
Abstract
Advances in healthcare applications benefit the scenario of medical service provision for both care staff and medical institution than ever. Following such success, a healthcare system, named RCTC (Resident Classification by Types of Care), which grades individuals in terms of the severity of five functional status assessment aspects: mental, movement, eating, toilet (urination and defecation functions), and medical treatment, was developed in this study. This system is designed based on a conceptual model that follows the assessment/classification/placement sequence for long-term care institutions. It is implemented to deliver appropriate services according to individual needs based on its preprocessing of classification and further reduces the costs of manpower and loading of care staff through the analysis of assessment logs. With this systematic appraisal, this system can not only help care staff determine the needs of residents but also produce personalized health plans (i.e., weekly schedule towards comprehensive assessment and personalized care services). Results of implemented (and in use as well) system have demonstrated the feasibility that it can enhance the quality of care services to residents, working load of care staff, and efficiency of care-related information management for medical institution.
1. Introduction
Health information technology (HIT) can reduce mistakes of medication or diagnosis, help medical professionals to obtain patient information in a timely manner, shorten their waiting time, and improve care quality and efficiency [1, 2]. Currently, HIT has been widely applied in health care industries. For example, the common HIT systems can help practitioners to input medical advice, track patient status, and record prescription and medications. Electronic medical records can keep patients’ personal health records, including medical records, inspection reports, and medical images [3], and a standard transmission format has been established to enable cross-hospital delivery. For patient safety, computer-aided diagnosis and treatment planning have been used to avoid failure to diagnose and improper treatment. One study explored the debate and initiatives concerning the use of HIT in health care in developing countries and discussed the main advantages, limitations, and perspectives [4]. Long-term care (LTC) institutions have lagged behind other settings in adopting HIT. Two early studies for resident classification were developed to improve placement decisions and to provide information for resource placement in LTC institutions [2, 5], but these systems lacked HIT support for comprehensive resident assessment. Several studies have presented factors that affect electronic health record (EHR) adoption in LTC institutions [6] and provided descriptions of the early users’ experiences with EHRs in LTC institutions [7]. A recent study [8] examined the adoption and utilisation of EHRs in LTC institutions and identified the barriers preventing the implementation of EHRs.
Assessment of the needs of healthcare [9] is the most important task for LTC institutions. The care staff should know the overall functional status of residents before providing required care services. Any assessment of LTC residents must be multidimensional and comprehensive enough to measure all health-related aspects of residents [10]. To assess care needs, Japan uses the care needs certification scale [11] to assess body function, actions in daily life, living function, cognitive function, behavioural and psychological symptoms of dementia, social adaptation, medical use over the past fourteen days and independence in daily life, which are classified into seven levels according to care needs. Germany uses ADLs and IADLs [12] as assessment tools. These tools are classified into three levels of care needs in terms of care time needed. Korea employs quantised ADLs to assess care subjects, which is classified into three ranks. The above assessment tools could be used for the general populace but are not widely used for LTC residents because they cannot meet the needs of residents with cognitive functional disorders. For this population, the International Classification of Function, Disability and Health (ICF) was published by World Health Organization to standardise descriptions of health and disability and can be used to assess residents’ cognitive function using the ICF and its qualifiers [13].
In relation to the fee schedule of LTC institutions, the Minimum Data Set 2 (MDS 2) [14] is the mandated assessment tool in American nursing homes. MDS 2 lists 18 risk assessment items and assessment criteria in total. The Resource Utilization Groups III (RUG-III) [15] case-mix system provides resident-specific means of allocating resources based on the variables of care costs for residents with different care needs. RUG-III uses a large number of rehabilitation-related and medical-care-related explanatory variables, and it is followed by the Japanese LTCI classification system [16]. A TAI-based system [17] was designed mainly as a resident management tool and includes variables related to the resident's functional status. Researchers [18] proposed RUG-III and a Japanese classification system for LTCIs. Their system contained rich medical explanatory variables and explained total medical cost better than the classification in a case-mix system. However, even medical components had a positive effect on explanatory power; the use of medical-needs-related variables will increase the complexity of a classification system, consequently restricting their utility to fee schedules. Okochi and Takahashi suggested that a simpler coding system, such as a TAI-based system, will be helpful to improve resident management and to represent the practical care needs of the residents.
