
Abstract
To combat the nationwide opioid epidemic, many states have implemented policies that require prescribers to check a patient's prescription history with Prescription Drug Monitoring Programs (PDMPs) prior to initiating or refilling opioid prescriptions. Using a difference‐in‐differences approach, we show that after states mandated PDMP use, opioid prescriptions decreased by 6.1% as intended. However, PDMP mandates had the unintended effect of driving existing opioid users towards more lethal illicit substitutes such as heroin. We found that reductions in prescription rates were accompanied by unprecedented rises in heroin overdose deaths: there were 6.37 more heroin‐related deaths per million population per year—a 50.1% increase—following PDMP mandates. Although stronger PDMP mandates (e.g., based on comprehensiveness, legal enforcement, integration with other health records, and interstate information sharing) reduced opioid prescriptions, we also find that stronger mandates inadvertently increased heroin overdose deaths. Additional analyses show that the substitution effect was not statistically significant among states with lower preexisting levels of pain reliever dependence, lower heroin availability, and greater access to substance abuse treatment. These findings point to an important policy implication: supply‐side restrictions such as mandated PDMP need to account for possible demand‐side substitution effects.
INTRODUCTION
The United States is in the middle of an opioid epidemic. There are currently over 2 million individuals with opioid use disorder (OUD), characterized by chronic abuse of prescription opiates; over 4 million people over the age of 12 have used pain medicines recreationally in recent years (Center for Behavioral Health Statistics and Quality, 2018); every day, more than 130 people die from an opioid overdose (CDC, 2018), and various regions of the country report daily increasing opioid fatalities (Vivolo‐Kantor et al., 2018). Physician overprescribing of opioids has been implicated as a primary driver of the nationwide opioid epidemic; many patients who are introduced to prescription opioids, usually for pain management, go on to display a pattern of escalating usage or substitution to more potent and dangerous alternatives (Compton et al., 2015; Meldrum, 2016). Furthermore, there is widespread evidence of doctor shopping, where a patient will seek opioid prescriptions from multiple physicians who may not be aware of the duplicate prescriptions. Easy access to prescription opioids can further exacerbate opioid dependence and abuse.
For these reasons, policies to combat the opioid epidemic have primarily focused on placing curbs on physician prescribing. Although a provider will be able to view historical prescriptions for a given patient using electronic health records (EHR) within their facility, because of a lack of interoperability of EHR systems (Kellermann & Jones, 2013), providers are not able to view prescriptions made at other healthcare facilities. To overcome this limitation, policies have recently focused on electronically sharing prescribing information. In particular, many states have proposed state‐wide electronic sharing of prescription information, with the intent of allowing providers greater oversight into individual patient prescribing. One of the most significant sets of such policies is the Prescription Drug Monitoring Program (PDMP), which has been implemented across many states. PDMPs entail the state‐wide electronic sharing of patient‐level prescribing information regarding controlled substances among providers, pharmacies, and law enforcement officials. During our study period, 19 states legally mandated prescribers to query the PDMP system prior to writing for controlled substances.
In this paper, we examine whether mandating the electronic sharing of prescription information has helped curb the opioid epidemic. Specifically, we consider both the demand (patient‐side) and supply (provider‐side) effects created by the health IT policy implementation. First, we examine how the intervention changes provider prescribing. Prior research has shown that the adoption of electronic health information systems depends on the perceived value, changes to organizational routines, and legal enforcement (Ben‐Zion et al., 2014; Hansen & Baroody, 2020; Yaraghi et al., 2015). Since some state programs allow providers' and pharmacists' discretion in whether to query PDMP, it is not clear how prescribing behavior will change following the implementation of the policy. In particular, the effectiveness of the policy may depend on the level of enforcement. Second, it is not fully understood how patients respond to the supply‐side restrictions. Prior work in examining the choice behavior of individuals has shown that when presented with choice restrictions, rather than limit consumption, individuals simply seek out alternatives (DiNardo & Lemieux, 2001; Mark Anderson et al., 2013; Powell et al., 2018; P. Wang et al., 2019; Y. Wang et al., 2016). In the context of the present study, it is critical to assess whether any curb on the supply of prescription opioids leads to an overall reduction in opioid consumption or whether patients simply seek out illicit alternatives (e.g., heroin).
To answer these questions, we construct a national panel dataset consisting of detailed information on opioid prescribing, as well as incidences of prescription opioid and heroin deaths from all states in the United States between 2006 and 2015. To identify the causal effects of mandated PDMP use on opioid prescription and overdose deaths, we employ a quasi‐experimental design that exploits the variation in the implementation of the policy across the different states at different times. We also test the sensitivity of our findings to a battery of robustness checks using alternative model specifications and data inclusion criteria to account for potential confounders.
Our detailed empirical analysis leads to the following results. First, we find that mandated PDMP use decreased opioid prescriptions as intended. On average, prescriptions for opioids declined by 6.1% following the implementation of the policy. However, despite the reduction in prescriptions, the policy did not reduce prescription opioid deaths. Perhaps more surprisingly, heroin‐related deaths increased substantially—by 50.1%—following PDMP mandates. Since heroin is an illicit substitute for prescription opioids, our finding suggests that placing supply restrictions for prescription opioids may have led patients to seek out a more dangerous, illicit alternative unaffected by the PDMP policy change. We find additional corroborating evidence from an analysis of Google Trends: keyword searches for prescription opioids (oxycodone and prominent brand names, OxyContin and Vicodin) decreased postpolicy while searches for heroin increased significantly.
Finally, the degree of substitution to heroin varied across PDMP mandate implementations; states with more restrictive PDMP mandates (e.g., comprehensiveness, legal enforcement, integration with other health records, and interstate information sharing) saw a more dramatic reduction in the prescription rate, but also a greater increase in heroin overdose deaths. In addition, prepolicy local environmental conditions moderated the effect of the policy implementation; substitution to heroin was not statistically significant among states with lower preexisting levels of pain reliever dependence, lower heroin availability, and higher substance abuse treatment facility availability.
This set of findings has several managerial and policy implications. First, although mandating PDMP reduces opioid prescriptions, the resulting supply restrictions lead to a significant increase in heroin deaths. Prescription opioid death rates did not significantly decrease in our sample; however, the increased heroin deaths are an unintended and undesirable public health outcome that policymakers should be mindful of.
Second, although more restrictive policies further reduce opioid prescriptions, stronger PDMP mandates lead to higher rates of heroin deaths. For example, policies requiring EHR integration and interstate sharing have the effect of further restricting the supply of legal prescription opioids. Unfortunately, they also spur greater substitution for heroin.
