
Abstract
People worldwide are getting older and this fact has pushed the need for designing new, more pervasive, and possibly cost effective healthcare systems. In this field, distributed and networked embedded systems, such as wireless sensor networks (WSNs), are the most appealing technology to achieve continuous monitoring of aged people for their own safety, without affecting their daily activities. This paper proposes recent advancements in this field by introducing WSN4QoL, a Marie Curie project which involves academic and industrial partners from three EU countries. The project aims to propose new WSN-based technologies to meet the specific requirements of pervasive healthcare applications. In particular, in this paper, the system architecture is presented to cope with the challenges imposed by the specific application scenario. This includes a network coding (NC) mechanism and a distributed localization solution that have been implemented on WSN testbeds to achieve efficiency in the communications and to enable indoor people tracking. Preliminary results in a real environment show good system performance that meet our expectations.
1. Introduction
Medical experts agree on the projections that forecast in the next couple of decades the population aged over 65 years to increase from 6.9% to 12.0% worldwide and, in particular, from 15.5% to 24.3% in Europe [1], with an average worldwide life-span expected to extend another 10 years by 2050 [2]. The growing number of older adults increases the demands on the public healthcare system and on medical and social services. Increased life expectancy reflects, in part, the success of public healthcare interventions [3], but public healthcare programs must now respond to the challenges created by this achievement, including the growing burden of chronic illnesses, injuries, and disabilities and increasing concerns about future care-giving and healthcare costs [4]. A study of Frost and Sullivan [4] has clearly indicated that, in almost all countries worldwide, healthcare spending per capita is rising faster than per capita income. If current trends hold, by 2050 healthcare spending is expected to double, claiming 20%–30% of gross domestic product (GDP) for some economies and 20% by 2015.
In this context, new technologies that can help seniors live at home longer provide a “win-win” effect, both improving quality of life and potentially saving enormous amounts of money. The forecast above clearly highlights the compelling need of delivering high-quality care to a rapidly growing population of elderly, while reducing the overall healthcare costs. Until recently, the cost of providing a continuous patient monitoring flow of patients' data, from patients' homes to care providers, was prohibitive, mainly because it requires continuous in-person patient monitoring through specially trained care givers available full time or dedicated communication and appropriate device infrastructures.
Nowadays, with the increasing availability of broadband technology at home, along with wireless networks and a wide range of consumer health electronics, an end-to-end infrastructure has begun to emerge, enabling new “pervasive healthcare” applications, more often shortly termed as “e-Health” applications. The availability of these networks and the widespread use of mobile devices make two-way continuous interactions between patients and their care providers feasible, regardless of physical location.
On the other hand, the use of information and communication technologies to facilitate and improve healthcare and medical services involves the use of appropriate devices both on patients and embedded in the living environment. Researchers and educators predict that these gadgets will soon turn the home into a medical nurse, keeping record on everything from pill-taking routines to signs of imminent crises.
For seniors, the benefits of an idealized medical smart home are physical, psychological, and emotional. Aging in place means continuing with familiar routines while health data, detection of critical conditions, and remote control of certain medical treatments are wirelessly made available to doctors, caregivers, and concerned family [5]. For society, the bonuses include significantly reduced health care costs and happier elders. Consequently, it is natural to expect that consumers will embrace in-home technologies precisely because they can potentially save them money on the cost of unnecessary time-consuming doctor visits, thus not jeopardizing their daily life activities.
On this subject, this paper aims to present the WSN4QoL project [6], which involves the design of wireless sensor networks (WSNs) specifically suited to meet healthcare application requirements. WSN4QoL is a 3-year project started at the end of 2011 and still ongoing. With the intent of bringing together experts, from industry and academia, it proposes the use of advanced WSN technologies for pervasive healthcare applications. In particular, it aims at providing network coding (NC) for multihop/cooperative diversity in the data communication protocol as well as distributed localization algorithms to meet the specific requirements of WSNs-enabled healthcare applications, namely, energy-efficiency, low-latency, data reliability, context-awareness, and security. Extensive performance analysis of the proposed solutions is given through numerical simulations as well as proofs-of-concept in real-world experiments, through the implementation into real healthcare devices.
The rest of the paper is organized as follows. Section 2 overviews the full system architecture presenting the design challenges offered by the general reference scenario, while Section 3 puts particular emphasis on the key elements of the communication protocol stack and the middleware of services offered to the application designers. Sections 4 and 5 present the NC and the localization testbeds, respectively, that have been implemented to evaluate the solutions proposed in real(istic) environments. Section 6 deals with a summary of current research efforts with similar objectives to WSN4QoL. Finally, Section 7 concludes the paper with a view on some of the open issues to be addressed as ongoing and future work in the remaining WSN4QoL project period.
2. WSNs System Architecture Design for E-Health
WSNs are distributed networked embedded systems where each node combines sensing, computing, communication, and storage capabilities. They have emerged as a new networking environment that provides end-users with intelligence and a better understanding of the environment. Because of their wide variety of applications, it is envisioned that, in the near future, WSNs will become an integral part of our everyday lives [7]. WSNs are wireless ad hoc networks composed of inexpensive nodes with sensing capabilities and a limited number of data sink nodes. These nodes communicate among each other by forming multihop wireless networks and by maintaining connectivity in a centralized or a distributed manner. The network topology is, in general, dynamic, since the connectivity among the nodes may vary with nomadic and mobile nodes.
2.1. Challenges
Although fundamental research results on WSNs theory and practice have been achieved for many different applications, for example, traffic monitoring, plant monitoring in agriculture, and infrastructure monitoring, the application of this technology to e-Health poses some unique application-specific challenges and constraints. In particular, the efficient design of a WSNs-enabled pervasive healthcare system is characterized by the following intrinsic differences with respect to “general-purpose” WSNs design, which require special attention [8]. (i) The devices have limited available energy resources, as they have a very small form factor. (ii) A low transmit power per node is needed to minimize interference and to cope with health concerns. (iii) The devices are located on the human body, which can be in motion. WSNs for e-Health should therefore be robust against frequent changes in the network topology and channel variability. (iv) Data mostly consist of medical information; hence, high reliability and low delay/latency are required. (v) Stringent security mechanisms are required to ensure the private and confidential character of data. (vi) Context-awareness through cooperative localization in outdoors and indoors is crucial to enable a prompt reaction in case of emergency. (vii) The devices are, in general, very heterogeneous. They may have very different demands or may require different resources of the network in terms of data rates, power consumption, and reliability.
Along these lines, the main research objective of WSN4QoL is to provide fundamental research advances, proof-of-concepts, and real-life implementations on the main enabling technologies for WSNs-aided e-Health applications. More specifically, disruptive techniques such as cooperative wireless communications protocols and distributed algorithms are investigated. The proposed solutions are designed, optimized, and implemented in real-devices by taking into account the specific requirements of e-Health: energy efficiency, low-latency delivery of data, data reliability, and security. In more detail, the research objectives of WSN4QoL include the following: (i) to design a protocol stack architecture, which can accommodate a variety of protocols, algorithms, and sensor devices for pervasive healthcare applications, (ii) to develop energy-efficient and performance-guarantee cooperative protocols and NC schemes for WSNs-enabled pervasive healthcare applications, (iii) to propose advanced distributed localization protocols and algorithms specifically suited for the scenarios (e.g., indoors) envisaged by WSNs-enabled pervasive healthcare applications, (iv) to conceive effective, efficient, and resilient security solutions for the proposed algorithms and protocols, (v) to implement and assess the performance of the protocol stack in a WSN testbed, and (vi) to integrate the proposed solutions in real devices and validate them in real working environments.
