
Abstract
Urinary incontinence is a common problem among adults. Studies have shown up to 70% improvement in stress incontinence symptoms following appropriately performed pelvic floor exercise. This improvement is evident across all age groups. In this study, we cooperated with a doctor of the Department of Obstetrics and Gynecology, Taipei Veterans General Hospital, Taiwan. We developed a noninvasive device with the purpose of helping patients commence and perform pelvic floor muscle training (PFMT). This device consists of a PFMT device, an Arduino control board, a force sensor, a Bluetooth device, and an SD card. The objectives of this study are to train patients to inhibit detrusor contraction voluntarily and to contract periurethral muscles selectively. The system records and analyzes sensor data and provides voice prompts during PFMT exercise for patients at hospitals or their homes. Meanwhile, it tracks patients' PFMT exercise at home, and doctors can contact patients for additional visitation(s) if necessary.
1. Introduction
Urinary incontinence in women is a common, distressing, and costly health problem. Urinary incontinence often causes a loss of self-esteem, social isolation, and restriction of normal activity [1–4].
Pelvic floor muscle exercises, initiated by Kegel in 1948, strengthen the tone and contraction of periurethral and pelvic floor muscles. Pelvic floor muscle training (PFMT) or Kegel exercise has been found effective in reducing stress incontinence and also urge incontinence [5–8]. Studies have shown up to 70% improvement in stress incontinence symptoms following appropriately performed pelvic floor exercise. This improvement is evident across all age groups [9, 10].
However, several issues require addressing: (a) there is no doctor or continence nurse supervision and patients cannot determine whether PFMT is done correctly, at home, and (b) to obtain results from rehabilitation, doctors must wait at least one month for a patient to revisit. If problems exist in the patient's rehabilitation process, they will delay the diagnosis and treatment schedule [11, 12].
The aim of this study is to rehabilitate the pelvic musculature. We cooperated with Dr. Horng, a doctor of the Department of Obstetrics and Gynecology, Taipei Veterans General Hospital, Taiwan. We developed a non-invasive device with the purpose of helping patients perform PFMT. This device consists of a PFMT device, an Arduino control board, a force sensor, a Bluetooth device, and an SD card.
The objectives of this study are to (a) train patients to inhibit detrusor contraction voluntarily and contract periurethral muscles selectively, (b) record/analyze sensor data and also provide voice prompts during PFMT exercise for patients at hospitals and home, and (c) track patients at home during the PFMT process, so that doctors can monitor patients and initiate additional visitations, if necessary.
With this system, doctors can keep track of patients' courses of treatment, and patients can receive better medical care.
2. Materials and Methods
In this study, our system architecture is divided into four layers, the physical layer, sensing layer, network layer, and application ayer. The physical layer includes medical equipment and an embedded system. We integrated an embedded system into medical equipment to install sensors. The sensing layer consists of sensors used to sense the rehabilitation process of patients. The network layer uses wireless transmission technology to transfer data. Finally, the application layer, including the application programs that provide feedback to patients during the rehabilitation process, analyzes and tracks patients' rehabilitation for doctors. The architecture is shown in Figure 1.

The architecture of the non-invasive wireless sensor PFMT device.
2.1. Physical Layer
We use a PFMT device, consisting of a U-shaped spring, which makes it easier for patients to use the non-invasive device for PFMT rehabilitation. The non-invasive wireless sensor PFMT device consists of a force sensor connected to an Arduino control board. The force sensor was placed inside the PFMT device and is used to obtain measurements of the contraction force of pelvic floor musculature, as illustrated in Figure 2.

The noninvasive wireless sensor PFMT device.
2.2. Sensing Layer
We use force sensors to detect the patient's pelvic floor muscle contraction, which determine whether the PFMT rehabilitation of the patient is correct or not. Using the PFMT device shown in Figure 3, the process of pelvic floor muscle training by way of clamped PFMT device (used between the thighs) and variations in contraction force of pelvic floor musculature can be accurately measured.