Third, the unintended substitution effects can be mitigated in several ways. For example, areas with low heroin availability and high OUD treatment facility capacity did not experience significant substitution for heroin under mandated PDMPs. This suggests that restricting the availability of illicit substances through increased policing, for example, and investing in OUD treatment capacity can mitigate the unintended consequences of PDMP mandates. Hence, in addition to supply‐side restrictions, it is critical that policymakers also consider demand‐side solutions such as expanding treatment and rehabilitation capacity.
The rest of the paper is organized as follows. In the next section, we provide a brief background of the opioid epidemic and the electronic prescription sharing policy in question. In Section 3, we present our hypotheses for the anticipated effect of the policy. Section 4 describes our data, and Section 5 presents the empirical specifications. In Section 6, we present our main results, and in Section 7 we conclude.
BACKGROUND AND RELATED LITERATURE
Research setting
A recent National Survey on Drug Use and Health (NSDUH) found that more than one‐third of U.S. civilian, noninstitutionalized adults reported prescription opioid use, with substantial numbers reporting misuse and use disorders (Vivolo‐Kantor et al., 2018). One of the most significant sets of policies deployed to combat the opioid epidemic has been PDMPs. Nearly all states have established PDMPs, which implement electronic databases that aggregate and facilitate the sharing of data on opioid prescriptions. Originally funded by the U.S. Department of Justice, PDMP was conceived as a tool of law enforcement to identify rogue prescribing operations (or “pill mills”) and other egregious or illegal prescribing practices. However, when PDMPs were initially rolled out, the systems were not user‐friendly or easily accessible, leading to low prescriber compliance. An early report shows that the median PDMP registration rate among licensed prescribers who issue at least one controlled substance prescription was 35% (Kreiner et al., 2014). Partly due to the low utilization, the effect of this policy has been modest or limited (Ali et al., 2017; Meara et al., 2016). In response, many states have recently mandated PDMP use, and measuring the effect of the mandate is the focus of this study.
During our study period, 19 states mandated PDMP use. These mandates, which are often legally enforced require prescribers to check with the PDMP system prior to initiating or refilling prescriptions for opioids. The strength of the mandate varies across states. Some states only mandate PDMP use for specific conditions; for example, Louisiana's law applies only to pain clinics, and Vermont's only to a specific opiate (buprenorphine). Some states allow subjective judgment in mandating PDMP use—Nevada, Delaware, and Ohio require that providers query the PDMP only if they suspect that the patient may be seeking controlled substances for any reason other than the treatment of an existing medical condition. In contrast, states like Kentucky and New York have the most stringent mandates—all prescribers must query the PDMP prior to prescribing any opioids.
By reducing the number of individuals introduced to opioids, the policy intervention was intended to help contain the opioid epidemic. However, although the policy intervention may slow the growth of new prescription opioid users, it may not help alleviate the suffering of millions of existing users already struggling with OUD. Mandating PDMP use may in fact inadvertently harm existing OUD suffers in two ways. First, the sudden lack of access to prescription opioids (and the debilitating withdrawal symptoms) may force users to turn to “street drugs” like heroin that have become increasingly accessible. These drugs are pharmacologically similar to prescription opioids, producing even greater sensations of euphoria and pain relief (Compton et al., 2016). Moreover, these illicit drugs lack oversight on quality in terms of toxicity and potency, and once a user starts taking them it becomes easier for the abuse to escalate further.
Second, drugs used in medication‐assisted treatment (MAT) that have been found to be effective in treating opioid addiction contain opioids (Volkow et al., 2014) are also subject to PDMP mandates (Brandeis PDMP CoE, 2016). Consequently, patients who are being treated for OUD might have difficulty obtaining prescriptions for treating their addiction. 1 Collectively, these factors could push existing opioid patients into seeking illicit substitute drugs such as heroin. However, there are also personal risks, costs, and legal consequences that can deter individuals from seeking illicit street drugs. How these two sets of opposing forces play out at the population‐level heroin remains an empirical question.
Related literature
There are several streams of literature that are relevant to our research question. Kelly et al. (2008) conducted a large‐scale phone survey and reported that regular opioid users often used opiates in conjunction with proton pump inhibitors and antidepressants. More recent studies have highlighted the addictive nature of prescription opioids and their devastating effect on public health. For example, Han et al. (2015) reported substantial increases in nonmedical use of prescription opioids and related death rates between 2003 and 2013. Studies have also examined the role of environmental factors in the use of prescription opioids. Shah et al. (2017) and Sun et al. (2016) identified that certain types of surgeries, gender, age, history of substance abuse, depression, and the length of opioid prescription regimen are significantly associated with chronic opioid use.
The intended goal of PDMP is to address chronic opioid misuse, and several studies have examined the effectiveness of PDMP using EHR and claims data. Bao et al. (2016, 2018), Haffajee et al. (2018), and Rutkow et al. (2015) reported decreased opioid prescriptions following the implementation of PDMP. Buchmueller and Carey (2018) reported that the mandated PDMPs reduce the misuse of prescription opioids in the Medicare population. Although our study also considers the effect of PDMP on prescription opioids, our primary focus is on examining the substitution for heroin.
A notable trend coinciding with the efforts to reduce opioid prescriptions is the increased rates of heroin use and overdose (Compton et al., 2016). A retrospective analysis of heroin use in the United States shows that among those who began abusing opioids in the 2000s, 75% of respondents indicated they started with prescription opioids (Cicero et al., 2014). The most commonly cited reasons for the switch to heroin were (1) heroin became more accessible and significantly cheaper, (2) it was easier to inhale or inject, and (3) its potency was much greater than that of prescription opioids (Cicero et al., 2014; Mars et al., 2014; Unick et al., 2014). Deiana and Giua (2021) find that regulations restricting the supply of prescription opioids were accompanied by negative externalities in the local market for illicit drugs, measured by opium possession and sales arrests.
In addition to prescription rates, opioid‐related deaths have become an important metric in understanding the evolution of the epidemic (Haffajee et al., 2015). Some studies have found that the tamper‐proof reformulation of OxyContin that was intended to address overprescribing may have contributed to heroin use and death (Alpert et al., 2018; Cicero et al., 2012; Dart et al., 2015; Evans et al., 2019). On the other hand, Patrick et al. (2016) found that the implementation of PDMP decreased opioid‐related overdose death rates using data up to 2013 in 34 states. 2
We contribute to the extant literature on the opioid epidemic in the following ways. First, we collect data from multiple sources over a longer period of time compared to prior studies. This allows us to generate differences‐in‐difference estimates that control for a larger set of confounders and over a longer period of time. A rigorous replication of the prior finding that PDMP laws reduce physician overprescribing can provide greater confidence that PDMP laws have worked as intended. Second, the impact of PDMP laws on substitution with other opioids such as heroin has been relatively understudied and needs to be examined in more detail. Third, in order to better understand the substitution to heroin, we examine whether the strength of PDMP implementations exacerbates the substitution to heroin. Fourth, we examine whether local environmental conditions such as easy access to heroin or the availability of substance abuse treatment facilities mitigate the substitution effect. Any findings on the role of environmental factors can inform clear policy choices such as increased policing targeted to reduce heroin sales or investments in OUD treatment capacity. Fifth, we explore keyword search data from Google Trends to understand user search behavior associated with the substitution from prescription opioids to heroin and to corroborate the large‐scale findings using end‐user behavior.