2.2. Reference Scenario
Similar to other works in literature (e.g., [9, 10]), the reference system architecture proposed in this project is as depicted in Figure 1. It is a three-tier system architecture, where at the lowest tier (Tier-1), a Bluetooth-enabled WBAN connects sensors to a local collector (i.e., a hub), which can be a portable embedded PC or a PDA. The hub needs to communicate with WBAN devices through a Bluetooth radio module and then send measurements reports towards a residential gateway, through a ZigBee/IEEE 802.15.4 based multihop WSN (Tier-2). The gateway is able to perform local computation and forward data to the public IP-based network (Tier-3) towards the professional caregivers for real-time analysis.

Reference healthcare 3-tier system architecture.
In recent work [11–13] we proposed alternatives to the Bluetooth for the communications among the devices forming the WBAN at the Tier-1. Nevertheless, in the WSN4QoL project, our focus is on the efficient data transmission over the WSN network at the Tier-2, as well as supporting real-time people localization in a fully distributed way.
3. System Protocol Stack
Figure 2 shows the intended communication protocol stack for the WSN of the reference scenario in Figure 1. Moving from the bottom, the protocol stack is composed of the following entities.
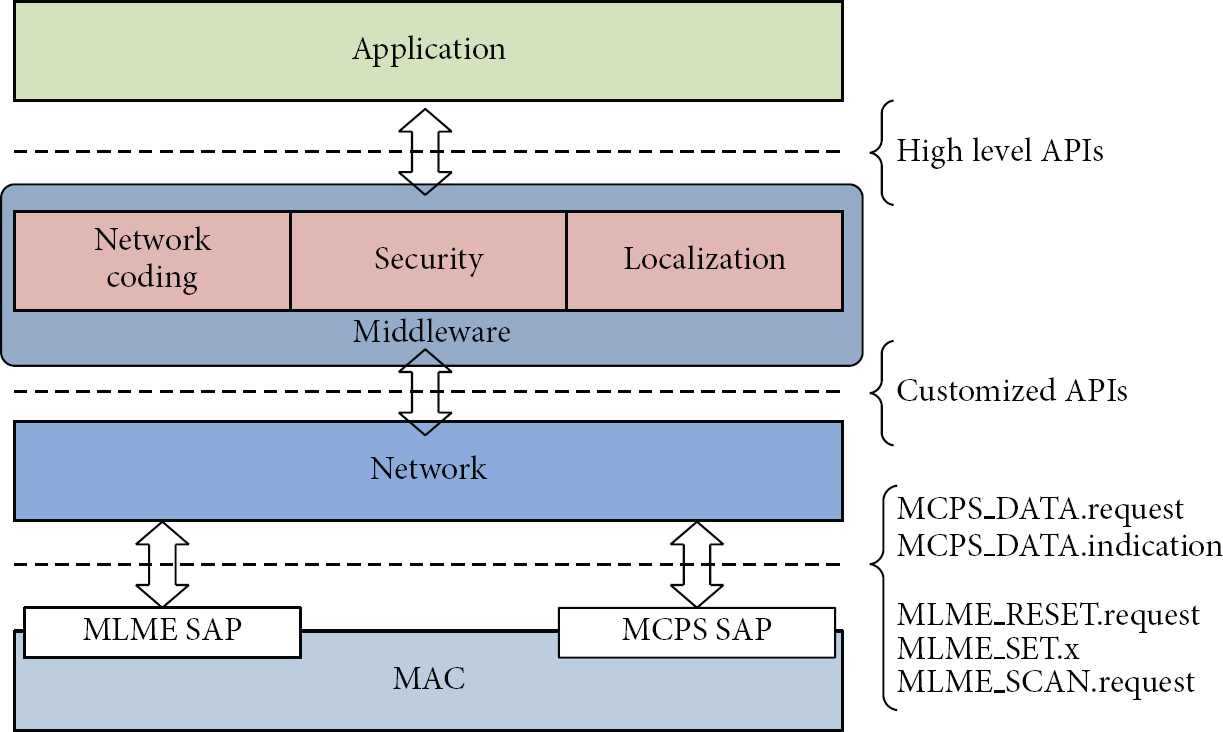
Communication protocol stack on top of the IEEE 802.15.4 standard. Basic interfaces are also shown.
(a) IEEE 802.15.4 MAC Layer. This layer is responsible for the access to the wireless medium for transmission and reception of the frames for both mobile patients and fixed relay nodes.
Among the options offered by the IEEE 802.15.4 standard [14], we have chosen to refer to the non-beacon-enabled mode, that is, the fully asynchronous mode. This choice is motivated by the fact that nodes can have variable duty cycle, especially the mobile ones, that is, those carried by the patients. In the classical scenario where patient's data need to be collected at a central station, the asynchronous mode offered by this standard allows for flexibility in accessing the medium only when patients' data are available and a transmission needs to occur. For the majority of time, the radio interface of these nodes can be kept off or in a low-consumption state to save the energy of the batteries. Moreover, the synchronous mode would have required association (and disassociation) mechanisms to allow the nodes to join the network prior to communication, resulting in a severe limitation on the nodes' mobility. Furthermore, to exploit the power of NC mechanisms for energy savings and network throughput gains (Section 4), messages sent by the mobile nodes need to be transmitted in broadcast, thus without a prior association mechanism.
Finally, along this line, the basic commands and events offered by the MAC to the upper layer are for packet transmission and reception and to set some specific parameters, such as the frequency channel and the transmission power, as well as the primitive to scan the IEEE 802.15.4 channels for energy and activity detection.
(b) Network Layer. Since the asynchronous mode of the MAC layer is chosen, this layer is responsible for keeping the synchronization among the fixed relay nodes. This is achieved by sending synch packets. Unlike IEEE 802.15.4 beacon frames, synch messages are not requested to be periodic: their transmission can be scheduled with an adaptive duty cycle, based on the environmental conditions (e.g., the presence of patients in the area or not), although for keeping their scheduling a mechanism inspired by the time division cluster scheduling [15] can be implemented.
Synch packets are fundamental to allow for minimizing the collisions among the messages sent by the mobile nodes, by defining a superframe structure constituted of time slots, where each mobile node is allowed to transmit, based on some policy rule. Finally, they are requested to implement both NC schemes and distributed localization algorithms, as will be detailed in the next sections.
Besides the synchronization, the network layer is also in charge of assigning the network addresses to the nodes. Usually, the radio interface of a node has an address which is worldwide unique as a serial number assigned by the manufacturer. In the case of IEEE 802.15.4 radios, these addresses are 64 bits long and can be used for the communication with any other node (extended address). Another option is for a node to get a network address, which is only 16 bits long, assigned according to some policy and used to communicate with the other nodes of the same network (short address).
Shortly, the extended address mechanism is used by the mobile nodes. The fixed relays are usually placed in strategic positions to ensure the best coverage of the environment and form a network with a static topology. Consequently, these nodes can be assigned with the addresses defined by, for example, the ZigBee Distributed Address Assignment Mechanism. This addressing mechanism assumes that nodes are organized into a tree and divides the address space into blocks, assigning each block to each node of the tree. The advantage of using short addresses in this way for the relay nodes is the fact that they do not need to maintain routing tables to forward incoming data: simply looking at the address, they are able to recognize if the packet has to be sent upwards or downwards along the tree. Finally, also packets to the mobile nodes are assumed to be sent in broadcast: this is still reasonable since it is assumed that the network traffic from the residential gateway to any patient (related to any actuation, such as, for example, automatic regulation of an insulin pump) is less frequent than the reverse direction (patient's monitored data collection).
The commands and events offered by this layer to the upper modules are customized based on the reference model we assume (ZigBee) with the addition of those elements needed to implement the services at the middleware layer.
(c) Middleware Services. This layer represents an interface between the underlying protocol stack and the application layer and is the core of the novelties introduced within the frame of WSN4QoL project.
The middleware encompasses three major blocks: (i) NC; (ii) distributed localization; (iii) security. These blocks exploit the services offered by the underlying protocol stack entities to provide a high-level application programming interface (API) to the application developers.
