
Abstract
We have successfully employed two-step circumspinal decompression for the treatment of thoracic OPLL. In the first step, laminectomy is performed according to the ossified lesion, and then correcting fixation of kyphosis (dekyphosis) is performed using instrumentation. In this study, we reconstructed the first step by a FEM. A commercially available FEM of the human body, THUMS, was used for the modeling of the operative procedure. The spinal cord and OPLL were incorporated into this model. After applying imposed displacement to OPLL, mechanical stress on the spinal cord was measured before or after posterior decompression at the occupying rates in the spinal canal between 0 and 70% in this model. When the occupancy rate was greater than 60%, the stress decreased after decompression compared to before decompression. The stress decreased by up to 52.3%. For reconstruction of dekyphosis, the change in the stress was analyzed after imposed displacement by which the spine was decreased: the cobb angle decreased by 10 degrees between T7 to T11. As a result, the stress further decreased by 14.6%. The present study proved the usefulness of posterior decompression and dekyphosis in order to reduce the pressure of the spinal cord in circumspinal decompression.
1. Introduction
Ossification of the posterior longitudinal ligament (OPLL) is an intractable disease characterized by spinal canal narrowing and spinal cord compression due to ossification/enlargement of the posterior longitudinal ligament extending craniocaudally along the posterior surfaces of the vertebral bodies, resulting in spinal paralysis.
We performed a 2-step surgery (posterior decompression and fusion as the first step and anterior decompression as the second step) for OPLL in the thoracic spine to achieve circumspinal decompression and obtained favorable results [1]. At the time of posterior decompression and fusion, correcting fixation of kyphosis (dekyphosis) in addition to laminectomy had been performed [2, 3]. Dekyphosis may lead to indirect spinal cord decompression, producing favorable results.
Therefore, we produced finite element models (FEMs) of OPLL in the thoracic spine, including the thoracic spinal cord, and mechanically evaluated the effects of posterior decompression and fusion, with dekyphosis as our routine method on the spinal cord, using computer simulation.
2. Methods
2.1. Posterior Decompression and Fusion with Dekyphosis
In posterior decompression and fusion as the routine method, laminectomy in the ligament ossification area is performed, followed by posterior decompression. Subsequently, left and right pedicle screws are inserted into the cranial and caudal sides of the ossification area, and rods with curvature about 15 degrees smaller than the kyphosis angle are placed into the screw heads for 5 to 10 degrees reduction in kyphosis and stabilization (Figure 1).

2.2. Production and Analysis of FEMs
To utilize the total human model for safety (THUMS: Toyota technical development) as a FEM of the human body in this study, the following revisions were made. The THUMS is an FEM model of the whole human body for crash analysis (Figure 2 (a)). The model used in this study was for an assumed female in the standing position (height, 150 cm; weight, 50 kg; and age, 40–50 years). From this THUMS, the head, spine, and ribs were extracted, and modifications were made to obtain a continuous model in this study (Figure 2 (b)). The spinal cord, spinal nerve roots, and OPLL were added to the original model for this study (Figure 2 (c)).

Since Tsuzuki [4] reported that the spinal canal area is smaller at the 8th thoracic spine (T8) and T9 than at other levels, OPLL between T8 and T9 may induce severe myelopathy. Therefore, the model was constructed assuming OPLL between T8 and T9. The shape of OPLL was assumed to be the simple segmental type. The ligamentum flavum was assumed to have a simple shape with a maximum thickness of 2 mm. The material constants of the ligament were inputted.
The spinal cord was added so that it could pass through the midline of the spinal canal. We performed modeling, assuming that the spinal cord extends to L5. Since ossification at T8-T9 was assumed in this study, the thickness of the spinal cord at T8-T9 was used. The thickness of the spinal cord at this level was determined based on the measurement results on MRI images of 20 healthy adults. As a result of the determination of the percentage of the anteroposterior diameter of the spinal cord to that of the spinal canal at T8-T9, the mean value was 50% (45%–60%). Therefore, the size of the spinal cord was determined to be 6.5 mm (50% of the anteroposterior diameter of the spinal canal at T8-T9). The transverse diameter was determined to be 10 mm as the general size [5]. There are no generally accepted opinions about Young's moduli of the gray and white matters of the spinal cord [6, 7]. Therefore, in this study, to simplify the model, we used the results of tensile tests performed by Bilston and Thibault [8] using the human cervical spinal cord without distinction between the gray and white matters. Spinal nerve roots from the 1st cervical spinal nerve to the 5th lumbar spinal nerve were constructed. Each nerve root was established so that it would originate in the spinal cord at the middle level of each vertebral body and be fixed on the posterolateral side of the vertebral body corresponding to the intervertebral foramen. The material constants of the nerve root were determined based on the report by Scifert et al. [9].