Without the aid of a software system, the types of care classification and care needs assessment are difficult to achieve because the assessment content mainly comprises complex health conditions and care needs. The assessment criteria also differ from each other for different assessors. Most previous researchers [19–22] would refer to the content of MDS when developing comprehensive care need assessment tools. Most software developers would also apply MDS as the assessment scale for the assessment package. These software packages offer a variety of features beyond data entry, including functions to help facilities support care tasks and improve efficiency in meeting multiple reporting requirements. However, the entire assessment process of these systems is complicated and time consuming, which is not suitable for Taiwan's institutions. By referring to a TAI-based system assessment content, we designed the RCTC system based on a conceptual model that follows the assessment/classification/placement sequence for LTC institutions. This sequence can be designed to resemble the sequence of tasks carried out by practitioners in the institution, and it can accommodate advanced HIT features that integrate the RCTC system with this sequence to enhance the institution administrator's ability to assess and provide resident care needs, track the quality of care service, make resident placement decisions, and monitor multiple performance indicators for the institution.
In Taiwan, there is intensive debate about LTC insurance [23], and however, there is no unified standard for resident assessment, so the institutions lack useful resident needs assessment tools to deliver personalised care. Taiwan is still in the preliminary stage of employing HIT to help provide proper care services for the residents of LTC institutions. Currently, data processing tasks are mostly still performed manually or semimanually. Some commercial LTC systems are designed as general electronic forms packages. Therefore, we developed the RCTC system to help care appraisers to assess residents’ overall functional status, required care needs, care methods, and estimated care time. This pilot study of the RCTC system cooperated with an eighty-eight-bed LTC institution. This institution belongs to a health service company. The health service company provides personal LTC service and owns two regional hospitals and five LTC institutions. We gathered current resident care methods, assessment tools, care-related records, and resident assessment procedures for this study. The care staff also offered professional knowledge for this project.
The objectives of this study are the following:
building up a resident assessment system for LTC institutions with a classification and grading concept, developing a RCTC system to automatically generate personalised care plans and weekly healthcare schedules for individual residents in the institution, improving effectiveness in management of medical institution, healthcare quality [24, 25] for residents, and working efficiency of staff.
2. Classifying Residents by Types of Care
Traditional pigeonholed resident placement constitutes a depersonalised care service and is deemed not socially acceptable [26]. Classifying residents into categories by their care needs would be useful for resident placement decisions and would reflect humanistic considerations. Residents would receive appropriate care service, which would be helpful for the improvement of care quality. The classification concept was based on the premise that the care staff should provide residents with the right care services at the proper time using the most economical means, which can be achieved through the use of reasonable assessment procedures for the classification of residents according to their care needs. Thus, the placement of residents into appropriate districts with proper care plans would help residents to live at their maximum potential with the acceptance of care services.
The RCTC system was designed mainly by referring to the TAI [15] (Typology of the Aged with Illustrations) scale's classification and grading concept. We modified some of the items of the TAI assessment instrument to better fit the Taiwanese population. Figure 1 shows the proposed conceptual framework of the RCTC system. The RCTC system as a whole includes a basic resident database, assessment module, care plan module, weekly care schedule module, and management module. Because the care services are different from those of the traditional HIT system according to the five functional status assessment aspects—mental, movement, eating, toilet (urination and defecation functions), and medical treatment—the RCTC system can automatically compute the care needs and form personalised care plans and weekly care schedules for residents. Thus, the care staff can implement more flexible care services for individual residents compared to traditional care plans. As for the weekly care schedule of the residents and the number of residents in specific categories in the institution, the LTC system can be implemented in accordance with the estimated resources, such as reimbursement, bed placement, staff assignment, and maintaining proper staffing ratios, to enable effective management and operational efficiency.

Conceptual framework of the RCTC system.