The NC entity is in charge of providing efficiency in wireless communications. By means of appropriate combinations of two or more packets into a single one and NC-aware routing mechanisms at the lower layer, a relay node is able to reduce the amount of traffic over the network, without losing data. Section 4 will present the basic building blocks developed within WSN4QoL to demonstrate the efficiency of a binary XOR-based network coding scheme in a scenario with two sources, one relay and one destination (i.e., a multiple access relay channel scenario), as compared to the case where the relay node simply forwards the received packets. In general, the proposed protocol stack allows for adopting multicast (and geographic) routing mechanisms at the network layer [16, Chapter 6] which are well suited for supporting NC schemes more complex than the binary XOR-based ones, including, for example, the random linear network coding (RLNC) [17].
The distributed localization block deals with the online estimation of the geographical position of a mobile node in the environment. Associating a spatial reference with every communication between the patients and the remote care givers is of paramount importance, whether in home or hospital environments, especially in case of alarms conditions. As better detailed in Section 5, the relay nodes emit their synch packets and doing so they play the role of anchor or reference nodes; that is, it is supposed they know their own position and they include this information in such packets. A mobile node is then able to estimate its own position by relying on the information gathered from the surrounding nodes.
The security block monitors the acknowledgement packets exchanged at the network layer among the nodes to identify potential threats or nodes malfunctioning and instruct the MAC layer to encrypt frames based on the security features offered by the IEEE 802.15.4 standard. Details about this block are out-of-scope of this paper, where the focus is switched to the other two elements, described in the next sections.
(d) Application Layer. This last layer mainly focuses on gathering measurements from the sensors and data compression. Although the WSN4QoL project also proposes low cost compress sensing techniques which exploit some key characteristics of the biometric data transmitted in order to provide energy-efficient telemonitoring solutions, this layer is out-of-scope of the present paper. Interested readers can find further details in our project website [6].
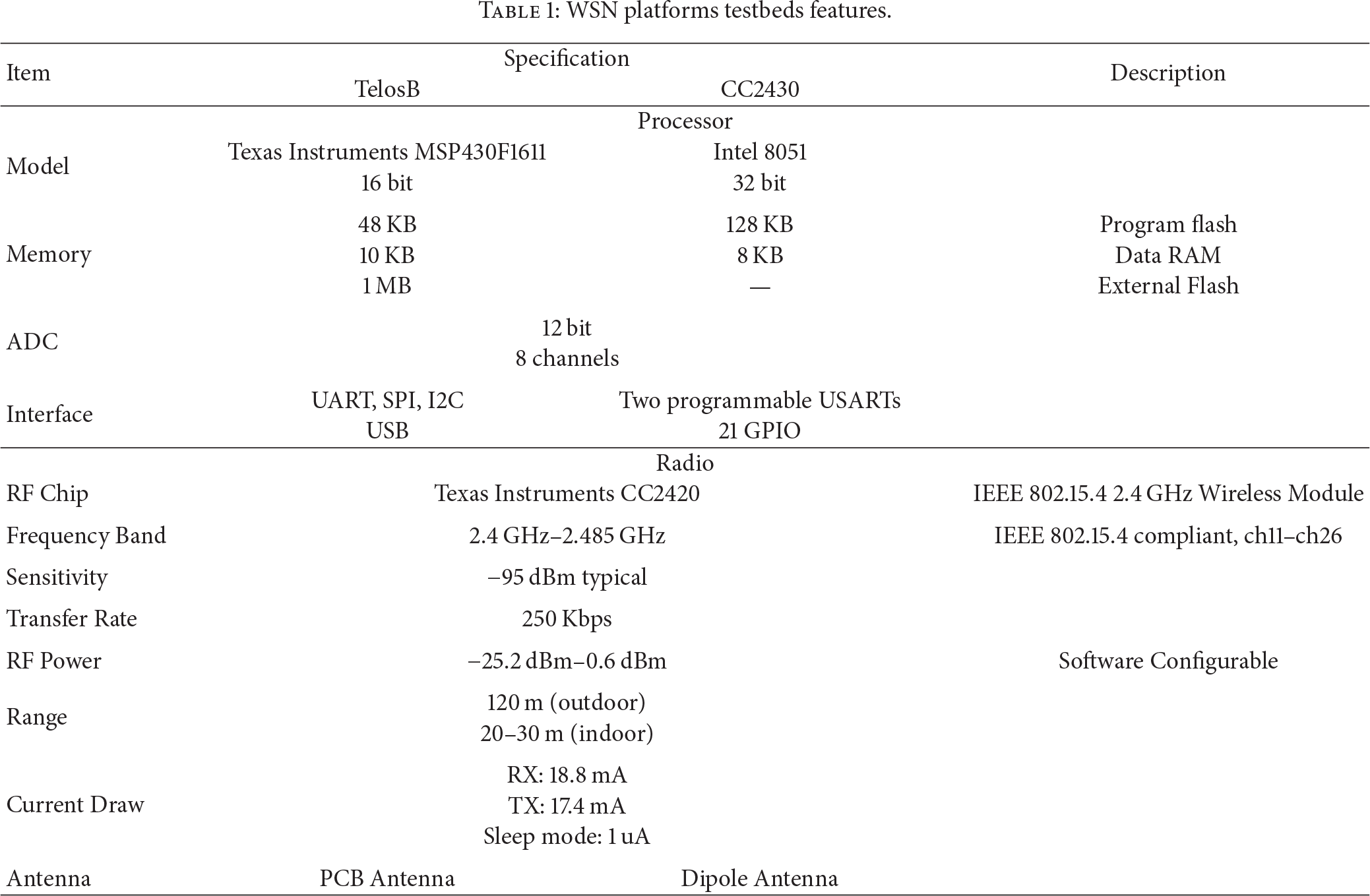
Next sections will present the implementation and experimental results of a binary XOR-based NC scheme and the distributed localization algorithm. Table 1 summarizes the main features of the WSN platforms used for the tests.
WSN platforms testbeds features.
4. Network Coding
To achieve efficient measurements reporting through the ambient relay network, the most viable solution is the application of NC techniques [18, 19]. In the preliminary implementation done in the frame of the WSN4QoL project, the scenario illustrated in Figure 3 has been implemented in the available testbed. In this scenario, two nodes A and B are mobile nodes carried by two patients; a relay node C has a fixed position and D is the destination of the measurements reports that are sent by the two source nodes. In the considered scenario, to further claim the gains introduced by the NC techniques, it is supposed that the destination node does not send back any feedback either to the relay or to the sources.

Scenario for efficient communications. Nodes A and B are mobile local hubs, node C is a fixed relay, and node D is the destination.
4.1. Implementation
Figure 4 presents the timings characterizing the scenario of Figure 3. In particular, Figure 4(a) presents the case of the baseline scenario and Figure 4(b) the case with NC.

Timings of the multiaccess relay channel scenario as depicted in Figure 3.
The relay C is responsible for defining the network scheduling among the source nodes A and B by periodically broadcasting the synch packets. The source nodes are programmed to send a message in their appropriate time slots; that is, node A sends its data after Tslot and node B sends its data after 2*Tslot. In the baseline scenario, node C then forwards the received data from A to the destination after Tslot and data from B after another Tslot; then it broadcasts a new synch packet and the process is iterated. In the NC scenario, instead of forwarding the two messages, the node C transmits to the destination a single message which is the combination of the two messages from A and B based on a binary XOR operation. In both cases, upon the reception of every synch, the destination checks what it has received in the superframe just concluded and updates the network statistics.
The main advantage of the NC against the baseline scenario is that the relay node forwards a single packet instead of two, resulting in larger energy savings and the higher throughput since the synch is sent every 4*Tslot instead of 5*Tslot.