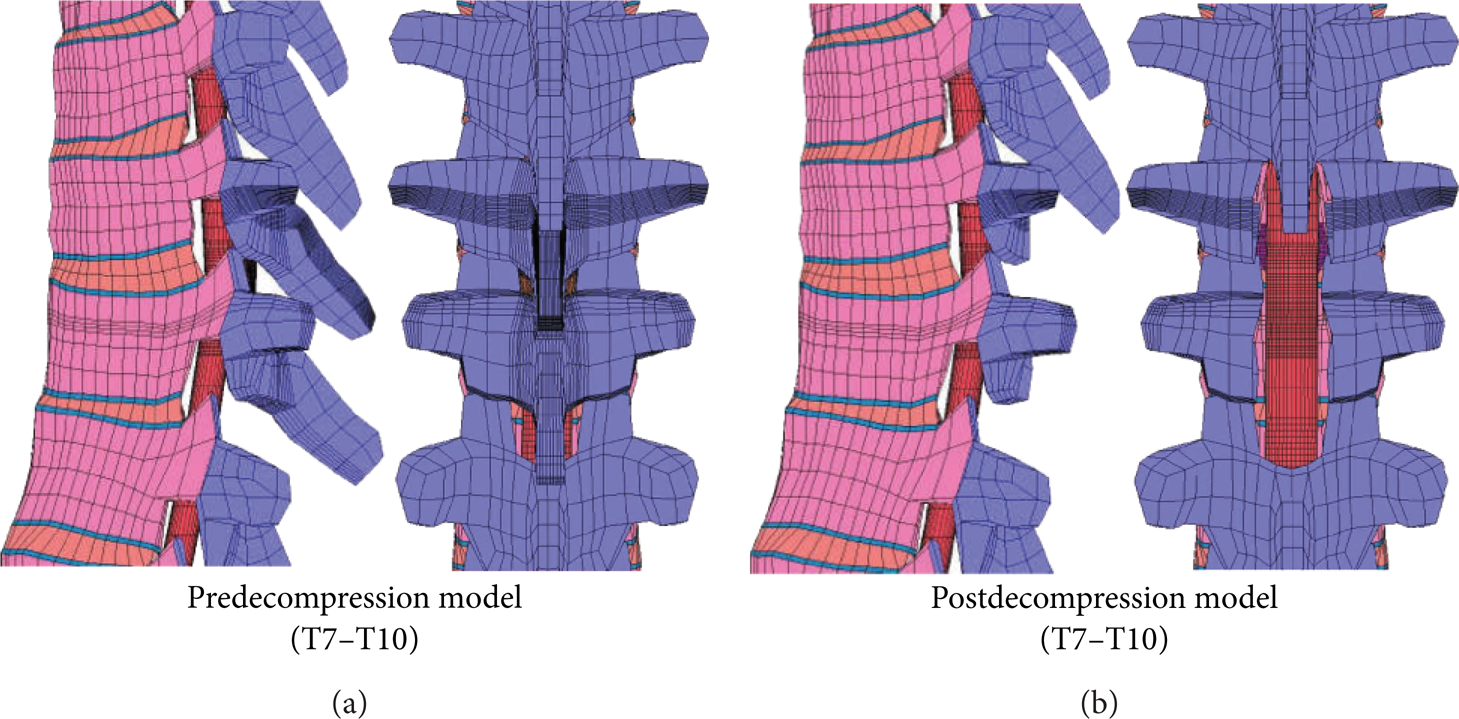
In this study, to evaluate the mechanical effects of spinal cord decompression, two models (before and after posterior decompression) were produced. The model after posterior decompression was produced by removing the vertebral arches (the posterior part of a vertebra) of T8 and T9 from the preoperative model (Figure 3).