The resident assessment procedure first evaluates the care needs and then classifies residents into categories of types of care. After assessment, three types of care and seven care grades are possible. Each element starts with mental status, which is mainly used to assess cognitive function, including verbal functions and language skills, concept formation and reasoning, perception, orientation, and attention. The functional levels are graded in light of cognitive disorders. In terms of movement, the assessment mainly considers the ability to complete daily activities independently, including personal hygiene, dressing and undressing, medication usage, and shopping. The worst situation is that the resident is unable to turn over in bed by himself/herself. In terms of eating, the assessment mainly considers the ability to perform actions related to eating, including if the patient can eat by himself/herself, if fixed dishware is needed, and food type. The worst situation is that the patient has to be fed by nasogastric tube or receive nutrition through intravenous injection. In terms of toilet functions, the assessment mainly considers the situation related to defecation and maturations, including if the patient can go to the toilet by himself/herself, if a diaper is needed, and the loss of control of defecation and maturations. The worst situation is that a Foley catheter is needed. In terms of medical treatment, the assessment mainly considers the need for medical treatment, including regular medical examination, emergency medical treatment, medical nutrition management, and special medical measures received in the previous two weeks. Each assessment option has a score. The RCTC system determines the grade in accordance with the scores to demonstrate the severity of each assessed criterion. Then, the type of care is determined according to the grade assigned to each element. The types of care fall into “total care,” “partial care,” and “no care.” The cumulative score of all subjects is calculated to judge the required care time. The higher the score is, the better the situation is and the shorter the care time needed.
3. Resident-Oriented Assessment
LTC institutions offer formal care services that provide living accommodations for residents who require on-site delivery of around-the-clock supervised care services, including professional health treatment and personal care services [27]. The concept of types of care or levels of care is used to classify residents on the basis of similar characteristics and to facilitate the delivery of appropriate care services [9]. Thus, a resident classification system should be resident-oriented, and a comprehensive assessment of resident characteristics related to health conditions and service requirements is assessed to reach a type of care decision. After classification by type of care, residents could be placed in an institutional facility that provides the needed care services.
The early LTC resident assessment tools mostly focus on the individual assessment at a single level. The major levels are assessment of cognitive function, assessment of activity function, and assessment of behavioural function [28]. Cognitive function refers to mental status, including memory, attention, and comprehension or language skills, which can identify dementia or signify the declining situation of patients with dementia in terms of cognitive function and dependence [29]. For example, the Mini-Mental State Examination (MMSE) is widely used to assess the cognitive function of the aged, while the Short Portable Mental State Questionnaire (SPMSQ) is used to assess mental status. Activity function assessment refers to testing and quantifying the ability to conduct functional movement. This assessment can be used to monitor the overall improvement situation of individual cases, including physical, mental, emotional and social functions. Therefore, it is an important reference to predict care needs and make care plans. The Barthel Index (BI) can be used to monitor the development situation in the rehabilitation field. Independence in Activities of Daily Living (ADL) is used to assess the movement independence of chronic disease patients and the aged in their daily lives. Instrumental Activities of Daily Living (IADL) is an important index to assess the independence of the aged. Functional Independence Measure (FIM) is used to assess the rehabilitation of multiple-disabled patients. Behavioural function assessment is mainly used to assess the behaviour problems of disabled patients, especially patients with brain damage.
In 1980, the WHO proposed the concept of International Classification of Impairment, Disability and Handicap (ICIDH), which influenced the concept of health functional assessment and its application. Many studies have explored the influence of health function classification on LTC [30]. Different health functional assessment tools were thus developed to assess LTC care needs. The most typical of these tools are the following. (1) The Residential Assessment Instrument (RAI) is composed of the Minimum Data Set (MDS), Resident Assessment Protocols (RAPs), and Specification. MDS contains all core items that must be assessed. RAPs are used to form nursing care plans [31], provide diagnostic logic, and help evaluators to confirm the care required by residents, in accordance with the care planning of individual cases [20]. (2) TAI is composed of classification and grading assessment scales, an assessment scale of the required care for the aged, degradation and aging process charts, and a summary table of each unit. TAI classifies the types of care and then grades them. The 12 types of care can be specifically divided into 6 scopes and 11 categories. The type of care, degradation and aging stage of care grades, and the care time needed in every stage are demonstrated by a diagram [32].