Both scenarios have been coded and tested over a WSN testbed composed by TelosB nodes [20] (Table 1), programmed with the TinyOS operating system [21], and implemented as protocol layer(s) on top of the Official TinyOS 15.4 MAC [22, 23]. The nodes of the baseline scenario have been configured to run on the channel 25 of the IEEE 802.15.4 standard, while the nodes of the NC scenario run on the channel 26: this is done in order to have the two networks working at the same time and test them in the same conditions.
To monitor in real time the network behaviour and the performance, a graphical user interface (GUI) has also been implemented and is shown in Figure 5. It shows (i) the nodes' transmissions, (ii) the values of the sensors readings, and (iii) the residual of the batteries which are data encoded in the transmitted packets, as well as the performance metrics of the network including (iv) throughput or goodput (i.e., the amount of sensors measurements successfully delivered to the destination in the unit of time), (v) packet loss, and (vi) energy consumption.
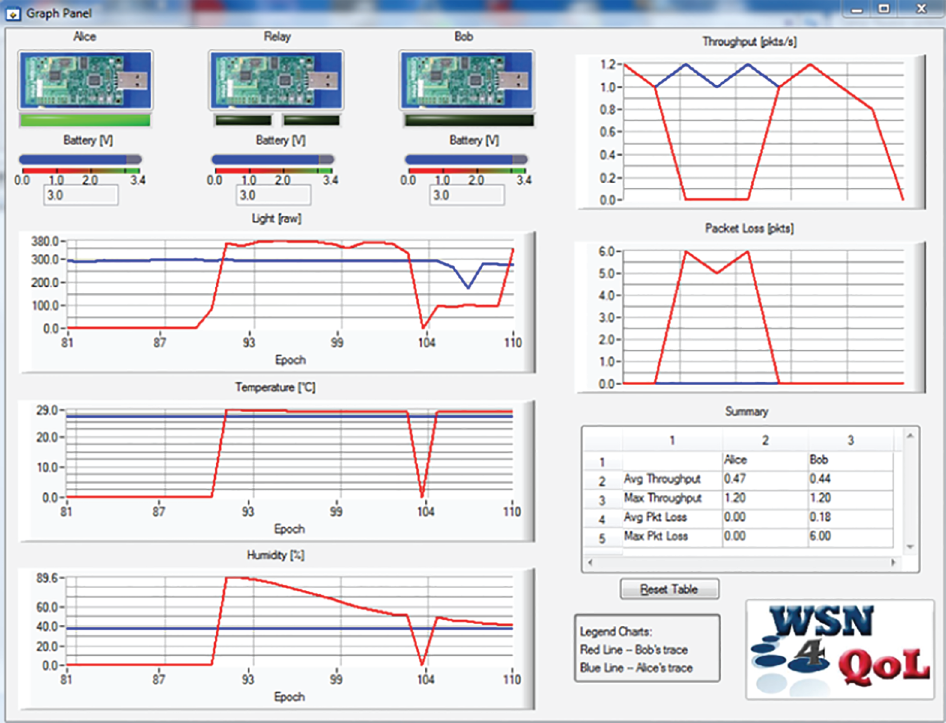
Graphical user interface to monitor network performance for network coding testbed.
4.2. Results
Compared to the classical relay scenario where node C forwards the received packets in two distinct slots, the NC scheme allows for achieving better performance in terms of joint packet loss ratio (PLR) and data goodput. In particular, the scenario of Figure 3 implemented on the mobile WSN testbed as described in the previous section was used in an indoor environment, such as a residential apartment, to run several tests by varying the transmission power levels between −25.2 dBm and 0.6 dBm. While source 2 nodes of both testbeds were kept in a fixed position, source 1 nodes of both networks were carried by a person who was walking at approximately constant speed over a preplanned closed path crossing the rooms of the apartment, resulting in a time of a lap of around 5 minutes and repeating the path at least 10 times for each experiment.
Although the PLR shows similar performance between the scenario with NC and the one with classical forwarding, the tests demonstrated that NC can achieve gains ranging from 32% to 68% in terms of instantaneous goodput. In particular, Figure 6 reports the goodput averaged over the whole experiments (i.e., all the laps for each transmission power) and for different values of the Tslot ranging from 200 ms to 800 ms (Figure 4). As it is evident, the NC shows always gains with respect to the baseline (relay-only) scenario for all the values of Tslot and all the transmission power levels. Moreover, analyzing the behavior with respect to the transmission power, both testbeds show similar performance and this further confirms that the two testbeds result in similar performance in terms of PLR.

Goodput comparison in multiaccess relay channel scenarios: with network coding and relay only.
Although in this preliminary testbed the simple XOR-based NC scheme has been implemented over a single relay scenario, future ongoing activities are focused on the enhancement of this mechanism in the cases where the ambient network is composed by several relay nodes, including multihop communications [24].
5. Distributed Localization
The aim of this section is to present the ongoing activity for indoor people localization in the WSN4QoL project. The algorithm we refer to is detailed in [25]. It is an anchor-based algorithm, which means it runs in a scenario where several fixed anchor nodes, that is, nodes knowing a priori their positions based on a common reference system of coordinates, are deployed in the environment and periodically broadcast their positions. A second set of nodes is mobile and called blind since they need to estimate their own positions according to the same reference system of coordinates, by relying on the data they are able to gather from the anchors and the environment. The algorithm is also range-based, since the blinds estimate their positions by first computing the distance with respect to the anchors available.
5.1. Implementation
Figure 7 shows a typical home environment where a set of anchor nodes are fixed and have been deployed in the rooms of the house. In such an environment a measurement campaign of the received signal strength (RSS) from the anchors in several points has been conducted, with the intention of building an RSS-to-distance relation curve, that is, an RSS-based ranging model used to estimate the distance between any pair of nodes from an RSS measurement.
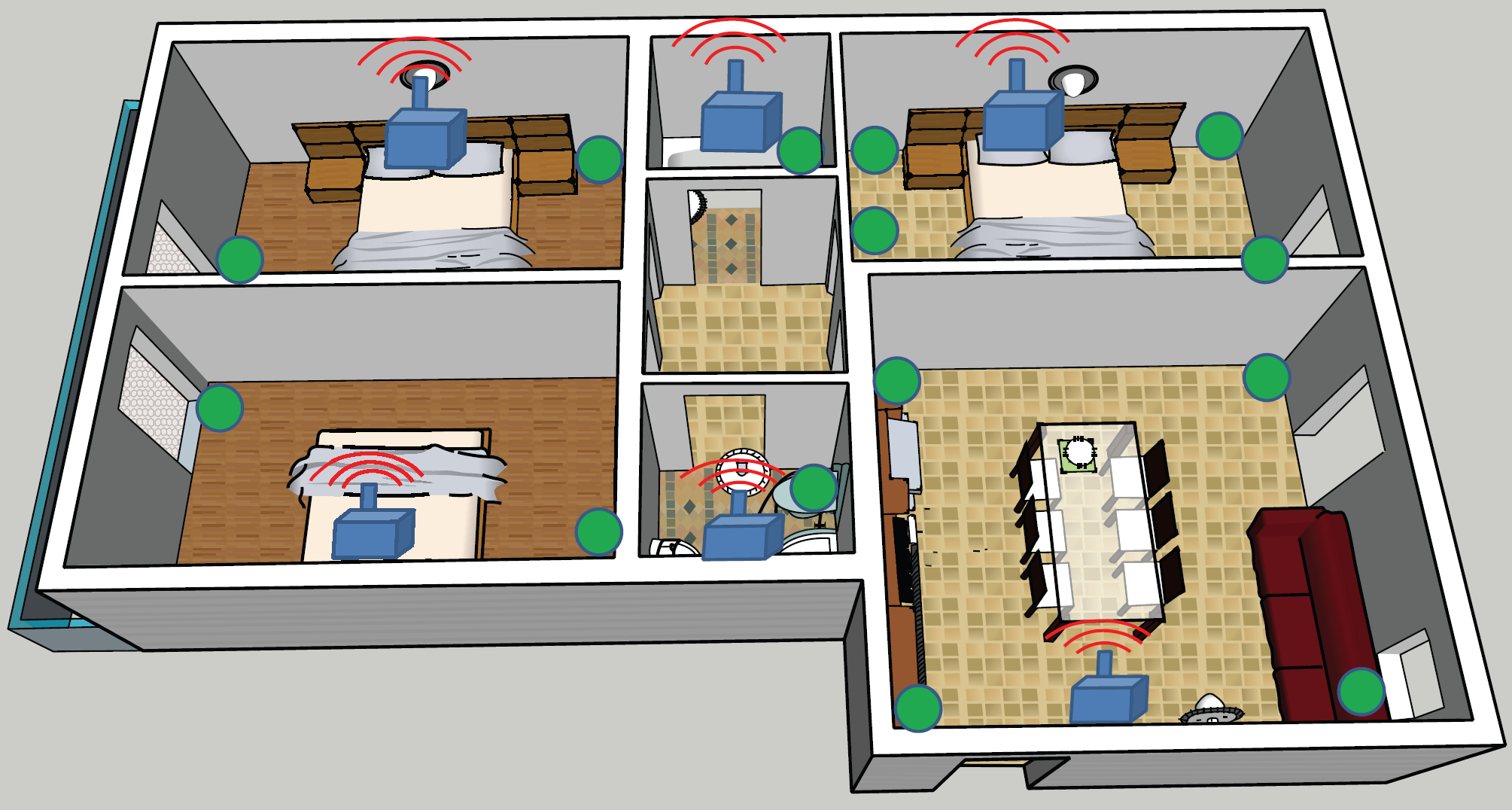
Indoor environment equipped with anchor nodes (blue squares) and RSS measurement points (green circles).