We next formally establish the hypotheses on how the policy may impact opioid prescription and heroin‐related deaths, with specific attention to the heterogeneity among the policy implementations.
HYPOTHESIS DEVELOPMENT
A growing body of research has examined the adoption of healthcare information technology (HIT) in improving care delivery. Early evidence indicated that the implementation of EHR, for example, had no effect on the quality of care (McCullough et al., 2016). More recent research, however, has led to findings that HIT drives improvements in care delivery. For example, Angst et al. (2011) and Forgionne and Kohli (1996) showed that the adoption of HIT led to a reduced patient hospital stay. Buntin et al. (2011) and Jones et al. (2014) found HIT to be associated with improvements in patient safety and satisfaction, as well as efficiency of care. Electronic medical records (EMR) have also helped in identifying high‐risk patients (Amarasingham et al., 2010) and have resulted in interventions that improved the quality of care as evidenced by fewer hospital readmissions (Bardhan et al., 2015).
Studies have also noted benefits of HIT in primary care. Chaudhry et al. (2006) conducted a systemic review and reported benefits of HIT in terms of increasing adherence to guidelines, enhancing disease surveillance, and decreasing medication errors. Lu et al. (2018) found that the adoption of HIT can enhance the automation of nursing tasks and improve clinical quality in nursing homes. Hydari et al. (2019) showed that advanced EMRs led to a 17.5% decline in patient safety events, mainly driven by reductions in medication errors and complication errors.
A recurring complaint of HIT and EHR, in particular, has been the lack of interoperability across healthcare organizations. That is, electronic records for a patient seen at hospital A may not be easily accessed by a physician caring for the same patient at hospital B in a subsequent encounter. This lack of interoperability can inhibit continuity in care delivery and potentially compromise patient health. In contrast, being able to maintain continuity of care has been associated with improved clinical outcomes (e.g., see Ahuja et al., 2020).
In contrast, PDMP systems allow information sharing among different providers. This not only facilitates the identification of high‐risk patients across healthcare facilities but also allows physicians to maintain continuity across multiple episodes of care. By enabling cross‐provider information sharing and allowing greater visibility into the medical history of the patient, health information exchanges such as PDMP can facilitate more effective care delivery. For example, Winden et al. (2014) pointed out that health information exchange can help providers by offering a more complete view of the medication history of patients. Such information sharing can lead physicians to identify potential high‐risk opioid dependency and misuse and to refrain from prescribing opiates.
Finally, compliance with mandated HIT systems such as PDMP also offers providers protection against liability claims. For example, Sharma et al. (2019) showed that the use of HIT systems reduced the number of legal lawsuits against providers. In particular, hospitals with higher adoption levels were more effective at reducing lawsuits. Given increasing scrutiny against providers for opioid overprescribing, the mandated use of PDMP systems may also offer providers protection against legal action.
Collectively, the ability to share patient information across providers, the ability to identify high‐risk individuals, and the defense against legal action suggest that mandated PDMP use should reduce prescription opioids. Mandating PDMP use reduces opioid prescription rates.
The impact of policies designed to curb the consumption of addictive substances has been documented extensively in the literature. For the most part, placing restrictions on the access and cost of substances has led to not only reduced consumption but also socially desirable outcomes. For example, increasing the minimum drinking age has been found to reduce alcohol consumption among high school students (DiNardo & Lemieux, 2001); cigarette excise taxes and antismoking advertising have been found to be effective at reducing cigarette sales (Y. Wang et al., 2016); restricting weekend alcohol sales has led to fewer traffic fatalities (McMillan & Lapham, 2006).
However, restrictions on addictive substances have also had unintended consequences, most notably increased spillover demand for close substitutes. The academic literature, for instance, has identified substitution between alcohol, marijuana, and prescription opioids. For example, an increase in the minimum drinking age was found to decrease the prevalence of alcohol consumption but also unintendedly increase marijuana consumption (Crost & Guerrero, 2012; DiNardo & Lemieux, 2001), suggesting that users started abusing marijuana when access to alcohol was limited. Similarly, broader access to medical marijuana appears to have facilitated the substitution of marijuana and away from more powerful and addictive opioids (Powell et al., 2018).
Although users may substitute for less harmful substances, in some cases the substitute may be more lethal. For example, even though excise taxes reduced cigarette consumption in aggregate, users responded by selecting cigarette brands with higher nicotine content (Y. Wang et al., 2016). Similarly, the widespread abuse of OxyContin (the brand‐name prescription containing the opioid oxycodone) led to the release of a tamper‐proof reformulation of the drug. Unfortunately, the introduction of the abuse‐deterrent version of OxyContin had the unintended effect of driving users towards lethal opioid substitutes, including heroin (Alpert et al., 2018; Evans et al., 2019).
In the context of our study, the sudden lack of access to prescription opioids (and the debilitating withdrawal symptoms) due to PDMP mandates may force users to turn to street drugs such as heroin that are relatively easy to obtain. These illicit drugs are pharmacologically similar to prescription opioids, producing even greater sensations of euphoria and pain relief among users. These street drugs also lack checks on toxicity and potency, and once a channel to street drugs is established, it becomes easier for the abuse to escalate further. Additionally, drugs used in MAT have been found to be effective in treating opioid addiction. Unfortunately, these drugs contain opioids and are also subject to PDMP mandates. Consequently, patients who are being treated for opioid abuse might have difficulty obtaining prescriptions for managing their addiction. Collectively, these factors could push existing opioid patients into seeking illicit street drugs. Mandated PDMP use leads to greater abuse of heroin.
Although PDMP mandates have been implemented across many states, there are varying levels of implementation. The strength of implementation in turn can impact medical prescriptions of opioids as well as subsequent spillovers into heroin. There are four primary dimensions along which we evaluate the strength of implementation: comprehensiveness, provider immunity, integration with EHR, and degree of interstate information sharing.
First, we consider the comprehensiveness of PDMP mandates. As discussed in Section 2, guidelines on PDMP mandates have varied from state to state. In some states, the guidelines have been loose; for example, providers are required to reference the PDMP database only if they suspect that the user is doctor shopping. In other states, providers are instructed to use PDMP only for specific prescription opiates. However, a handful of states have implemented comprehensive PDMP mandates, for example, providers must query all patients prior to prescribing any opioids. These comprehensive mandates represent the strictest guidelines, and we posit that the states implementing the comprehensive mandates have a stronger form of PDMP.