Results from previous study [26] suggested that assessment should be based on not only medical diagnosis but also impairment and disability for long-term care. Classification systems developed for LTC should use more sophisticated methods than those used in other care areas. One similar work [5] employed functional status, behavioural status, and medical diagnosis as variables for logistic function modelling to predict the prior probability of levels of care. A study [33] developed a classification system using functional level, disease category, risk factors, and health indices. Therefore, resident assessment must be multidimensional for LTC, and the assessment must be comprehensive enough to measure all elements for each resident. To evaluate the practical care needs of residents, “mental,” “movement,” “eating,” “toilet,” and “medical treatment” were the five main categories of variables used in this study. Moreover, the type of care classification for a resident was determined after a comprehensive assessment of the resident. The results of the resident's type of care can be helpful for the care of residents because the care service aspect is emphasised and curing disease is usually not a viable goal. Following classification by types of care, a resident can be placed in an institutional facility that manages the provision of substantial care services. Accordingly, residents can then be classified in terms of their required grade of care.
4. The Innovative Resident Care Process
Currently, most LTC institutions in Taiwan can only provide “package services” instead of individual services for residents. Before the completion of the RCTC system, the original care process of residents was as shown in Figure 2(a). The care appraisers manually and subjectively conducted the assessment by various scales as required, such as the Barthel Index, independence index of ADL, MMSE, SPMSQ, and Behavioral Rating Inventory of Executive Function. For normal situations, the care appraiser should fill in the corresponding care plan according to the health conditions of the resident. For example, if the resident encountered one care problem, a corresponding care plan should be filled in. If the resident encountered multiple care problems, multiple care plans should be filled in. However, because LTC residents often encounter multiple care problems at the same time, the final care plan will be rather complex and difficult to maintain without the aid of a software system. For this reason, the care staff will usually care for all of the residents with the same care plan. That is, aside from special medical situations, every resident will be treated under the same care plan, including eating, bathing, toilet, and movement. If there are no special circumstances, residents are not reassessed after admission.

Comparison of resident assessment processes.
Figure 2(b) shows the RCTC system innovative care process, which is composed of four stages: resident assessment, care plan, care implementation, and regular assessment. The care appraisers could comprehensively assess residents with the aid of the RCTC system, including mental, movement, eating, toilet, and medical treatment. After a comprehensive assessment, the RCTC system will automatically determine the type of care of each resident and predict the required care time. It is helpful for care administrators in the institution to place residents into different districts according to the type of care and organise suitable manpower according to the overall predicted care time. Aside from type of care and care time, the RCTC system can automatically form personalised care plans and weekly care schedules for each resident. Care staff in the institution can not only determine the health conditions of residents but also explain the current situation and care methods to residents’ relatives. If any amendment is needed or care emphasis is added by the resident's relatives, it can be recorded in the weekly care schedule. The overall weekly care schedule is based on different types of care, by which the care staff can implement their care work. An additional advantage of the RCTC system is that the staff can rapidly reassess whether there is any change in the resident's health condition. Moreover, the RCTC system will proactively notify the staff to conduct regular assessments every three months to make new care plans and weekly care schedules.
Additionally, the innovative resident assessment process assesses residents with the aid of the system instead of the written assessment method used in previous procedures. After the completion of the assessment, the care plan is formed automatically, which not only improves the situation of filling in many care plan forms but also increases communication methods with the relatives of residents. Moreover, the care staff can better understand the care content so that they can make fewer mistakes. The RCTC system can provide personalised care plans to improve upon the drawbacks of package services.
5. The Architecture of RCTC System
The methodological approach of RCTC system development is illustrated in Table 1 and has three stages: inception, object-oriented analysis and design, and implementation. Each stage is defined by work content, method, and output. The software development process includes eliciting information on systems and needs, mapping care processes into the system, and soliciting ideas for the software from institutional care staff. We developed a pilot run system for an institution and incorporated the resident assessment processes, assessment questions, care services, and required care time. We employed the ontology methodology to enable interdisciplinary team members to elicit requirements semantically and derive implementation models that meet those requirements, and the UML methodology was used to describe the static and dynamic structure of the RCTC system to generate conceptual models, dynamic models, and user interfaces. For knowledge-oriented systems, the ontology can formally represent knowledge as a set of concepts within a domain, as well as the relationships among those concepts. The ontology's vocabulary and taxonomy abilities provide a conceptual framework for sharing, analysing, and retrieving data in a specific domain. Therefore, ontology allows system developers to focus on the application domain structure rather than implementation details and allows the system developers to reuse and share application domain knowledge across different software platforms and programming languages. In this study, ontology helped care administrators, care staff, and system developers to utilise appropriate pieces of knowledge when facing complex care problems and situations.