Typically, the calibration activity to compute the parameters of the model is performed offline and in a static context; then the system needs to run in an environment which is more dynamic, for example, with people moving around or changes in the furniture and so on. As a consequence, RSS propagation parameters are strongly environment dependent and usually show big fluctuations, which suggest that using any fixed and outdated estimate for the channel parameters certainly yields less accurate estimates of distances and thus of final positions. To cope with this problem, an anchor-aided dynamic and adaptive estimation of the signal propagation parameters has been previously proposed and can be easily implemented [26] as shown in Figure 8.
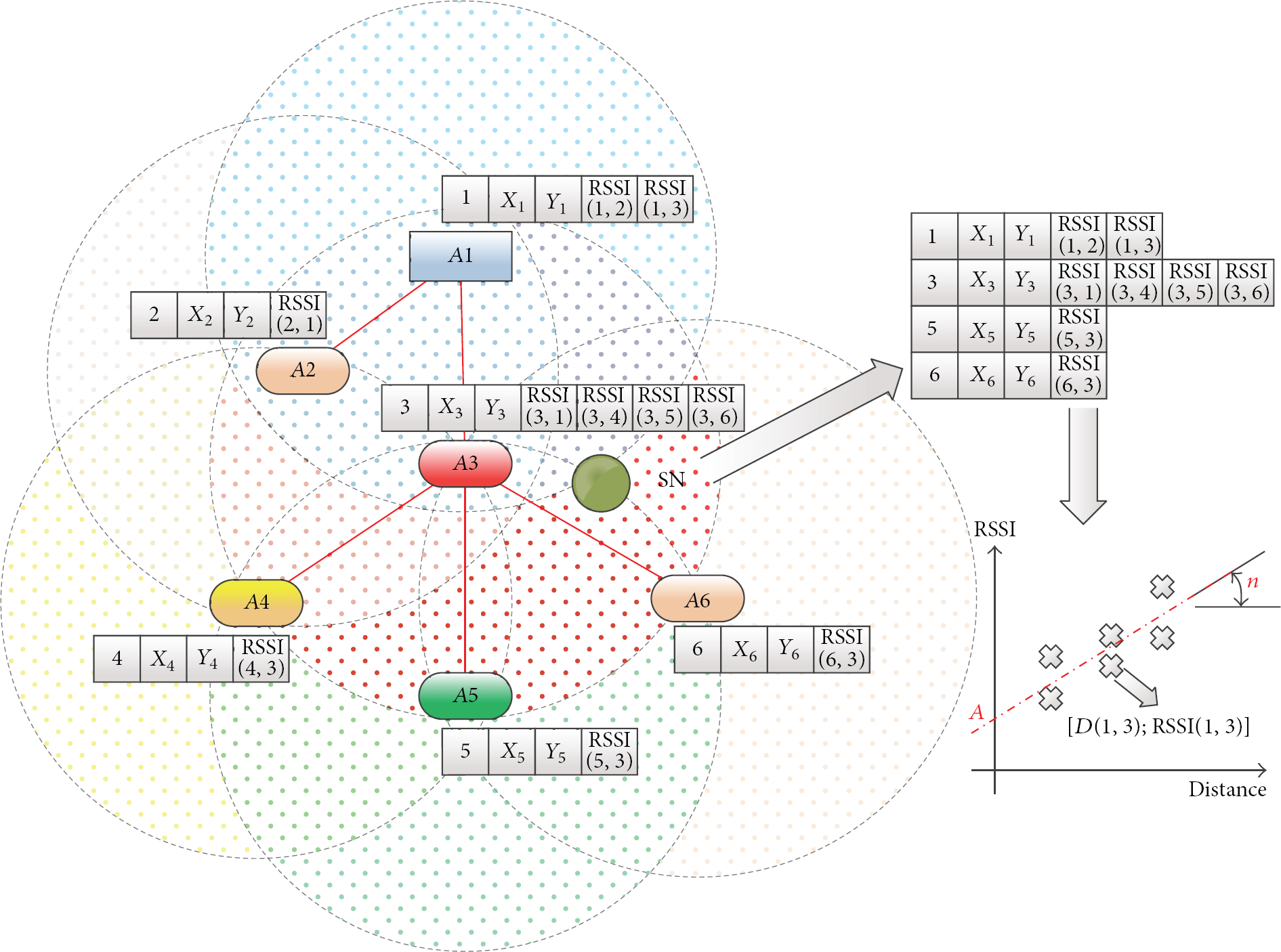
Anchor-aided dynamic and adaptive estimation of the ranging model.
In particular, the relays-anchors put in the synch packets the RSS received from other anchors in their communication range. Figure 9 shows how the IEEE 802.15.4 data frame is used for the anchors to transmit their positions, including also the RSS data needed for implementing the dynamic and adaptive ranging model estimation.

IEEE 802.15.4 data frame used by anchors with localization-oriented payload.
Every mobile node in the area receives these packets and is then able to correlate the distance among the available and known anchor nodes with their respective RSS so that the ranging model can be reconstructed as formulated in [26].
The implementation has been done on TelosB nodes [20] running the TinyOS operating system [21] for the anchor nodes and an IEEE 802.15.4-compatible platform for the mobile node, such as the Texas Instruments CC2430 [27] which has the same radio interface of the TelosB nodes (Table 1).
Similar to what has been done for the NC testbed, to monitor in real time the network behaviour and the performance, a GUI has been implemented and is shown in Figure 10. It allows for configuring at deployment time the position of the anchor nodes and then shows (i) the nodes' activities, (ii) the residual of the batteries which are data encoded in the transmitted packets for every node, and (iii) the statistics of the localization estimations for the mobile node such as (iv) instantaneous position estimation, (v) covariance ellipse (with a 70% confidence interval) of the last 5 estimations, and (vi) the ranging parameters estimated by the mobile node.

Graphical user interface to monitor network performance for Localization testbed.
5.2. Results
Figure 11 presents preliminary results of the localization of a blind node placed in several points in the environment of Figure 7. The blind node has been left in each position for 5 minutes, resulting in at least 100 localization estimations.
