modules and each type of module has a considerable large number. Therefore, the modules can be manufactured in mass production. (ii) The number and types of modules in a robot configuration can be minimized to meet only the set of specific needs required by one individual. (iii) Modules are reusable. In many cases, the duration of a robot configuration serving for an individual is relatively short in comparison to the lifetime of the modules. Once a rehabilitation mission is accomplished, these modules can be disassembled and ready for the next configuration in another application. With the improved performance from personalization and the cost reduction from mass production and reconfiguration, the performance/cost ratio is expected to be increased significantly. Eventually, it results in that the rehabilitation robots become accessible to the majority of the patients. The modularization also brings the benefit of openness and extensibility. With the advance of new technologies, new types of the functional modules can be introduced into the system and work with other available modules seamlessly.
5. Research Tasks
To develop reconfigurable rehabilitation robots, we think the researches at the following tasks are necessary and, correspondingly, the methodologies and tools are available to fulfill these tasks:
to study the relation between a reconfigurable modular architecture and system capability of personalization and functionalities and quantify the impact of reconfigurability and modularization for the personalization and the improvement of the ratio of price and performance,
to study the methodologies for system reconfiguration,
to investigate the methodologies for real-time control for rehabilitation and the decentralized control of modular robots,
to study the methodologies for the automatic kinematic and dynamic modeling of various configurations from a modular system,
to conceive a novel rehabilitation robotic system with reconfigurable modular architecture and build the prototype robot for the ankle or wrist rehabilitation,
to conduct the simulation and experiments to evaluate the performance of the robot.
5.1. Architecture Design
The examples of rehabilitation robots in Section 3 demonstrated few common features; consequently, their targeted applications were very specific and narrow. It implies that those systems have the limited capability for personalization. In addition, the majority of components are customized, which leads to a high cost in fabrication. Bear in mind that it is unnecessary to design unique rehabilitation robot for each specific need. Therefore, a reconfigurable and modular robotic architecture has been proposed here. The idea behind this new architecture is elaborated as follows.
A human being's body can be treated as an assembly of the objects such as the head, hands, feet, and legs. Joints among the objects allow relative motions so that human being can have many different motions. As shown in Figure 14, an object, such as a fist or foot, has a certain volume, which can be defined by a set of the boundary surfaces. At the detailed levels, a surface can be represented by a set of edges, and an edge can be represented by a set of key points. Therefore, the motions of key points can be used to represent the motion of an object.

A Body's motion represented by the motions of points with respect to time.
To implement the motion control of key points on boundaries, some instances of configurations from a reconfigurable modular architecture in Figure 15 are illustrated. Modular components are pin-array like platform, where the number of pins and the configuration of array can be customized to meet different functional requirements of rehabilitation robots. The tips of the pins will keep contact with human body such as a foot, a leg, or the backside of a body. Via the control of the pin position, the parts of the human being bodies can be driven to generate the required motions for rehabilitation.

Some instances of configuration for a modular architecture.
5.2. System Reconfiguration
Configuration design is to determine task-oriented configuration when a patient's requirements are given. Task-oriented configuration design is an optimization problem with a design space with mixed types of design variables [42–46].
Modular architecture reduces the design space of original design problem with no modular architecture greatly. Moreover, encapsulated modules bring the couplings of design variables in different disciplines. Classic machine design theories cannot be applied in the design of modular systems directly. Modular architecture diminishes the boundary of sequential design tasks, for example, the boundaries of type synthesis and dimensional synthesis. When a module is specified for a configuration, its type is determined, so are its geometries and dimensions. Concurrent optimization configuration design (COCD) can be used to support the task-orientated configuration design [47]. COCD is specially developed to support the configuration design of a system with strongly coupled design variables.
5.3. Automated Modeling for Kinematics and Dynamics
The configuration design under a set of given task requirements is involved in the evaluation of a large number of design alternatives in the design space, including the robotic performance in kinematics, dynamics, and control, while most of modeling methodologies were developed for robots with dedicated structures. Therefore, those methodologies should be advanced in the sense that their flexibility should be enhanced to model kinematic and dynamic behaviors of robots directly based on modular design variables. The complexity of an automated modeling process depends on the nature and number of modular variables of the reconfigurable system. Two alternative modeling approaches are “direct” and “indirect” modeling. Direct modeling refers to the procedure of generating the direct relations of modular variables of disciplinary behaviors of robots; it should be tailored to one modular system and lack of flexibility in dealing with other modular systems. Indirect modeling decomposes the entire modeling process into two steps, so that the existing modeling methodologies can be utilized. The first step is to bridge modular variables and disciplinary variables; for robotic systems, disciplinary variables can be kinematic and dynamic variables in the Denavit-Hartenberg (D-H) notation. The second step is to utilize existing methodologies to model behaviors of robots based on disciplinary variables.