The RCTC system development stages.

Figure 3 illustrates a schematic ontology class hierarchy structure for the RCTC ontology. The RCTC ontology presents a formalised description of concepts of resident classification by type of care. The information presented in this ontology was extracted from major resident charts, care plan templates, care guidelines, and administrative information, and it was discussed with the care administrators of the institution. The ontology class hierarchy structure was constructed on the basis of the resident assessment process, and it represents the five major subcategories, under the category of RCTC ontology. The five subcategories are resident management, care management, nutrition management, social worker management, and administrative management. There are three major categories under the resident management subontology: resident demographics, relative information, and admission notes. This subontology includes all basic concepts and health information that are relevant to residents in the institution. The care management includes major assessment tools, care plans, and weekly care schedules for the classification of residents by type of care. The nutrition management, social work management, and administrative management subontologies include information related to management of daily activities of the institution.
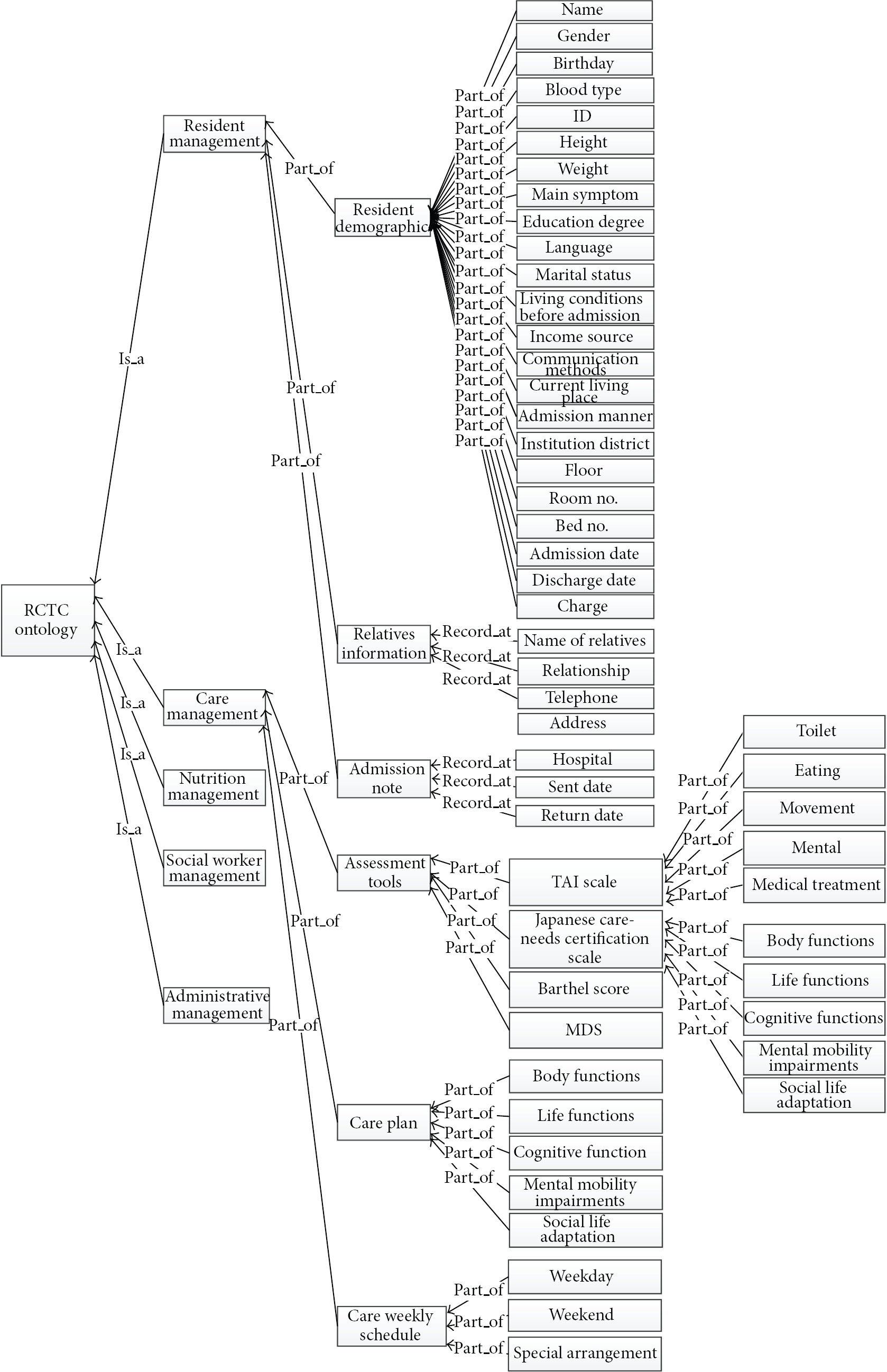
The RCTC ontology.