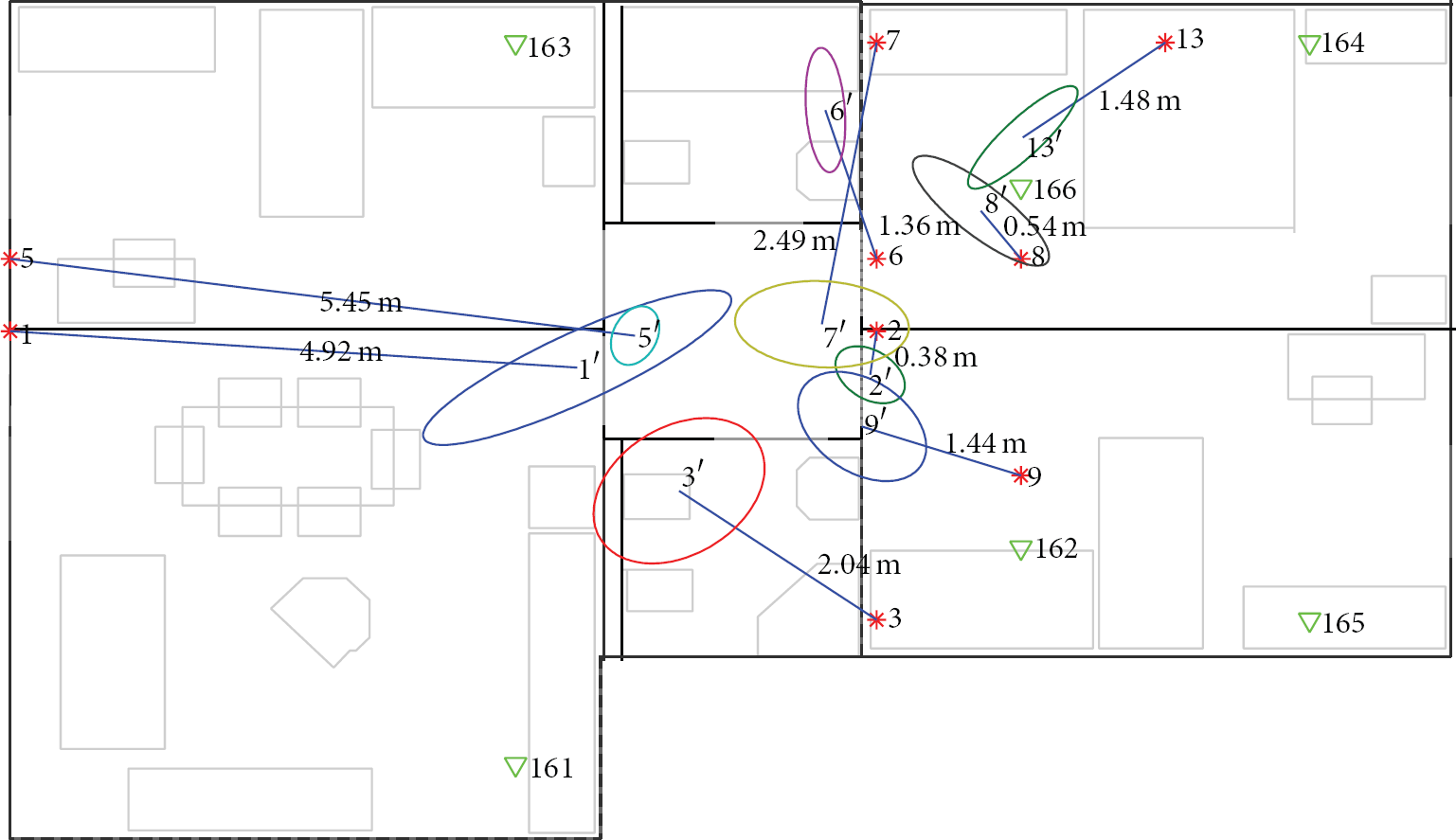
Localization results in the scenario of Figure 7. Average localization errors and covariance ellipses are also shown.
It is evident that better topological conditions (i.e., where surrounded by the anchors) lead to better localization accuracies and stability (i.e., little average errors and low variability among estimations). Overall, the average localization error over the area of 60
6. End-to-End Solutions and Testbeds
After having presented the solutions proposed within the WSN4QoL project, this section overviews the state of the art in the field of WSN-based systems for pervasive healthcare applications, pointing out the main innovation aspects that the WSN4QoL project proposes.
6.1. Motivation
Before proceeding to give an overview of the solution and testbed in literature, an interesting vision of e-Health remote monitoring systems as given in [29, 30] is worth mentioning. In these works, authors classify the telecare applications as an instance of the broader cyber physical world (CPW), where a tight integration of sensing, computation, and communication elements concur to the definition of the system. In this line, several exciting research challenges and opportunities arise and might stimulate new research activities in the emerging areas of CPW convergence.
In general, nowadays, these technologies still require the development of reliable, scalable, and evolvable systems in various application domains. They should hide unnecessary complexities inherent to CPW, such as heterogeneity and distribution, and support rapid implementation of application and runtime reconfiguration and resource management to meet functional and nonfunctional requirements. One of the key elements focuses on the study of methods and techniques that can be used to investigate the structure and evolution of the dynamics of human behavior under the lens of pervasive computing. In this perspective, the sociotechnical nature of the CPW convergence calls for novel and interdisciplinary research approaches mixing ICT (information and communication technologies) expertise with lessons learned from applied psychology, sociology, medicine, complexity science, and so forth.
Along this line, wearable computing (WC) for remote assistance is one of the best examples where this multidisciplinary approach takes the most promising advantages. The maturity of WC can be demonstrated by several projects showing its main application domains. Monitoring the wearer's vital signs promises improved treatment and reduction of medical costs. Many projects are aiming at a preventive lifestyle and early diagnosis, by focusing on the integration of healthcare more seamlessly into everyday life.
Nevertheless, [29] stresses the fact that several research challenges have still to be met in this field. In particular, the large-scale production of smart clothes requires scaled-up manufacturing processes to exploit economy of scale effects. In addition, web-based data gathering methods (e.g., [31, 32]) are supportive in fusing heterogeneous sensor modalities and in the automatic annotation of data streams. Moreover, major challenges arise for data privacy and security in designing algorithms and protocols to protect the sensed data against unwanted collection and distribution of personal information.
The work in [33] summarizes the most recent developments in the field of wearable sensors and systems, relevant to the field of health and wellness, safety, home rehabilitation, assessment of treatment efficacy, and early detection of disorders. The integration of wearable and ambient sensors is discussed in the context of achieving home monitoring of older adults and subjects with chronic conditions. Particular emphasis is given to the analysis of the key enabling technologies to broaden the wearable systems for patients' remote monitoring. Among these, we underline the new advances in the sensors miniaturization's technologies and low-power microcontrollers and radios, which can be integrated into system-on-chip implementations and enable e-textile based systems (such as [34]) or unobtrusive wearable devices (such as [35]). Mobile phone technology played the major role in the pervasiveness of remote monitoring systems, since smart phones are broadly available and easily act as information gateways to central stations through mobile telecommunication standards such as 4G. Moreover, mobile devices can also function as information processing units. Reference [33] concludes that the past and ongoing research toward achieving remote monitoring of older adults and subjects undergoing clinical interventions will soon face the need for establishing business models to make them effective in the market to cover the costs. However, we believe that also a new area of research should involve the definition of new communication standards for the interoperability among the plethora of authorities, as stressed by similar other surveys, such as [36].