The material constants of this analytic model were the same as those used in the THUMS. The material constants of OPLL, which were newly added, were assumed to be similar to those of cortical bone in the thoracic spine (Table 1). Further, 248.7 (N) corresponding to the weight of the upper half body was applied to the center of gravity of the trunk, and analysis was performed [10]. As having restraining conditions, the intervertebral disc and spinal cord on the lower surface of L5 were completely fixed.
Material constants of the model.
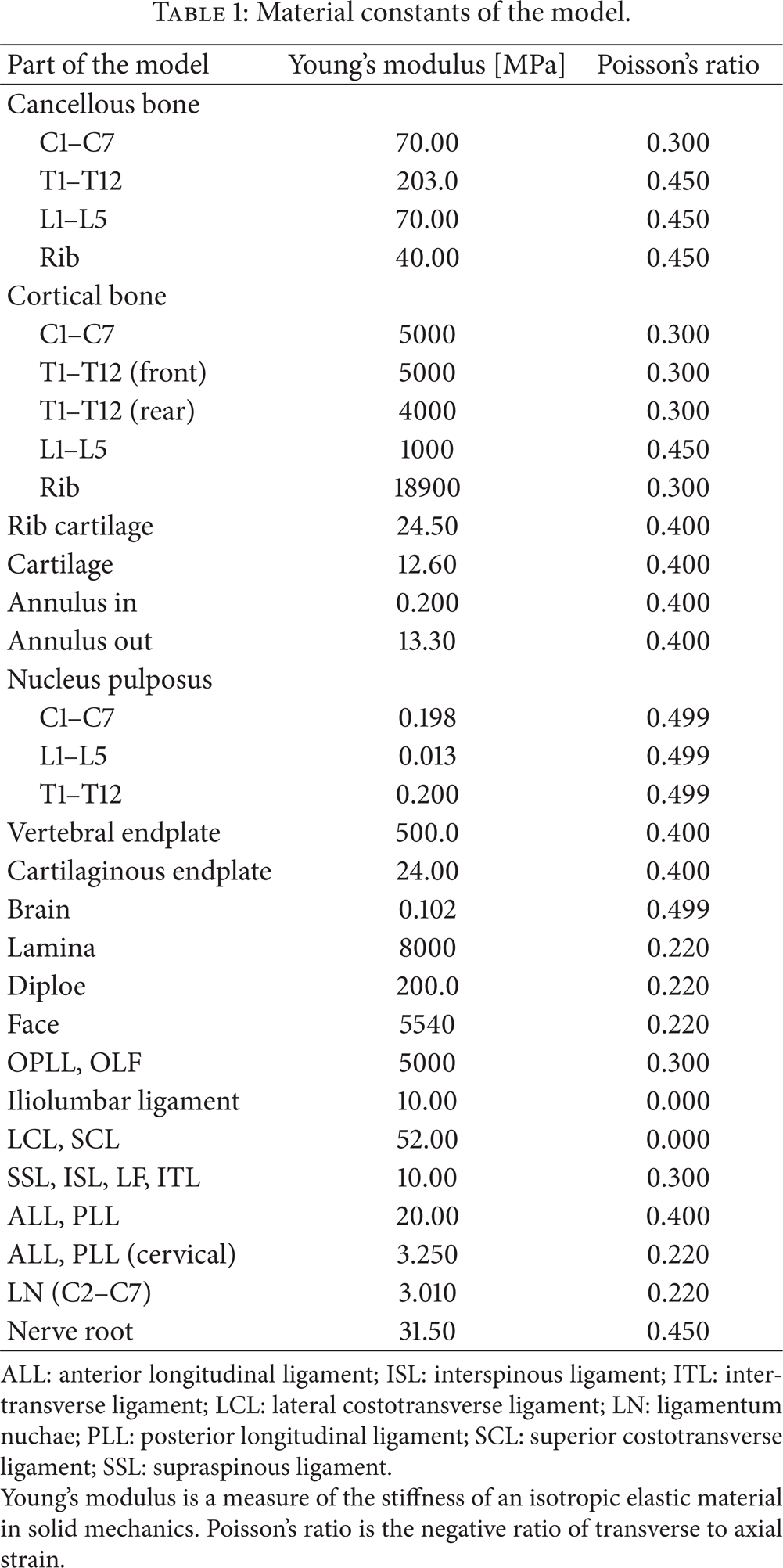
ALL: anterior longitudinal ligament; ISL: interspinous ligament; ITL: intertransverse ligament; LCL: lateral costotransverse ligament; LN: ligamentum nuchae; PLL: posterior longitudinal ligament; SCL: superior costotransverse ligament; SSL: supraspinous ligament.