The pelvic floor muscle training with PFMT device.
2.3. Network Layer
The PFMT device includes a Bluetooth device that is used to transmit sensor data to a mobile device, such as a smartphone or a tablet, for analysis and feedback; an appropriate message will prompt patients on what steps should be taken after device usage. The rehabilitation data of a patient can be sent through mobile device directly to hospital servers. In this way, the doctor can keep track of patient rehabilitation and provide the appropriate treatment(s). If the Bluetooth device cannot successfully link to a smartphone, tablet, or desktop computer, an SD card is can be used in the PFMT device to store sensor data. When patients return to the hospital, doctors can obtain sensor data from the SD card and analyze the PFMT exercises done by patients.
2.4. Application Layer
The application layer is divided into two subsystems. One is the client system, and the other is the server system. The client system is a home rehabilitation system, whereas the server system, which is an intelligent medical treatment system, is built at the hospital. The detailed descriptions are as follows.
Home rehabilitation system. The home rehabilitation system analyzes sensor data from the network layer and transmits responses to the patient via text message, audio message, video message, vibrate, and/or other multimedia. In this way, the patient can determine whether his/her actions are correct or not. Intelligent medical treatment system. Doctors can track and observe patients' PFMT exercises done at home by way of the intelligent medical treatment system. This system receives sensor data of rehabilitation exercise processes from the home rehabilitation system. Using the sensor data, this system analyzes patients' rehabilitation processes includes physical conditions and rehabilitation results. The features include (a) tracking whether patients perform daily PFMT exercise assigned by doctors, (b) analyzing whether or not the PFMT exercise process is correct, and (c) the adjusting of the rehabilitation plan depending on patient rehabilitation.
3. Data Processing and Analysis
First, patients performed PFMT rehabilitation exercise regimes supervised by doctors, specialist physiotherapists, and/or continence nurses at a hospital. We collected the sensor data and proposed a quantization method. The aforementioned method converts sensor signals into quantifiable data. Furthermore, we used statistical k-means clustering [13–16] and the k-nearest neighbor algorithm (k-NN) [17, 18] to analyze data. This provides important information for helping patients execute PFMT exercise and also assists doctors in medical care.
3.1. Data Collection
In accordance to doctor instructions, patients commence performing PFMT exercise. If necessary, doctors may use electrical stimulation to help patients understand how to correctly complete pelvic floor muscle contractions.
Two experimental examples of PFMT exercises are shown in Figures 4(a) and 4(b); the force of pelvic floor muscles is measured with respect to the force unit in pounds, as shown on y-axis. Figure 4(a) shows the signals of a patient's PFMT exercise, but the exercise results are incorrect. The force is strong. However, it is from thighs, not from pelvic floor muscle. Figure 4(b) shows the result after the patient correctly performs PFMT exercise.
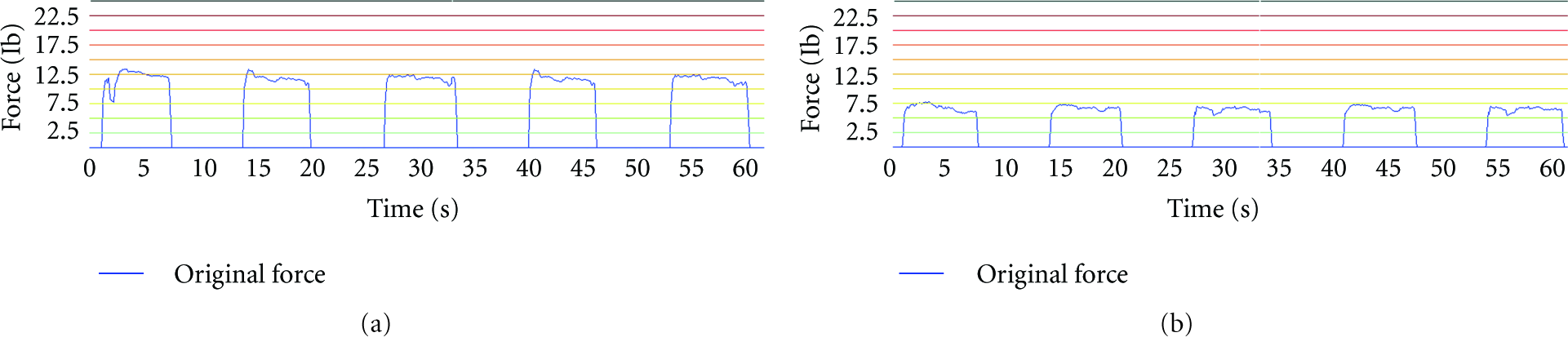
(a) Signals of an incorrect PFMT exercise, (b) Signals of a correct PFMT exercise.
3.2. Quantization
To analyze data of patient rehabilitation, we proposed quantization methods to convert sensor data into quantifiable data. To judge the correctness of a patient's exercise, we needed to know the force and duration of pelvic floor muscle contraction. The standard deviation is used to evaluate the stability of the patient's movements as shown in Figures 5 and 6.
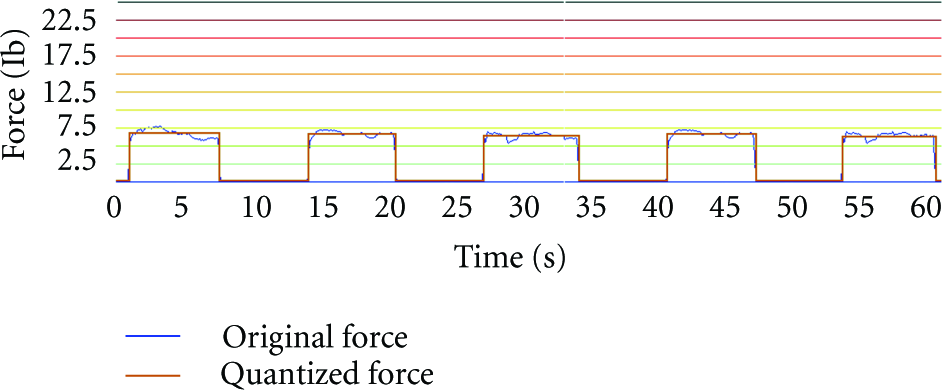
Original force and quantized force of five pelvic floor muscle contraction motions.