Second, the degree of legal enforcement can strengthen the effectiveness of PDMP. Specifically, state laws vary in their degree of immunity grants, which protect providers from civil and criminal liability if they fail to review the PDMP data prior to prescribing. Legal actions against overprescribers have recently received increased attention in the media, and the liability costs associated with such action can be particularly high (Sharma et al., 2019). Immunity grants protect providers against such punitive outcomes. As such, in states that have nonexistent immunity grants, providers may have a greater impetus to comply with PDMP laws.
Third, the extent to which PDMPs integrate with EHRs varies across states. PDMPs only contain information regarding controlled substance prescriptions, when they are integrated with EHRs, providers may be able to further identify risk factors for OUD based on previous surgery history or addictive behavior related to noncontrolled substances such as alcohol and tobacco (Ellis et al., 2019). In addition, without integration with EHRs, prescribers need to manage multiple disconnected software systems resulting in interruption of the clinical workflow—a factor that has been a barrier to the use of PDMPs (Holmgren & Apathy, 2020; Rutkow et al., 2015). Therefore, integration with EHRs enables prescribers to coordinate care across systems and work more effectively.
Fourth, the degree of PDMP information sharing varies across states. Some states allow only within‐state sharing of the prescription information, whereas other states have collaborated to allow interstate sharing. Users who live in states that do not collaborate with other states can easily cross state borders to seek out‐of‐state prescriptions. The ability of users to find alternative sources of prescription opioids can severely restrict the efficacy of PDMP laws.
Such cross‐shopping across state boundaries has been observed in a number of settings; for example, Seiler et al. (2021) have found that an increase in tax on sweetened beverages reduced sales in the focal region, but increased sales in neighboring regions that did not see the same tax hike; increasing taxes on alcohol (Conlon & Rao, 2015, 2020; Miravete et al., 2018, 2020), cigarettes (Harding et al., 2012; Lovenheim, 2008; Merriman, 2010), and cannabis (Hollenbeck & Uetake, 2021; Jacobi & Sovinsky, 2016) have had similar geographic demand spillover effects.
The spillover can have unintended socioeconomic costs. For example, Lovenheim and Slemrod (2010) found that an increase in a state's minimum legal drinking age led to an increase in fatal accidents for 18–19 year‐olds in that state living within 25 miles of a jurisdiction with a lower drinking age. Similarly, Jacks et al. (2021) found that the repealing of prohibition in select counties in the 1930s contributed not only to an increase in infant mortality in those counties but in neighboring (dry) counties as well.
Given the relative ease with which users can travel across state borders, we posit that PDMP laws that facilitate information sharing across state borders will be more significant deterrents to users who may otherwise be inclined to seek out‐of‐state prescriptions.
Collectively, we posit that stronger PDMP laws, as reflected in a higher degree of comprehensiveness, lack of immunity for prescribers who violate PDMP laws, integration with EHR, and greater spatial information sharing achieved through interstate information sharing, are more effective at reducing opioid prescription. Stronger PDMP mandate laws, as indicated by high comprehensiveness, lower prescriber immunity, integration with EHR, and greater interstate information sharing, lead to lower prescriptions for opioids.
The lowered prescription rate may in turn lead patients—particularly those who have become dependent on prescription opiates—to seek out illegal alternatives like heroin. We posit that the unintended spillover effect will be particularly strong in states with the strictest form of the law. Stronger PDMP laws, as indicated by high comprehensiveness, lower prescriber immunity, integration with EHR, and greater interstate information sharing, lead to greater spillover demand for heroin.
DATA AND DESCRIPTIVE STATISTICS
Data
We collect opioid prescribing data from the QuintilesIMS Transactional Data Warehouse, which provides information on the number of opioid prescriptions dispensed at 59,000 pharmacies that collectively represent 88% of prescriptions in the United States (QuintilesIMS, Raleigh, North Carolina, USA).
We obtain prescription opioid‐ and heroin‐related death rates (per million population) from the Multiple Cause of Death data field in the Wide‐Ranging Online Data for Epidemiologic Research (WONDER) database maintained by the Centers for Disease Control and Prevention (CDC). 3 We gather state‐level data for a 10‐year period during which the major expansion of PDMP mandates initially occurred (2006–2015).
For each state‐year, we first count the total opioid‐related overdose deaths as those showing drug overdose as the principal cause. Specifically, we use the International Statistical Classification of Diseases and Related Health Problem, Tenth Revision codes (ICD‐10) X40‐44, X60‐64, X85, and Y10‐14 and any mention of an opioid as contributing cause of death (T40.0, Opium; T40.2, Other opioids; T40.3, Methadone; and T40.4, Other and unspecified synthetic narcotics), including heroin (T40.1). We also separately count prescription opioid‐related deaths with the related ICD‐10 codes. 4 Finally, we estimate the total heroin‐related deaths by subtracting the prescription opioid‐related deaths from the total opioid‐related deaths in the first step above. This sequence of steps allows us to circumvent data suppression in the WONDER database when heroin‐related death counts are small. Lastly, we compile the death rates in all 50 U.S. states and the District of Columbia. We exclude North Dakota in 2006, 2011, and 2012 due to data inconsistency, consistent with prior studies (Dowell et al., 2016; Patrick et al., 2016).
We also gather data from Google Trends 5 to assess public interest in specific opioids over time. Google Trends measures a topic's total searches relative to all searches on all topics and reports search intensity scaled from 0 to 100 during specified time periods in a given region. For each state, we obtain monthly search trend data between January 2006 and December 2015, querying five opioid‐related search terms individually: heroin, the two most popular prescription opioid active ingredients (oxycodone and hydrocodone), and common corresponding pain medication brand names (OxyContin and Vicodin), respectively.
To account for demographic and socioeconomic factors associated with drug usage, we collect data on population size, age and gender composition, racial composition, unemployment rate, education, income, and poverty level from the American Community Survey for all the states in each year between 2006 and 2015. We also collect local crime data from the Uniform Crime Reporting Program and the number of active substance abuse treatment facilities from the National Survey of Substance Abuse Treatment Services.
Our treatment is the set of states post mandated PDMP use, where prescribers are required to check the PDMP prior to initiating opioid prescriptions or refilling them. We obtain the data on state‐specific implementations of mandated PDMP usage from Haffajee et al. (2018). During our study period, a total of 19 states mandated the use of PDMP (Table 1).