Young's modulus is a measure of the stiffness of an isotropic elastic material in solid mechanics. Poisson's ratio is the negative ratio of transverse to axial strain.
There have been various studies on the relationship between the occupation rate and symptoms [11–13]. Matsunaga et al. [14] reported that myelopathy developed in all 45 patients with an occupation rate ≥60%. Therefore, in this study, to create an occupation rate ≥60%, analysis was performed by changing the size of OPLL so that the occupation rate became 70%, respectively. Changes in OPLL were reproduced by applying forced displacement to the surface (Figure 4).

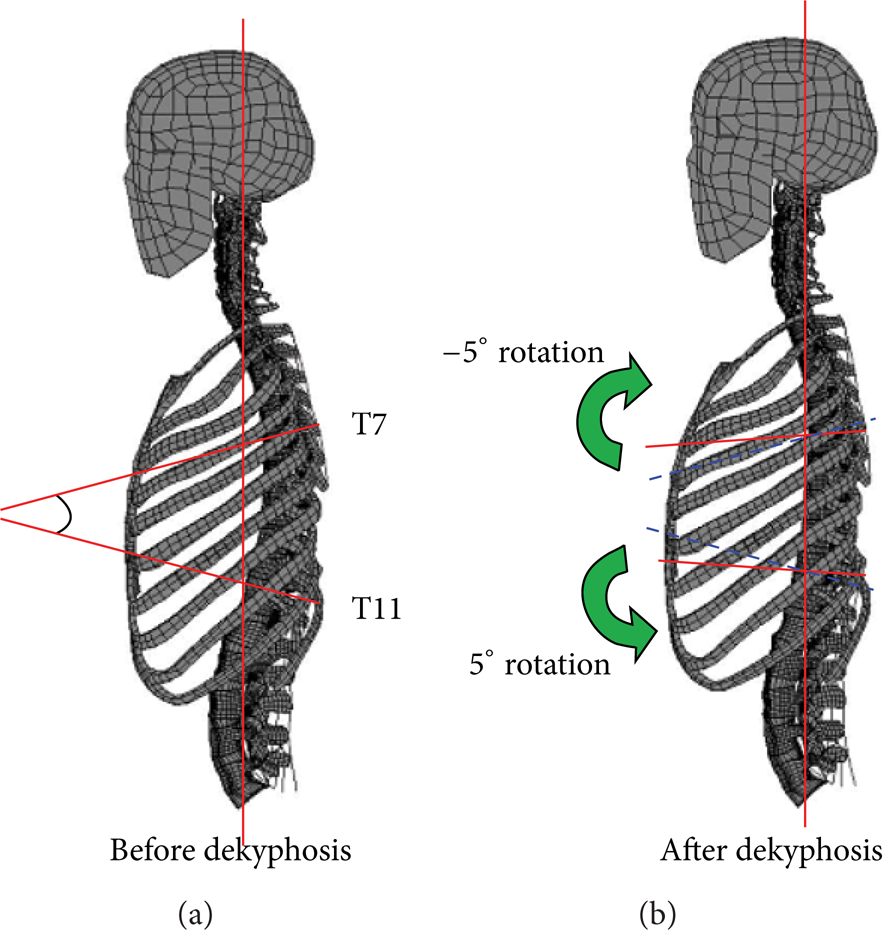
Under these conditions, analysis and comparison were performed using the model before posterior decompression and model after laminectomy representing posterior decompression. In addition, mechanical evaluation after posterior decompression followed by thoracic dekyphosis was performed. Since the mean dekyphosis angle in the 15 patients that we surgically treated was 6 degrees (5–10 degrees), the maximum dekyphosis angle in this study was determined to be 10 degrees, and stress was measured with each dekyphosis angle from 0 to 10 degrees. As shown in the postdecompression model with a Cobb angle (the angle formed between a line drawn parallel to the superior endplate of the upper vertebra and a line drawn parallel to the inferior endplate of the lower vertebra) between T7 and T11 of 19 degrees in Figure 5, dekyphosis was reproduced by rotating the upper part of T7 by −5 degrees and the lower part of T11 by 5 degrees (total rotation, 10 degrees).