The proposed RCTC system is an assistance system for assessing institutional residents, as well as for generating personalised care plans and weekly care schedules. Our system is based on the World Wide Web (WWW) technique because the WWW is a standardised, cross-platform environment. WWW applications can be effective in creating virtual working platforms, which provide easy ways to collaborate and communicate with coworkers. Therefore, it is appropriate to use the WWW to develop an assistance system for resident management.
In this study, we used Microsoft SQL Server 2008 to build an institutional database based on the resident assessment tools and added tables at the care administrator's request. We used the C# programming language to code the whole system. The platform is available for the nursing staff, care staff, and institution administrator to obtain the required residents’ information. As shown in Figure 4, the RCTC system architecture includes an institutional database and two module sets. The module sets are described in detail below.

RCTC system architecture.
5.1. Assessment Module Set
This module set is primarily provided for user interfaces. It contains resident management, resident assessment, care plan generation, and weekly care schedule arrangement modules. The resident management module is used to manage residents in the institution. The resident assessment module determines the type of care of each resident and calculates care grade by classification and grading scales. The care plan generation module provides suggestions about care services and what care aspects should be emphasised. The weekly care schedule arrangement module helps care staff deliver better care service for the resident. Depending on the needs of the care staff, the interface for the assessment scales is customisable in that it displays adjustable items and uses a graphical interface to highlight the important changes after the assessment. It is therefore able to assist the care staff in understanding the changes in the health condition of the resident in the complex relationships among the five care aspects. Moreover, the resident's information, including their demographic personal details, discharged disease abstract, and assessment results, is maintained by the interfaces of this module set.
5.2. Management Module Set
This module set is mainly used by institution administrators to set up the system permissions, create and modify assessment tools, and estimate the overall resources needed for the institution. This module set is composed of system administration, scale tools management, care staff scheduling, and resource allocation modules. The system administration module offers the overall system functions for institution management. The scale tools management module is designed to maintain the assessment scales, including scale items, item weights, and algorithms for the estimation of care time. Because there are still many uncertainties in Taiwan's regulations and many factors involved in the assessment of residents, the use of assessment tools may be changed to comply with Taiwanese laws, so we retained flexibility in this module. Currently, the RCTC system mainly refers to the TAI scale, Japanese care needs certification scale, and Barthel score. The care staff scheduling and resource allocation modules can generate weekly care plans for individual residents and calculate the demand for manpower and resources, which can be valuable references for the institution administrator to manage and monitor resource consumption.
As shown in Figure 4, the resident assessment module is the most critical module of the RCTC system. The resident assessment procedure first evaluates care needs with respect to five functional status assessment attributes (with scores ranging from one to one hundred) of the resident. Then, it classifies residents into types of care categories (with grades ranging from one to seven). That is, three types of care and seven care grades are defined after evaluating by overall care time. The sequence diagram in Figure 5 explains how groups of objects work together to achieve the resident assessment process.

Sequence diagram for the resident assessment process.