Mandated PDMP use by states
Note: The law effective date, as well as its comprehensiveness and immunity requirement, were reported based on the review of laws in Haffajee et al. (2018). The list of states that have been funded by the Substance Abuse and Mental Health Services Administration (SAMHSA) through integrating the PDMP with EHRs was based on CDC (2017). Information on states' interstate data sharing was obtained from the survey conducted by the Center for Excellence at Brandeis University (PDMP TTAC, 2015).
We use data from 2006 to 2015 to examine the short‐term effects of the focal policy change. We chose this time frame because, after 2015, more potent synthetic opioids such as fentanyl became key contributors to overdose deaths and correctly attributing the cause of death in available datasets became challenging for several reasons. First, unlike heroin, there is no separate diagnosis code for deaths related to fentanyl; the cause of death is often coded as “other and unspecified synthetic narcotics.” Second, this catch‐all code includes deaths related to both prescribed and illegal versions of fentanyl. Further, heroin was often laced with fentanyl as fentanyl became prevalent, in which case the associated death was being attributed to fentanyl instead of heroin. Therefore, we use data up to 2015 to avoid these coding issues related to the onset of fentanyl. As a robustness check, we combined heroin deaths and deaths related to other and unspecified synthetic narcotics as the outcome measure in more recent data and found a greater effect size (see Supporting Information Table A10).
Descriptive statistics
States requiring providers to review the PDMP system before prescribing opioids are labeled “treatment states,” and states that do not implement such policies during our data period are labeled as “control states.” As depicted in Figure 1a, prior to 2010, only one state (i.e., Nevada) required providers to query the PDMP database before prescribing opioids. Starting from 2010, the number of treatment states dramatically increased and totaled 19 by the end of our study period.
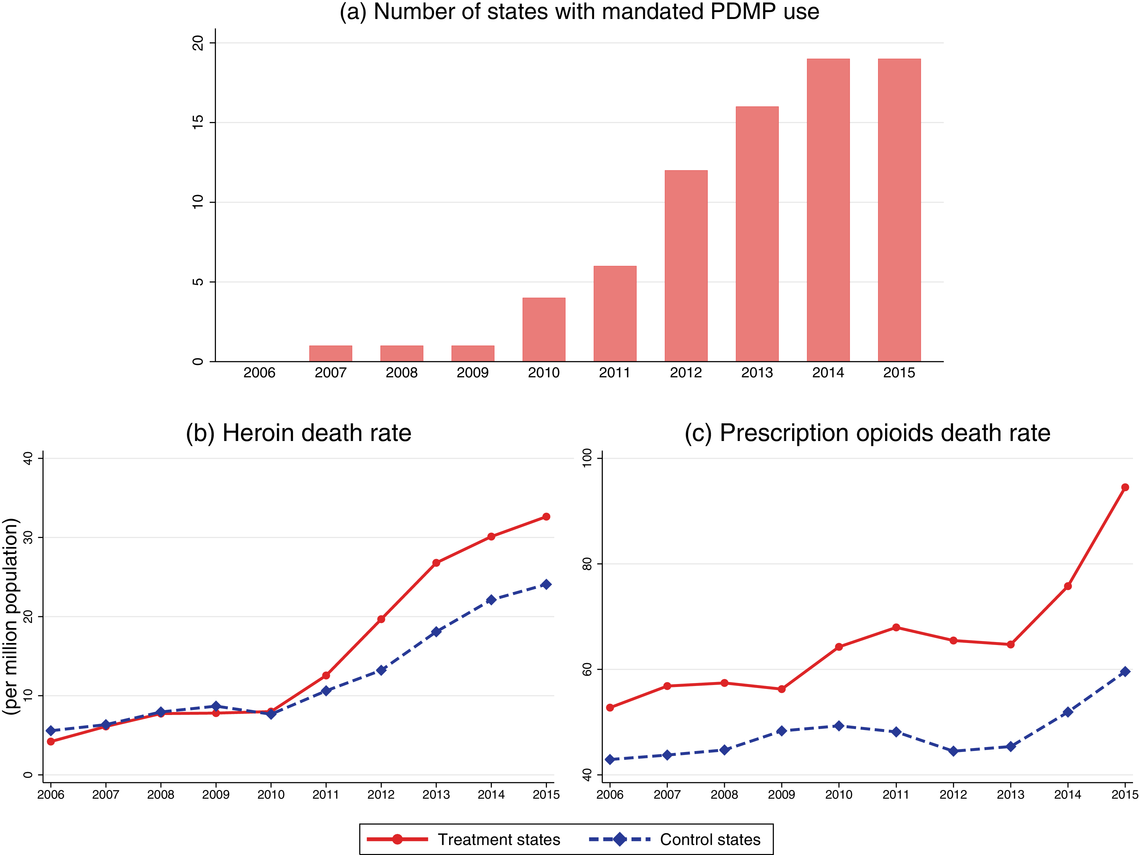
Number of states with mandated PDMP use and trends of prescription opioid and heroin death rates in states with and without mandated PDMP use, 2006–2015. Note: The number of states with mandated PDMP use was calculated based on the law implementation date shown in Table 1. Death data were obtained from the Multiple Cause of Death data field in the Wide‐Ranging Online Data for Epidemiologic Research (WONDER) database, 2006–2015
Figure 1b shows the primary outcome of this study, that is, the trend of heroin‐related overdose death rates for treatment states and control states. Until 2010, heroin overdose death rates for the two groups are similar (5.8 vs. 6.3 per million population, 

However, we do not find such divergence in prescription opioid overdose deaths. As Figure 1c shows, prescription opioid‐related overdose death rates are substantially higher in treatment states than in control states (77.7 vs. 53.8 per million population, 
Patterns in Figure 1b,c hold even after controlling for state‐specific and year‐specific factors using fixed effects (see Supporting Information Figure A1). In particular, we note that the timing of heroin‐related deaths rising sharply coincides with the increasing number of states mandating PDMP use, which suggests a positive relationship between the law implementation and heroin deaths. We further explore the identification of this relationship in the sections given below.
EMPIRICAL MODELS
To quantify the effect of state‐mandated PDMP use, we use a difference‐in‐differences econometric model. Our outcomes of interest include opioid prescription, opioid overdose death, and heroin overdose death rates. For each of the outcomes, we estimate the following regression model:





An important assumption underlying our difference‐in‐differences estimation is that in the prepolicy period states that mandated PDMP use is similar to those that do not. We test this assumption by using an event study framework. The event study sets the policy implementation year of each state to a baseline reference time of zero, in order to examine the temporal difference between treatment and control states in the pre‐ and postpolicy periods. The estimated function is as follows:





RESULTS
Mandated PDMP use on prescriptions and death rates
Table 2 presents the results of our analyses (Equation 1). In column 1, we estimate that after mandating PDMP use, states experienced a reduction in opioid prescriptions by 4.96 per 100 persons, amounting to a 6.1% decrease compared to the overall average rate of 81.97. This suggests that the policy was effective in limiting access to prescription opioids as intended, supporting Hypothesis 1. 6 Furthermore, we find that the PDMP mandates resulted in 6.37 more heroin overdose deaths per million population per year (see column 3). Compared to the overall average rate of 12.72 per million population, our estimate corresponds to a 50.1% increase in heroin overdose deaths. This result provides support for Hypothesis 2—by reducing prescription opioids, PDMP mandates have inadvertently led prescription opioid users to abuse heroin instead.