On the other hand, [37] presents a range of wireless communication technologies and standards (i.e., IEEE 802.15.1 Bluetooth, ZigBee/IEEE 802.15.4, Ultra-wide-band (UWB), medical implant communication services (MICS), and IEEE 802.15.6 Task Group). It lists their current limitations, by dividing the platforms into implantable and on-body devices. In particular, the integration of wireless technologies into medical devices, such as insulin pumps and on-body cardiac monitoring devices, has many benefits, but also poses many challenges, including (i) enabling the secure transmission of the collected private data, (ii) prevention of electromagnetic interference between different wireless devices and compatibility with the remaining circuitry, and (iii) compatibility with, and safety of, the biological tissues. In this perspective, although security and privacy are well investigated in the literature and well taken into account in the projects, we believe that the latter two issues are still too often widely neglected. Of particular interest is the constraint posed by the last one. Besides the power and small size requirements, implantable devices also need to be compatible with biological tissues in order to prevent possible infection and rejection of the device by the biological tissue. Compared to implantable devices, on-body devices are less prone to the biocompatibility constraint. However, it is worth noting that also in this case long-term skin contact with such devices can cause different forms of skin irritations. Thus, on-body devices should also either be developed with biocompatible materials, or be truly noninvasive, where no skin contact is required for the acquisition of the desired data.
6.2. Testbeds
The authors in [38, 39] provide two examples of ECG telemonitoring implementation testbeds. Reference [38] focuses on the extension of the Standard Communication Protocol for Computer-assisted Electrocardiography (SCP-ECG), which provides standardized communication among different ECG devices and information systems, to be included in health monitoring systems. The paper describes the implementation of the new protocol as a software component in a five-month pilot period of health telemonitoring system (HTS) including 27 patients. The testbed they used to show the feasibility of their proposed enhancements includes all the elements of a telecare system. In particular, a wearable data acquisition system, consisting of several sensors (e.g., ECG, NiBP, SPO2, Pulse Rate, Temperature, and PLE), is equipped with a Bluetooth radio, a GPS receiver, and a personal digital assistant (PDA) with mobile ADSL capabilities. The PDA automatically organizes the data gathered from the sensors and other information manually inserted by the user into the data structure defined by the protocol. A remote health monitoring system (RHMS) is implemented on a PC on the expert's site and is able to store, present, and process the acquired data from the PDA. The PDA communicates with the RHMS using fixed and mobile ADSL.
Although the suitability of the protocol has been clearly shown, security aspects are merely taken into account by the use of data encoded transmissions, while user identification of the involved people (i.e., individuals, technicians, physicians, etc.) is performed through a simple log-in screen requiring user ID and password.
On the contrary, [39] explicitly focuses on the implementation of security techniques in similar ECG-based telecare applications even if the scope of the paper is limited to the sensing device. Namely, a secure cross-layer-based miniaturized BSN platform has been developed. It consists of a processing unit and a radio transmission unit with a sensor board and a local battery power supply or energy scavenge supply. The design of such platform puts particular emphasis on resource-awareness; that is, it adopts a joint unequal resource allocation (i.e., transmission power and data rate) and real-time selective encryption, according to the channel status.
In [40] a body posture model and an unsupervised learning and clustering algorithm have been proposed to reconstruct different stationary postures. An extensive validation has been performed through a BSN composed by Freescale nodes [41] equipped with 3-axis accelerometers. These nodes are firmly attached through bands to four limbs to measure the posture of arms and legs, with two accelerometers on each limb, and report through a wireless single-hop ZigBee radio the measurements to a central station. Experimental results demonstrate that the proposed system can achieve very high classification accuracy and is able to recognize complicated stationary postures.
The authors in [42] use a pair of Shimmer motes [43]. Shimmer is a wireless sensor platform programmed in TinyOS [21], characterized by a small form factor, that can record and transmit physiological and kinetic data in real time using the most well-known communication technologies, such as Bluetooth or IEEE 802.15.4. The chosen device incorporates a triaxial accelerometer, a microcontroller, and an IEEE 802.15.4 radio transceiver. One mote is used as a wearable device while another is attached directly to a PC acting as a base station. Since the proposed method to extract features from acceleration measurements is not computationally intensive, the filtering technique has been implemented directly on the wearable device in order to communicate with the base station only when alarms occur and then save batteries.
In a slightly different scenario, that is, military missions and monitoring of soldiers, the contribution of [44] is the concept and implementation of a closed-loop, end-to-end, real-time on-body prediction system for reducing health risks due to uncompensable heat stress (UHS). This involves gathering physiological data (multipoint skin temperature) and postural information (multipoint body acceleration) for the purpose of autonomous real-time modelling and prediction. One of the central concepts driving this system development is that data processing must be performed by system devices mounted on the body to achieve a better real-time closed-loop control. Autonomous operation is essential because a long-range radio link to a central location might not necessarily be available. A relatively powerful hardware platform is thus required to support real-time on-body data processing, which also enables two control loops. An inner loop implements local actuation, namely, notifying alarms to the user or automatically taking some actions such as cooling the body. An outer loop involves the communication with a remote station for, for example, mission plan change or the return to the base to install new cooling systems. Similar approaches can be easily implemented in more traditional civil scenarios for remote patient monitoring.
Another simple yet efficient Internet-based telecare remote monitoring system is presented in [45], where the focus is on a remote-controlled home mechanical ventilation (HMV) system, which is progressively being used to treat patients with severe chronic respiratory failure. Contrary to the most conventional settings, the system designed avoids any high order information technology architecture. It is based on a simple and low cost data transfer server (DTS) that grants the Internet connection to most commercially available ventilators through the GPRS network. The device captures ventilation signals (e.g., pressure, flows, volume, leaks, and oxygen saturation) and controls the ventilator settings. The DTS is built upon an embedded system board (a Linux-enabled FOX board [46]) equipped with a GPRS modem and a commercial USB flash memory. It operates as a web server with its own address and password. With such an approach, an independent point-to-point (from patient home to HMV provider) communication is established. Therefore, the HMV provider (being a hospital service or a private practice physician) can receive real-time or previously recorded ventilation data in uplink and modify the settings in downlink by simply connecting, via Internet, to the individual web address of the DTS at the patient's home, ensuring this way the closed-loop control.
A remote and mobile patient monitoring service architecture using heterogeneous wireless access in which each patient is equipped with a remote monitoring device with a heterogeneous wireless transceiver is presented in [8]. While the system architecture is not a novelty, since authors propose that a mobile patient can use different types of wireless technologies (e.g., WiMAX-based WMAN and WiFi-based WLAN technologies) to transfer monitored biosignal data to the healthcare center, the most innovative aspect in this contribution is the formulation as a constrained Markov decision process (CMDP) of the problem on the e-Health service provider side, who has to pay to the wireless network service provider a certain number of connections to be reserved for the patients. Using stochastic programming techniques, the optimal number of reserved connections can be determined to minimize the cost of the e-Health service provider under randomness of connection demand due to the mobility of the patients. Also, at the patient-attached device, the transmission scheduling of biosignal data with different priority is optimized to minimize the connection cost and satisfy the delay requirements.
In the frame of coupling wearable BANs with classical WSNs for environmental monitoring, [9] presents a study of a healthcare architecture for monitoring elderly or chronic people in their residence. Figure 12 sketches the reference network architecture, where wearable sensor system (composed by a single belt of sensors) communicates with powerful mobile computing devices through Bluetooth and the wireless sensor network through ZigBee. The higher part of the architecture includes communication technologies such as cellular-based networks and WiFi (or even WiMax). Although similar to WSN4QoL's reference scenario sketched in Figure 1, this architecture differs from that since patients sensors and ambient living WSN nodes form two distinct subnetworks. Nevertheless, as in WSN4QoL, the study involves a real implementation of the proposed architecture in different scenarios, including nursing-house, home, and hospital environments. Besides the security aspects related to the communication of patients' data, the paper shows that the architecture is flexible enough to allow for querying the fixed wireless sensor network nodes and the mobile BANs over heterogeneous communication technologies. Authors also stressed that a tighter integration between the wireless sensor network and the wearable systems can be achieved through the use of 6LoWPAN technologies and that biomedical sensor positioning would be crucial to detect the location of people at any place and any time [47].