5.4. Robot Control and Rehabilitation
Because of the modularized architecture, two levels of control should be taken into consideration. The first type control is for rehabilitation activities. The lack of a solid understanding of how motor recovery can be promoted has led to the ad hoc development of control algorithms based on some concepts from rehabilitation, neuroscience, and motor learning. The modes for this type of control can be classified into three categories. (i) Passive: the patient is inactive and the robot moves his/her body. This mode might be suitable for preventing muscle contractures but its effectiveness in stimulating motor recovery is doubtful. (ii) Active assisted: the robot partially assists the patients' movement. This movement is important when patients are able to initiate movement but have difficulty in completing a movement towards a target. (iii) Active constrained: this mode forces concentration and targets particular muscle groups and specific coordination patterns [42]. To maximize the capability of a reconfigurable modular robotic system, different control modes should be explored so that the control system can be flexible to be tailored to specific patients.
The second type of control is for the decentralized control of a modular system. Since system components are modularized and some modules have their controllers at the module level, the system-level objective has to be achieved by the coordination of module-level control.
Open architecture control (OAC) seems an appropriate infrastructure to control reconfigurable robots. OAC refers to hardware and software systems designed to address a broad variety of applications. Modular components used for a reconfigurable robotic system can be from different manufacturers, yet, due to use of open standards, the hardware and software work together. Such openness engenders competition among component suppliers and works in favor of system integration. OAC would benefit a reconfigurable robotic system in the sense that heterogonous hardware and software components from different vendors can integrate seamlessly, the system flexibility can be enhanced, and the maintenance and upgrade costs can be reduced.
5.5. Prototyping and Validation
There are many ways to develop a reconfigurable modular system for the verification of the hypothesis and methodologies. The modular components to generate motions for robotic configurations will be critical. Since one of the objectives is to reduce the cost of the rehabilitation robots, different solutions for the actuations (pnumetrical, hydraulic, or electrical motors) will be compared to determine the suitable type of actuations for the reconfigurable modular system. Another important aspect is the interface of a robot configuration with a patient. Since the system is designed for the disabilities or elderly, it is crucial to possess an easy interface, so that the patients can operate the system easily without little help.
In prototyping a reconfigurable rehabilitation robot, various application scenarios can be considered. For example, the device for the ankle recovery can be used to illustrate the feasibility of reconfigurable systems [45]. Moreover, the possibilities of using a reconfigurable pin-array platform for the rehabilitation of hand and wrist injuries can be investigated. To demonstrate the design concept, the CAD models of all of the parts and off-the-shelf components should be designed and prototyped. As the validation in a virtual environment, in the feasibility study, 20%, 50%, 75%, and 95% percentiles of avatars are used as the virtual patient's models to demonstrate the performance of the reconfigurable rehabilitation robots. The preliminary test should be conducted to evaluate the adjustability of sizes, motion ranges, and the levels of the powers and velocities for rehabilitation. The possibility of tests on actual patients should also be explored to acquire the first-hand feedback from right users.
6. Summary
Many industrialized countries are suffering from the limited resources for healthcare and ever-increasing number of disabled and elderly population. A practical way to address this issue is to apply more advanced and reliable robotic technologies for the healthcare industry. Existing assistive technologies are unsatisfactory in meeting personal needs and fulfilling the required functions at a reasonable cost. Any innovation to improve the capability of personalization or reduce the ratio of price and performance will stimulate the applications of robotic technologies in healthcare significantly.
Reconfigurability and modularization can be the solutions to address these issues; they can promote the applications of robotic technologies for more functionalities and targeted patients. A reconfigurable modular robot consists of a set of modules; different types and number of modules can be deployed and these modules can be assembled in different configurations. Therefore, the same system can generate many configurations for meeting the different needs of patients. As a result, the same set of modules can be utilized in many applications; this leads to a higher rate of the utilization. The modular architecture also has its advantages in maintenance and extensibility. Finally, although our survey and discussion are focused on rehabilitation robots, the similar issues occurred to the other types of medical robots; the methodologies for reconfigurable modular robots can be surely extended and used in designing other medical robots.
Conflict of Interests
The authors declare that there is no conflict of interests regarding the publication of this paper.