This sequence diagram contains one main object on the appraiser's end. From this starting component, the care appraiser will receive the assessment demands from the RCTC server. The care appraiser can select the proper assessment tool to evaluate the health conditions of the resident, and it can also check the resident's record to see the resident's entire history. That history is retrieved from perspective tables in the institutional database. When any assessment is completed, the system will automatically compute the care needs and generate a personalised care plan and weekly care schedule for each resident. This procedure will enable care staff to deliver the required care services to their residents.
6. Design of the Assessment Algorithm for Care Time
RCS can assess the estimated case time of residents, which employs decision trees as its core. The design process is described in detail below.
6.1. Step 1: Conceptual Design of Decision Trees
The structure of the decision tree is similar to a binary tree, which has a root node; each node has a left and right child node. The decision tree's node not only stores numeric values, but also stores text. If the decision tree's node is a numeric value, then the value of the left node must be smaller than that of the right node. We designed the tree structure as database fields to record the relationship between nodes.
6.2. Step 2: Decision Tree Design
We employed a depth-first traversal algorithm to implement the recursive call of the decision tree. As shown in Figure 5, the back-end web server retrieves a decision tree structure from the database and generates HTML tag <ul> and <li> to include the tree's structure. When a user starts to use a decision tree, the system will first create the current root node and its left and right child nodes according the node value. Then the decision subtree structure was included in the <ul> and <li>XML tag. The tree generation process will end when the decision tree build is complete. Finally, a j Query organization chart plugin was used to generate a visualized decision tree.
6.3. Step 3: Connecting to the Assessment Results
After the completion of the decision tree, we need to connect the assessment results with the decision tree. We first added four fields including node type, type code, left side rules, and right side rails into a decision tree table (Table 2). The tree traversal direction depended on the current subtree's assessment result. As shown in Figures 6 and 7, the node's type and type code were used to identify the scale subject and assessment dimensions and then traversed the left side rule or right side rule by the rule of the node. The assessment result is determined once the expected traversal was made.
Decision tree table.


Decision tree building process.
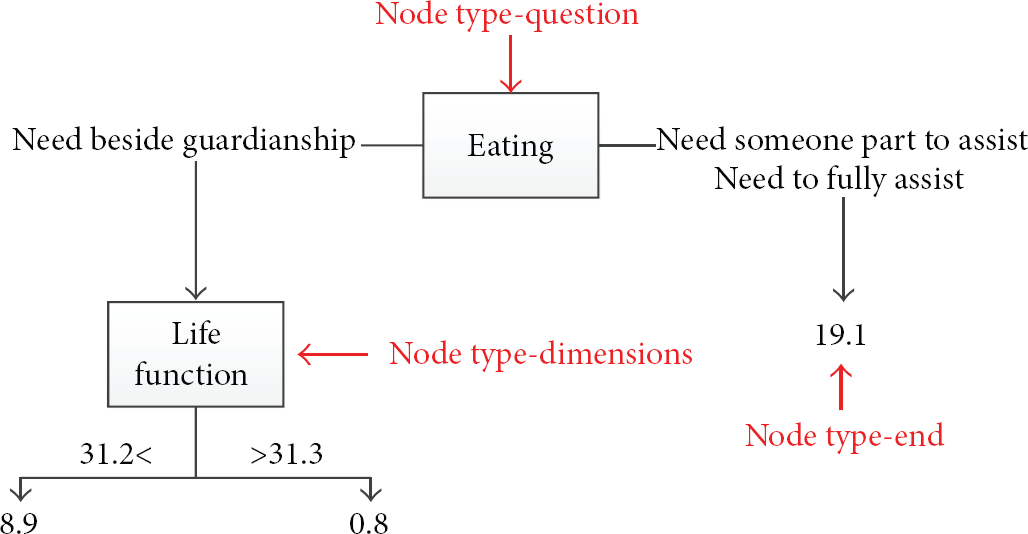
Node type determination.
6.4. Step 4: Decision Tree Judgment Logic
Using decision tree judgments logic to determine the case time of results output. The judging process will call their own, when the node type is “results” output care time. If cannot be found node who behalf node type or node location, output “Error”. As shown in Algorithm 1, Cannot be found node occurs, set of judgments of the decision tree set error, need to be corrected.