3. Results
3.1. Analysis of the Model before Posterior Decompression
When the occupation rate of OPLL was gradually increased from 0%, stress in the spinal cord began to develop at about 25%, and it increased with the occupation rate. In particular, when the occupation rate exceeded 60%, the spinal cord was markedly deformed, and stress sharply increased (Figures 6 and 7). The maximum stress at an occupation rate of 70% was 618 kPa.

3.2. Analysis of the Model after Posterior Decompression
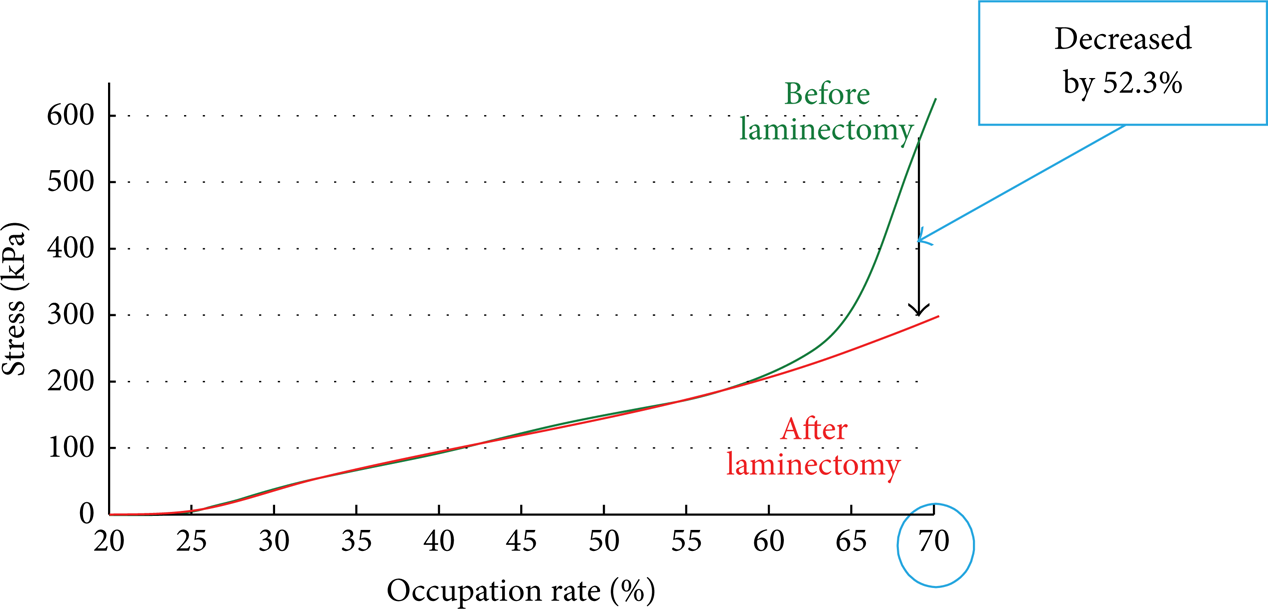
In the postdecompression model as well as the predecompression model, stress increased with the occupation rate. The stress in this model was similar to that in the predecompression model until an occupation rate of 50%, but it was lower than that in the predecompression model at an occupation rate ≥50% (Figures 6 (c) and 7). The maximum stress at an occupation rate of 70% was 295 kPa, showing a 52.3% reduction compared with the value (618 kPa) in the predecompression model.
3.3. Analysis of Dekyphosis
In the model after posterior decompression, dekyphosis reduced stress in the spinal cord. The degree of this reduction increased with an increase in the dekyphosis angle. At an occupation rate of 70%, the stress before dekyphosis (dekyphosis angle was 0 degree) was 295 kPa, but it maximally decreased to 252 kPa (a 14.6% reduction) when the dekyphosis angle was 10 degrees (Figure 8).