Healthcare system hierarchical network architecture in wireless sensor networks [9].
In this line the work of [10, 48–50], where the paradigm of the Internet of Things, that is, 6LoWPAN, is applied to healthcare and BSN systems, is worth mentioning. In particular, while [47] focuses on simulation results to assess the performance of a proposed distributed handover procedure to support body sensors mobility and continuous access, in the other papers, preliminary implementations approaches in TinyOS [21] are illustrated with particular emphasis on handling mobility and inter-BSNs communications.
Achieving location of the patients is one of the goals of the work presented in [10] and sketched in Figure 13. In this paper, however, it is supposed that a wearable system built upon smart shirts, such as, [34], is completely hardware-independent from the positioning subsystem built upon devices that each patient is also supposed to carry. Both subsystems communicate with an IEEE 802.15.4-enabled wireless sensor network acting as distribution network between the terminals (patients) and the gateway to the public Internet-based network. Once again, however, the two subsystems (sensor measurements reporting and patients' localization) are independent of each other, while in WSN4QoL the goal is to make them converge into a single network able to support different services simultaneously. The prototype has been implemented and tested in a real-world scenario within hospital facilities by equipping up to ten patients with this equipment, and positive feedback was received by the hospital personnel, paving the way to future applications.
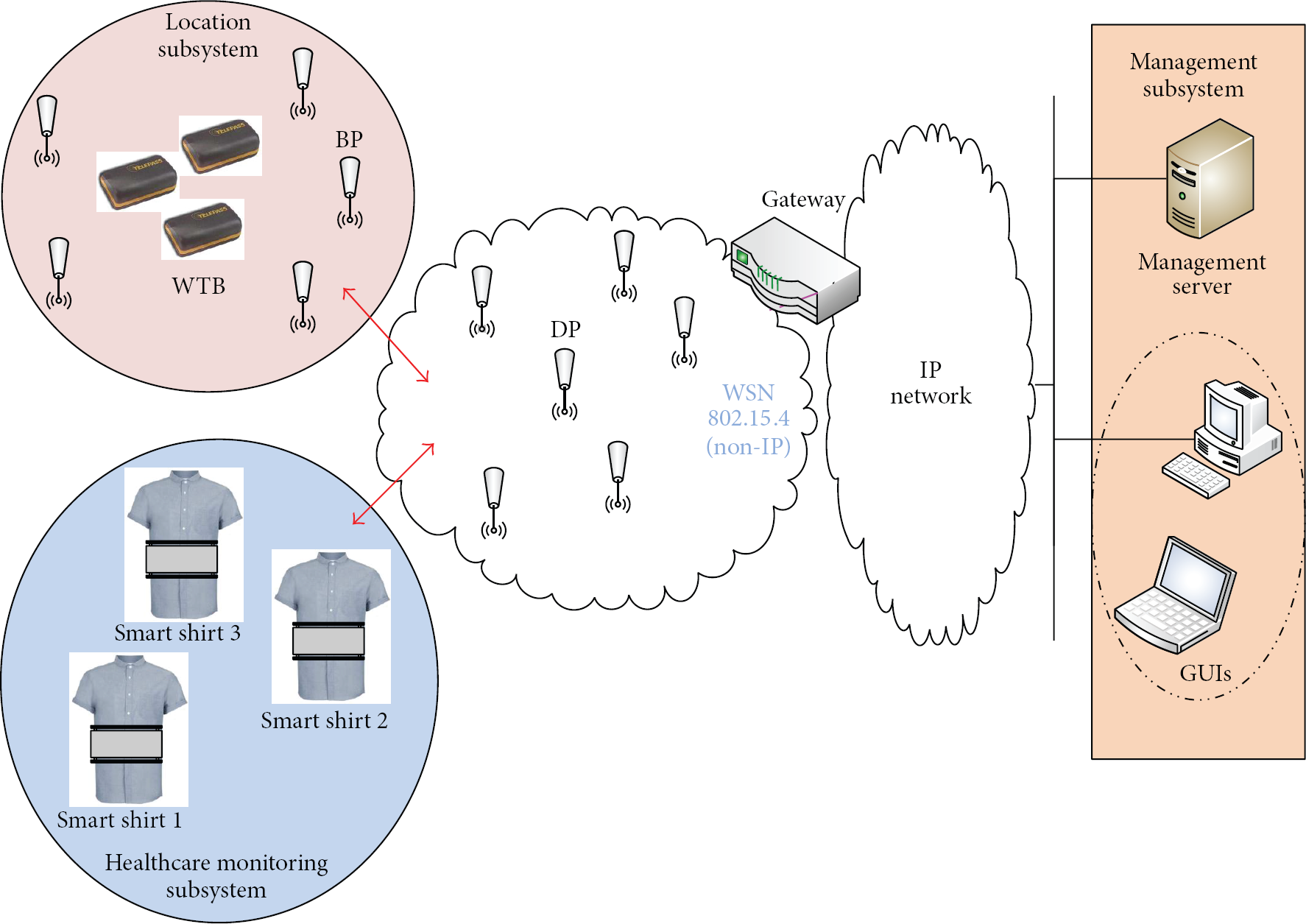
Healthcare monitoring and location systems [10].
The two-tier architecture is also the basis to the work presented in [51, 52], where scalability performance is evaluated considering the IEEE 802.15.4 at the lower tier and WLAN/IEEE 802.11 at the upper tier of a healthcare monitoring system. End-to-end packet delay and packet access time to WLAN have been evaluated as a function of the number of concurrent BANs (up to 50). Authors claim that there is need for choosing carefully network parameters, because the interaction of high-data-rate streams, such as EEG, with lower-rate streams, such as EKG or blood pressure data, causes some unwanted effects on the packet jitter of the latter. Moreover, in [53] an overall comparison between GPRS and WLAN communication technologies for the higher tier of the system architecture is presented. The study clearly shows that GPRS and WLAN have complementary power and delay profiles: GPRS has lower power consumption to keep network connectivity and send data, but delays might be high, whereas WLAN has higher energy cost but lower delays. Finally, the paper [54], where a mapping of the quality of service requirements for e-Health on the QoS classes of 3GPP networks is presented, is worth mentioning.
A different technological approach is pursued in [55, 56]. In this work, to solve the issues related to RF interferences, authors investigate the potentiality of using infrared communication for data transmissions in mobile healthcare contexts. Simulation of scenarios of line of sight and diffuse configurations show that it is theoretically possible to achieve optimal outage probabilities with very low transmission power, which would help improve the energy efficiency of such systems. However, although promising, these results need to be confirmed by experimental trials, still far to be achieved.
7. Conclusions
In this paper, the WSN4QoL project has been described with particular emphasis on its challenges and objectives in the area of proposing efficient WSN-based solutions for pervasive healthcare applications. NC techniques and distributed people localization mechanisms have been implemented on real WSN testbeds. Preliminary tests in real working environments gave promising results, in line with our expectations.
Future work will include the implementation of the proposed solutions in real medical devices, as well as repeating these tests on a larger scale testbed. Overall, we believe that the intelligent implementation of the solutions proposed in a self-organized WSN will pave the way for a pervasive healthcare system that is free of economic burdens and is able to focus on the real needs of patients regardless of their age span.
Footnotes
Conflict of Interests
The authors declare that there is no conflict of interests regarding the publication of this paper.
Acknowledgments
This research was supported by the European Commission under the Marie Curie IAPP WSN4QoL project, Grant no. IAPP-GA-2011-286047. An earlier version of this paper appeared in the Proceedings of the IEEE 15th International Conference on e-Health Networking, Application & Services (HealthCom), 2013 [![]() ].
].