Quantized force and the standard deviations of force in a PFMT exercise.
We denoted
Duration of a pelvic floor muscle contraction:

Force of a pelvic floor muscle contraction:

We then convert data into a Cartesian coordinate system. Figure 7 shows the relationship of duration and force of pelvic floor muscle contraction motions in a PFMT exercise. A point with coordinate (X, Y) denotes the duration and force (

The relationship of duration and quantized force of pelvic floor muscle contraction motions in a PFMT exercise.
In order to allow doctors evaluate the quality of patient PFMT exercises, we provide a standard deviation force of each pelvic floor muscle contraction. In this way, doctors can review the detailed status of each contraction in a PFMT exercise and, if necessary, provide additional medical assistance to help patients improve their contraction motion. The formula is shown below.
Standard deviation force of a pelvic floor muscle contraction:
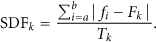
Figure 8 illustrates the standard deviation of pelvic floor muscle contraction motions in a PFMT exercise. The duration and standard deviation (

The standard deviation of pelvic floor muscle contraction motions in a PFMT exercise.
3.3. Analysis
Because hospital patients can obtain assistance from doctors and nurses to do PFMT exercises correctly, much helpful pelvic floor muscle contraction sensor data can be collected by the PFMT device. Differences in patients' ages, genders, body types, and recovery situations are reflected in the quantized contraction sensor data, reinforcing the necessity to analyze data according to the individual.
After quantization, we can determine what constitutes correct contraction sensor data, such as the high-density cluster in the lower-right corner of Figure 7. In statistics and data mining, k-means clustering is a method used for cluster analysis. Thus, k-means clustering is used in this study to classify sensor data as correct or incorrect in performance of a contraction. The operations are formulated in (4) through (5) and are listed as follows [19, 20].
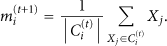
Given an initial set of k-means (

3.4. Classification
According to the results of k-means classification, we use k-NN analysis for the sensor data of pelvic floor muscle contractions when patients perform PFMT exercises at home. K-NN can classify that a particular motion belongs to particular cluster, according to the characteristics of the cluster and doctor guidelines; we use text, audio, video, voice, and/or vibration feedback to assist patients in understanding the correctness of their PFMT exercise.
We can represent our data set containing P clusters
k-NN [21, 22] can be run in these steps.
Store the output value of the k-nearest neighbors to a query contraction motion q in vector
The query contraction motion q is classified by cluster m, where
4. Experimental Results
Rehabilitation procedures are divided into four phases. In the first phase, the patient, with the assistance of a doctor, learns how to use the PFMT device, which is a specialized aid used for urinary incontinence rehabilitation. The PFMT device is combined with an embedded system device to detect rehabilitation movement. This assistive device is placed between thighs to measure the force of pelvic floor muscle contractions. In this phase, the sensor data of the patient for pelvic floor muscle contraction is collected at the hospital, as shown in Figure 9.