4. Discussion
We have reported that posterior decompression followed by kyphosis correction is effective against myelopathy due to thoracic OPLL based on clinical results. However, there have been no mechanical studies on this surgery. In this study, FEMs of thoracic OPLL were produced, and stress generated in the spinal cord was analyzed.
In the predecompression model, stress generated in the spinal cord began to increase when the OPLL occupation rate increased to 25%. This may have been because of contact between OPLL and the spinal cord at an occupation rate of 25%. The maximum stress began to sharply increase at an occupation rate of 60%. The spinal cord comes into contact with the ligamentum flavum at an occupation rate of 50%, but since the ligamentum flavum is soft, this ligament may not have affected the maximum stress at an occupation rate from 50% to 60%. These results suggest that the risk of spinal cord disorder increases at an OPLL occupation rate >60%.
At an OPLL occupation rate ≥60%, stress generated in the spinal cord was lower in the postdecompression model than in the predecompression model. At an occupation rate of 70%, the maximum stress generated in the spinal cord was 618 kPa before posterior decompression and 295 kPa after posterior decompression, showing a 52.3% decrease. This may have been because of the absence of anteroposterior trapping of the spinal cord due to laminectomy. Posterior decompression markedly decreased stress in the spinal cord.
On the other hand, the results of the present experiment suggest that stress remains in the spinal cord even after posterior decompression, and the effects of posterior decompression performed alone are inadequate in the presence of extensive OPLL. Tokuhashi et al. [15] described that spinal decompression is inadequate in using posterior decompression and fusion alone when the thoracic kyphosis angle is > 23 degrees. Ito et al. [16] defined the local ossification angle (the medial angle at the intersection between a line from the superior posterior margin at the cranial vertebral body of maximum OPLL to the top of OPLL with beak type and a line from the lower posterior margin at the caudal vertebral body of the maximum OPLL to the top of OPLL with beak type) and reported poor improvement in the JOA score after posterior decompression alone when this angle was >28 degrees. Thus, since there is a possibility that the results of posterior decompression are affected by not only the size of the anterior ossification lesion but also the local kyphosis angle, changes in stress in the spinal cord after reducing kyphosis were evaluated in the dekyphosis model in this study. As a result, the maximum stress decreased by 14.6% after a 10-degree reduction in kyphosis compared with the predekyphosis value in the model at an OPLL occupation rate of 70%. This shows a decrease in spinal cord compression by OPLL after dekyphosis, which may have been because the spinal cord shifted posteriorly after dekyphosis and was indirectly decompressed. Based on these results, further improvement in symptoms by indirect decompression using dekyphosis can be also expected in clinical practice. Matsuyama et al. [17] clearly showed, using intraoperative ultrasonography, a reduction in pressure from OPLL after dekyphosis using posterior instrumentation. Posterior stabilization with instrumentation prevents postoperative kyphosis and the instability after posterior decompression for thoracic OPLL [15, 17–19]. Dekyphosis stabilization is not only to maintain spinal stability but also to reduce the compressive pressure of the OPLL plaque on the spinal cord [3].
In actual surgery, posterior decompression with dekyphosis is performed as a first-step operation, and resection of OPLL using an anterior approach is performed as a second-step operation. Our results showed that stress in the spinal cord is markedly reduced by posterior decompression and further reduced by the following dekyphosis as a first-step operation. This spinal cord decompression allows safer OPLL resection using an anterior approach as a second-step operation.
In this study, the spinal cord was modeled as a simple shape with a constant thickness. For more detailed analysis of the spinal cord closer to that in the human body, analysis using models that also have the dura meter, cerebrospinal fluid, and internal structures of the spinal cord is necessary. In addition, since the morphology of the spinal cord as well as OPLL differs among individuals, analysis using a model of each patient is also clinically required. Thus, analysis using models closer to the human body is necessary in the future.
5. Conclusion
We reconstructed the OPLL model using a finite element model, and the mechanical stress on the spinal cord was measured.
After the laminectomy when the occupancy rate was 70%, the stress put on the spinal cord is decreased by 52.3%
We found that laminectomy was more effective when the OPLL occupancy rate was greater.
When the dekyphosis angle was 10 degrees, the stress on the spinal cord decreased by 14.6%.
This study demonstrates that the pressure on the spinal cord is indirectly reduced by dekyphosis.