{ Switch nodetype readEvaluate RecursiveTree (node, left) RecursiveTree (node, right) response break; readEvaluate RecursiveTree (node, left) RecursiveTree (node, right) response break; response root : name (code) = score break; response break; }
{ response }
7. System Implementation
In this study, the RCTC system provides an institutional database that stores relevant data such as the resident's demographic data, disease history, assessment results, specific care needs, and type of care and the care appraiser's interactions with the caregivers. These stored data help the care staff to assess the care needs based on their residents’ health conditions, care plan arrangement, and wellness activities, as well as the status of care decisions, care actions undertaken, and other relevant information that could aid in the provision of proper care. The RCTC system provides information on residents’ care type, care method, estimated care time, and personalised care plan, as well as the weekly care schedule for residents in each district. The care appraisers can add or modify the residents’ basic data, hospitalisation records, and other information. To retain the flexible extension of the system, the RCTC system follows the modular design principle, enabling the institution care appraisers to modify and maintain assessment tools and care plan templates, thereby enhancing its usability.
We show several screen layouts, including the system administrative environment, scale tools layout, assessment screen, personalised care plan, and estimation of institutional overall resource needs. Figure 8 depicts the function of assessing resident's care needs. Care appraisers assess the resident by asking questions relating to the five functional status assessment aspects, and they choose the proper care plan corresponding to the selected option. The personalised care plan offers suggestions on each aspect of the assessment results. The assessment module automatically computes the grades of the care needs for each aspect. Care staff can follow the content of the care plan to implement their care work. Figure 9 shows the assessment result determined by the system, which shows the required care time for nine care-need components, grades resident care needs as “level seven,” and recommends the type of care as “heavy degree of care needs.” The care appraiser and care staff can quickly review the overall situation and care needs of the resident by using the information shown as a report and a radar chart. According to the care plan, the weekly care schedule presents the care methods and care notes of the resident in different timetables. Care staff of the institution should record the additional requirements provided by family members of the residents in the sheet during their communication.

Assessment of a resident's care needs.

Resident assessment result.
The desire to balance the individual resident's care needs with the constraint of manpower limitations led us to develop our resident classification mechanism. The assessment/classification sequence is intended to be used by care appraisers, who are involved in resident assessment and care service delivery. For institution management issues, management data were collected on the selected residents not only through assessment/classification by the care appraisers, who may or may not be independent of the institution, but also by service caregivers within institutions. Because the primary resource used by LTC institutions is manpower, classification/placement is intended to determine how much care manpower should be put into each resident based on overall estimated care time. The assessment/classification provides information on residents who are under specific types of care with different care-level grades, and the classification/placement information can be used for reimbursement, bed assignments, and decisions about staff assignment, recruitment, and staffing ratios, to achieve effective management and operational efficiency.
8. Conclusions
The RCTC system presented in this study provides care practitioners in LTC institutions with a comprehensive assessment system that includes classification and grading concepts. The RCTC conceptual model follows an assessment/classification/placement sequence that can be used for resident assessment, classification, and placement decisions for LTC residents. The major functions of the RCTC system are to assess LTC residents based on five functional status assessment aspects, classify residents into different types of care, and grade the care needs in terms of severity. Moreover, this RCTC system offers personalised care plans and weekly care schedules, which make the care methods more flexible and of higher quality than traditional “package services.” During our research, we proposed that the estimation of a resident's overall care time can be employed to estimate the resources the institution will require, including care manpower and consumptive materials. Currently, the system is under a pilot run with our cooperative institution. We hope to offer an assessment framework sample of an LTC institution in Taiwan that can be widely used in the future. We also plan to cooperate with the hospital to implement the system outside of LTC institutions and use it to realise seamless service in hospitals.
Footnotes
Conflict of Interests
The authors declare that there is no conflict of interests regarding the publication of this paper.
Acknowledgments
This research was partially supported by National Science Council of Taiwan, under Research Projects NSC102-2221-E-227-001 and NSC100-2622-H-227-001-CC3 and by the MSIP (Ministry of Science, ICT and Future Planning), Korea, under the ITRC (Information Technology Research Center) Support Program NIPA-2013-H0301-13-4007 supervised by the NIPA (National IT Industry Promotion Agency).