Collecting the sensor data of pelvic floor muscle contraction.
In the second phase, the k-means algorithm is used to classify collected sensor data collected during the first phase. The data classifications will be used as training data, so that the doctor can examine a patient's condition and prescribe personalized treatment. Doctors, according to classification results, establish guidelines using the characteristics of each cluster corresponding to the patient's condition.
Figure 9 shows the classification results of a PFMT exercise by k-means clustering, in which
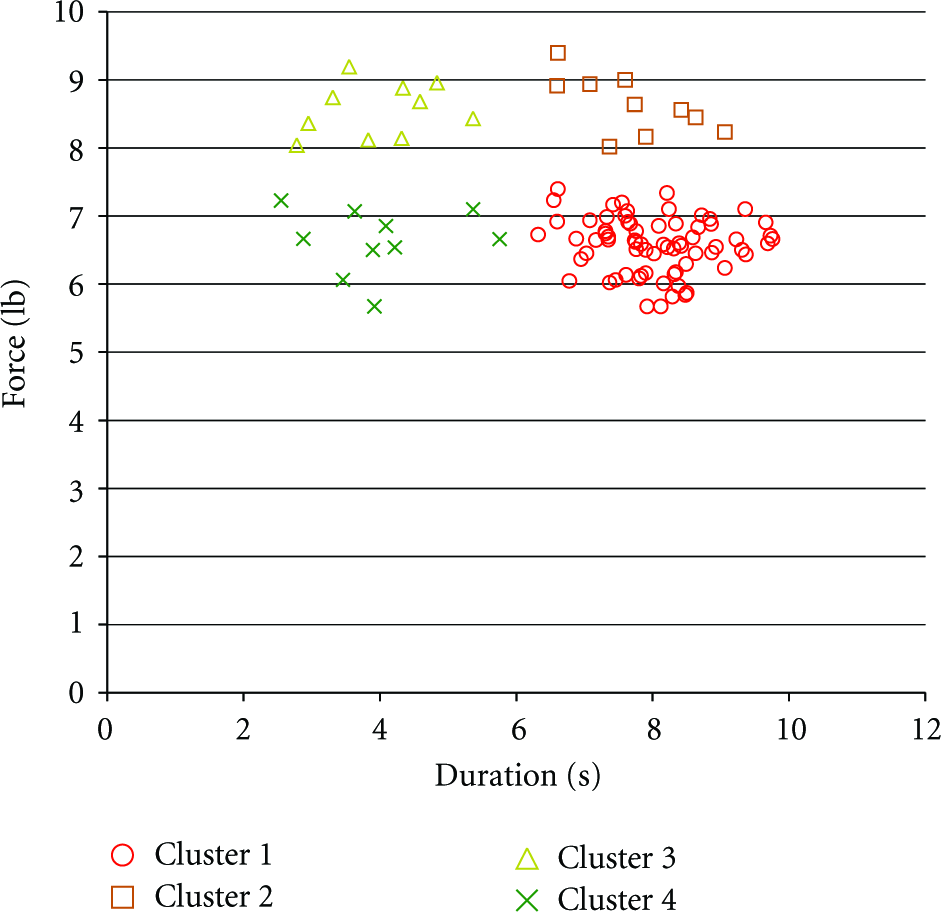
Classification results of a PFMT exercise by k-means clustering,
In the third phase, sensor data of patient rehabilitation at home is collected. The proposed system uses k-NN algorithm to classify the sensor data and determine whether the patient's contraction actions are correct, according to medical treatment and guidance feedback.
In Figure 11, for example, when the patient is performing pelvic floor muscle contractions, the quantified results, such as P1 and P2, use the k-NN algorithm to find the nearest neighbors of P1 and P2. Of P1's seven nearest neighbors, there are four neighbors in the cluster 4, two in cluster 3, and only one neighbor in cluster 1. Therefore, P1 is classified as cluster 4; it is an incorrect contraction action. Thus, the proposed system will send a warning message to the patient. Of P2's seven nearest neighbors, four are in cluster 1, and three are located in cluster 4; therefore, P2 is classified as belonging to cluster 1 and is a correct pelvic floor muscle contraction.

The classification of two pelvic floor muscle contractions P1 and P2.
During the last phase, the doctor can follow a patient's rehabilitation progress through charts, in terms such as whether the patient has committed to daily rehabilitation, whether performed pelvic floor muscle contractions are correct or not, and so forth. A rehabilitation data in 15 days is shown in Figure 12. When the patient returns to the hospital, the doctor can adjust the course of rehabilitation to help patients accelerate recovery.

A rehabilitation data in 15 days.
5. Conclusions and Future Work
Because of privacy issues, many patients reject the invasive treatment of urinary incontinence treatment. Therefore, patient rehabilitation is quite slow in progress [23].
In this study, we use wireless sensors to develop a noninvasive PFMT device for use in a treatment system. This study has two main objectives. First, the patient can do PFMT exercise, at home and without the assistance of doctors or nurses, by using the proposed system; the system can analyze patient rehabilitation sensor data in real time, and patients can determine whether their rehabilitation actions are correct or not and adjust their own rehabilitation actions accordingly to improve the effectiveness of rehabilitation.
Secondly, to deliver better medical care to patients, the system can assist doctors in collecting sensor data, understanding the patient's rehabilitation process, adjusting the course of treatment, and helping patients to improve rehabilitation exercise.
Currently, we have made 20 sets of devices to provide the doctors of the Taipei Veterans General Hospital, Taiwan, for clinical trials. In the future, we will continue to collect patients' feedback to improve our system. Moreover, we will develop new devices and systems to help patients who are ill-suited for standing do PFMT exercise. From a longer-term point of view, we desire to build a more intelligent system that patients can handle by themselves. It will improve the utility of home rehabilitation.