Effects of mandated PDMP use on prescription rate and overdose deaths
Note: Model controlled for state fixed effects and year fixed effects. Standard errors were clustered at the state level.
*p < 0.1; **p < 0.05; ***p < 0.01.
We also estimate event studies (Equation 2) and present estimated coefficients for dummies of the timing relative to the policy change in Figure 2. We note that the estimated coefficients for the opioid prescription rate and heroin death rate are not statistically significant in years before the mandated PDMP use. This demonstrates that there are no systematic differences in the prepolicy trends between treatment and control states, providing support for the key parallel trends assumption underlying the difference‐in‐differences model. Consistent with our prior observations, the opioid prescription rate decreased significantly for treatment states in the postimplementation period (Figure 2a). In addition, there is a growing increase in the heroin death rate for treatment states in the postimplementation period, with the magnitude of this effect becoming larger in the second and third years (Figure 2b). This suggests that the impact of mandated PDMP use on heroin overdose deaths is likely to grow over time.
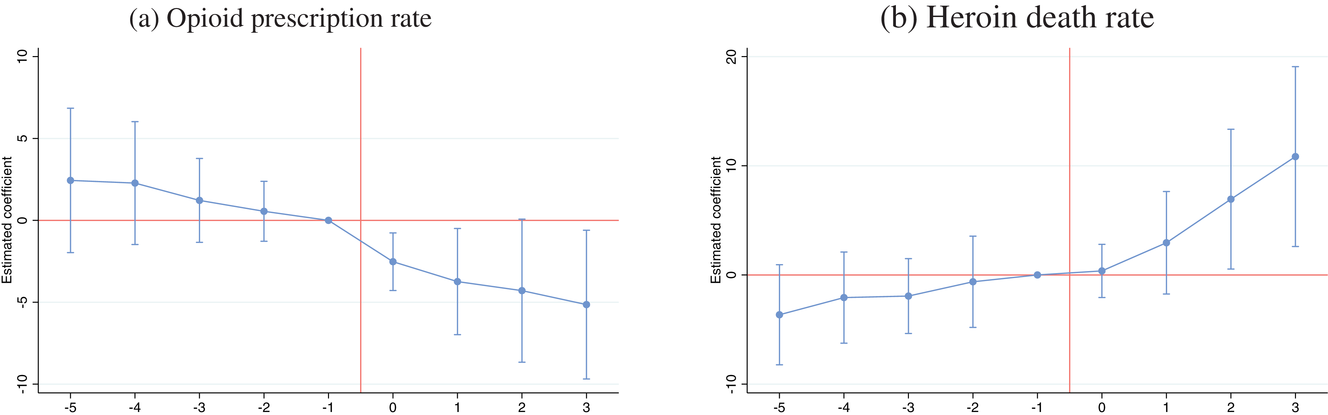
Effect of mandated PDMP on prescriptions and heroin overdose deaths. Note: Each graph shows the point estimates based on the event study with the 95% confidence intervals, adjusted for within‐state clustering. The year of mandating the PDMP use is normalized to 0
How do the effects vary by the strength of the law?
We assign states into “strong” and “weak” treatment categories based on the following four criteria (see Table 1). First, within the treatment states, the stipulations for which prescribers are required to review a patient's prescription history vary from state to state. In some states, for example, providers should access the PDMP only if they suspect that the patient may be seeking the controlled substances for reasons other than the treatment of an existing medical condition. Some states have limited laws that apply only to certain ingredients (methadone in Oklahoma, buprenorphine in Vermont) or settings of care (pain clinics in Louisiana). In contrast, there are four states that specify objective criteria for checking the PDMP (rather than based on subjective beliefs) and cover a broad array of prescribing contexts (not limited to certain ingredients or settings of care). States with such comprehensive use mandates—Kentucky, New Mexico, Tennessee, and New York—are labeled as the strong group, while the rest of the treatment states are assigned to the weak group category. Second, state laws differ in their conditions of immunity grants. Some state PDMPs have immunity grants that protect prescribers from civil and/or criminal liability if they fail to review the PDMP data prior to prescription. These grants may relax the impetus on prescribers to check the database since there is no penalty associated with failure to do so. We categorize the treatment states that do not have immunity grants as the strong group. Third, some states have been funded by the Substance Abuse and Mental Health Services Administration (SAMHSA) to promote PDMPs to integrate with EHRs. Interoperability within the workflow is crucial to streamline provider access and use, which enables PDMPs to work more effectively. States with EHR integration are characterized as strong states. Finally, many states have improved the PDMP reports by initiating interstate data sharing with regional neighbors, in an effort to thwart drug abusers and traffickers from crossing state lines to obtain prescription drugs. We define treatment states that enabled exchanging of PDMP data across state boundaries as strong states.
If stronger PDMPs are effective as originally intended, we should observe a reduction in opioid prescriptions. Table 3 presents the results for opioid prescription using subsample analysis. In general, we note that states with more stringent regulations experience larger reductions in the prescription rate. In column 1, we estimate that PDMP mandates lead to a reduction in opioid prescriptions by 3.54 per 100 persons in states with noncomprehensive mandate laws. In contrast, the effects are much stronger in states with comprehensive mandates, where the opioid prescription is reduced by 11.53 per 100 persons. Coefficients in column 2 suggest that treatment states with immunity have a reduction in opioid prescriptions by 4.30 per 100 persons, whereas treatment states without immunity have a reduction of 9.07 per 100 persons, compared with control states. In column 3, we estimate that treatment states that integrate PDMP with EHR have a stronger effect—PDMP mandates reduce opioid prescription by 10.91 per person in states with EHR compared to a 4.30 reduction in states without EHR. Finally, coefficients in column 4 suggest that treatment states with interstate data sharing have reduced opioid prescriptions by 7.73 per person, while the reduction is insignificant for treatment states without interstate sharing. These results provide support for Hypothesis 3 that stronger PDMP mandate laws lead to a greater reduction in opioid prescription.
Effects of mandated PDMP use on opioid prescriptions by the strength of law
Note: In each column, the sample included the “Yes” or “No” treatment states and the control states. The model controlled for state fixed effects and year fixed effects. Standard errors were clustered at the state level.
*p < 0.1; **p < 0.05; ***p < 0.01.
Results in Section 6.1 show the unintended effect of PDMP mandates on heroin deaths. This suggests that, unlike the effect on the reduced rate of opioid prescribing, stronger PDMPs may result in increased heroin deaths. Table 4 presents the estimates for heroin deaths; we see that states with stronger versions of PDMP experience a more dramatic increase in heroin deaths. For example, column 3 shows that PDMP mandates result in an increase of 20.80 heroin overdose deaths per million population in states that integrate PDMP with EHR. In contrast, PDMP mandates do not significantly impact heroin deaths in states without EHR integration. Similar patterns are observed in column 4: PDMP mandates have a greater impact on heroin deaths in treatment states that allow interstate data sharing. These results suggest that stronger PDMP laws lead to greater spillover demand for heroin, as evidenced by the increased heroin‐related deaths, supporting Hypothesis 4.
Effects of mandated PDMP use on heroin death rate by the strength of law
Note: In each column, the sample included the “Yes” or “No” treatment states and the control states. The model controlled for state fixed effects and year fixed effects. Standard errors were clustered at the state level.
*p < 0.1, **p < 0.05, ***p < 0.01.
How does the substitution effect vary by prepolicy local factors?
In this section, we discuss how the substitution of prescription opioids for heroin can be influenced by local environmental factors, including preexisting rates of opioid abuse, availability of heroin, and access to substance abuse treatment facilities.
First, prior work has shown that the shift to heroin after the reformulation of OxyContin was larger in states that had higher prereformulation recreational use of OxyContin (Alpert et al., 2018; Evans et al., 2019). Likewise, one might expect to see larger shifts from opioids to heroin in areas with more pervasive abuse of opioids before the mandated use of PDMPs. To capture the initial level of opioid abuse, we obtained data from the NSDUH 2010–2013 waves
7
on the level of pain reliever dependence. We then partition the data for treatment states into four groups based on the 
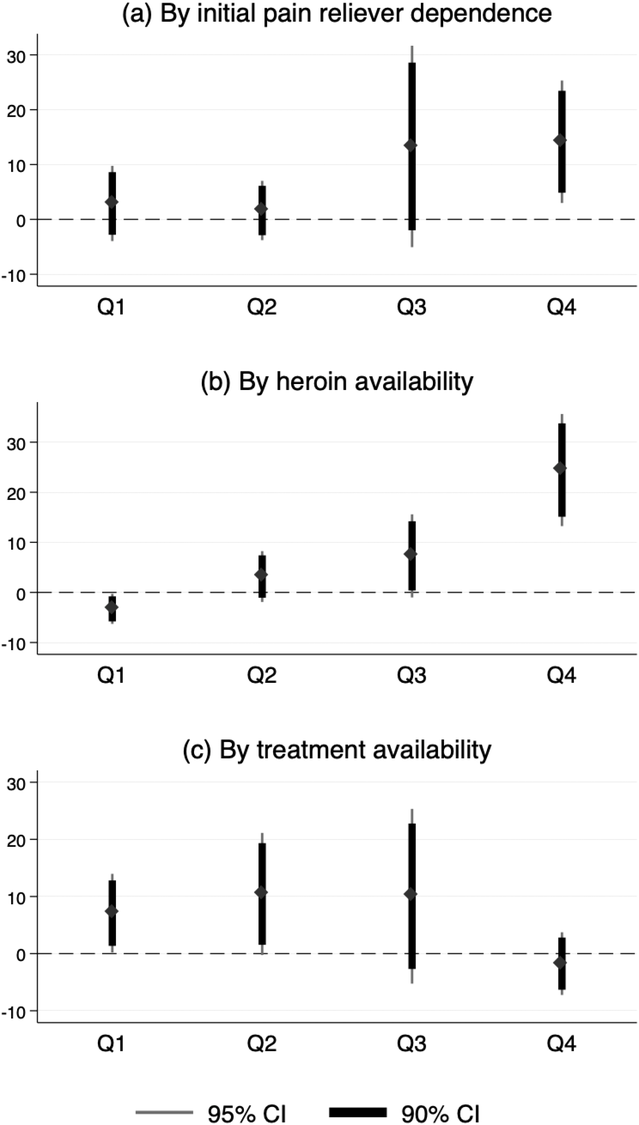
Effects of mandated PDMP use on heroin overdose deaths. Note: Each graph depicts the difference‐in‐differences estimates of the effects of mandated PDMP use on heroin overdose deaths. The treatment states are first partitioned into four groups based on the 25th, 50th, and 75th quartile points for each of the characteristics. Q1, Q2, Q3, and Q4 represent a subsample of each group of mandate states plus comparison states. The thick and thin bars represent the 90% and 95% confidence intervals, respectively
Another factor that might moderate the substitution effect is the availability of heroin (Cicero et al., 2014; Compton et al., 2016). Presumably, patients are more likely to switch from prescription opioids to heroin in areas where heroin is more easily accessible. Data on population‐level heroin availability are based on the NSDUH; the survey includes asking respondents to rate the difficulty of obtaining heroin in the past year. We focus on the proportion of people who believed heroin was easy or fairly easy to obtain during 2010–2013. 8 As shown in the lower panel of Figure 3, the substitution effects are most salient in areas with the highest availability of heroin (fourth quartile), corroborating the potential substitution to heroin upon the implementation of PDMP mandates.
Finally, we examine whether the effects on heroin deaths are attenuated by the availability of OUD treatment. To estimate this effect, we obtain the number of specialty treatment facilities offering OUD treatment services in each state from the National Survey of Substance Abuse Treatment Services data. As shown in Figure 3, the substitution effects are most salient in areas with lower levels of treatment (first and second quartiles). This suggests that providing more treatment options for patients who are already addicted can mitigate the substitution for heroin.
Mandated PDMP use and Google search trends
To corroborate the population‐level substitution of opioids for heroin, we examine data obtained from Google Trends, which allows us to assess whether the public interest in opioids changed following mandated PDMP. Figure 4 shows trends in selected keyword searches on Google between 2006 and 2015 in four states (Kentucky, Ohio, Tennessee, and Louisiana). During the months following mandated PDMP use, the level of interest for the keyword heroin trended upward, while the proportion of searches for prescription opioid brands such as OxyContin and Vicodin trended slightly downward. Table 5 presents the difference‐in‐differences (DiD) estimates. We find that the Google Trends index for heroin increased after mandating PDMP use—the search proportion of heroin relative to all searches increased by 3.21 significantly. In contrast, there were significant decreases in keyword searches for prescription opioids: oxycodone, and brand names OxyContin and Vicodin, while the change in keyword hydrocodone was not significant. These results provide support for our hypothesized mechanism that people who are unable to obtain prescribed opioids will seek out illicit opioids, as evidenced by Internet searches. 9
Effects of PDMP mandates on Google search trends
Note: Model controlled for state fixed effects and time (year and month) fixed effects. Standard errors were clustered at the state level.
*p < 0.1, **p < 0.05, ***p < 0.01.
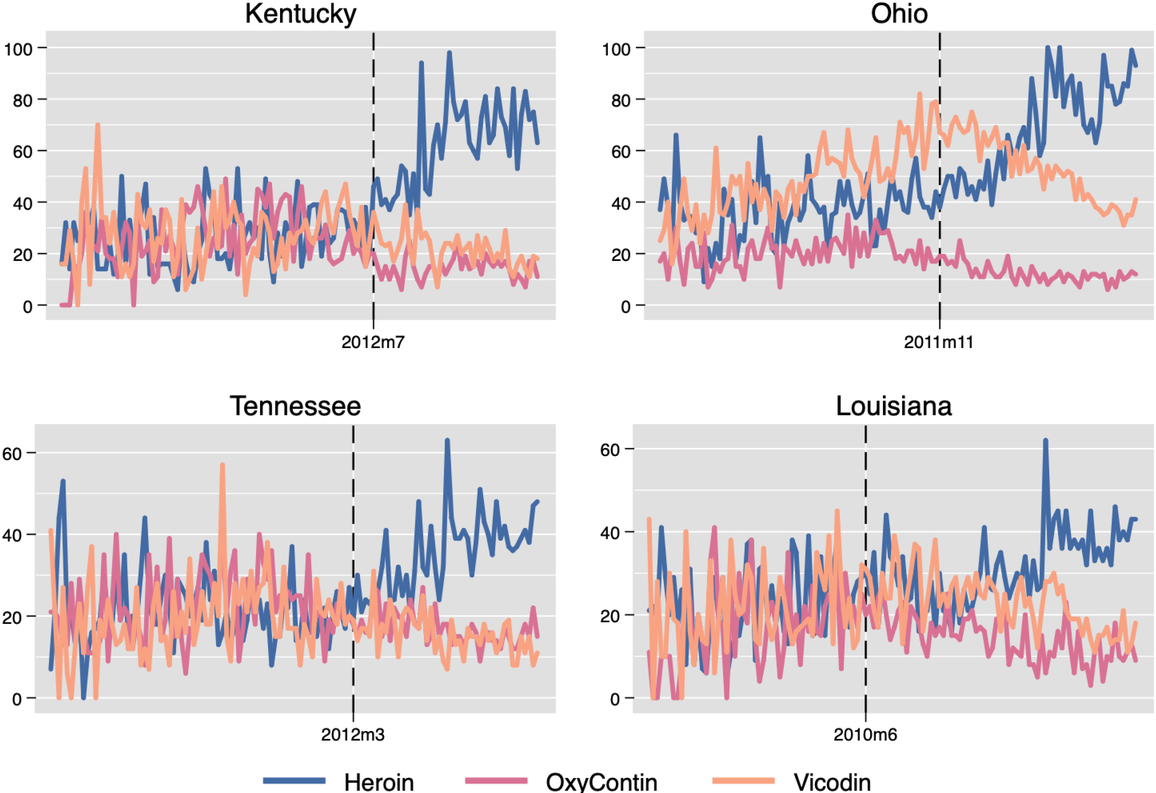
Monthly Google trends index for relevant opioids around the implementation of mandated PDMP use in selected states, 2006–2015. Note: The vertical dashed line indicates the time of mandated PDMP implementation
Robustness checks
We conducted a series of robustness tests that include several model specifications and variable operationalizations. We first test for alternative model specifications, including using the logarithm of absolute deaths as dependent variables, and adding state‐specific time trends to account for unobservable state‐level factors that evolve over time. We then lag the implementation date by 1 year and repeat the analysis, considering the possibility that the newly implemented interventions may be effective with some time lag.
In addition, we account for possible confounding due to other opioid‐related regulations implemented by states around the same time (e.g., pain clinic laws, the reformulation of OxyContin) and exclude outlier states (e.g., North Dakota with a high rate of suppressed data, New Mexico with inconsistency in measuring key outcomes in some periods, Washington with its unique mandate to follow prescribing guidelines, and Florida with its unique legislation to close “pill mills”). We also conduct a falsification check where we randomize the law implementation time; this allows us to confirm that our results were not idiosyncratic.
Finally, it should be noted that synthetic opioids such as fentanyl have become a key contributor to overdose deaths, and many heroin‐related deaths may in fact be due to synthetic opioids mixed with heroin (Mars et al., 2018). These deaths may be coded as death due to “other and unspecified narcotic deaths” (T40.6 in ICD‐10). To test the robustness of this coding issue, we combine unspecified narcotics with heroin deaths. We also repeat the analysis by excluding state‐years that had few heroin deaths. Our main findings are robust to all of the above tests; see Supporting Information Section EC.3 for more details.
CONCLUSION
This study examines the impact of electronic sharing of prescription information on population‐level prescription opioids as well as illicit alternatives. We find that mandating PDMP has the effect of curbing overprescribing of opioids. As such, mandating PDMP use may be an important policy intervention in addressing the opioid epidemic. However, the curbing of opioid prescriptions also has an unintended effect of generating increased spillover demand for heroin. The unintended impact on heroin‐related deaths has not been fully understood, particularly in recent years as more states have rolled out PDMP mandates. Many researchers and policymakers have called for detailed empirical analyses of more data prior to claiming any causal effects of PDMP (Rudman et al., 2017). We employ data from all 50 U.S. states and the District of Columbia during the years 2006–2015 and find that states with mandated PDMP use experienced an unprecedented (50.1%) rise in heroin‐related deaths.
We also find heterogeneous effects of the policy on outcomes. More stringent versions of PDMP mandates in terms of legal enforcement, specificity of use, integration with EHR, and interstate information sharing are effective at further reducing opioid prescriptions. Unfortunately, stronger mandates further exacerbated heroin‐related deaths, suggesting that restricting the prescription opioid supply is not a panacea.
We also show that environmental factors moderate the effect of PDMP mandates: areas with lower levels of pain reliever dependence, lower levels of heroin availability, and higher availability of treatment facilities do not exhibit an increase in heroin deaths, suggesting that the substitution effect is mitigated by the local environmental conditions.
We supplement our analyses with Google keyword search data to corroborate the substitution of prescription opioids for heroin. We find that in postpolicy, there is an increase in Internet keyword searches for heroin, whereas searches for keywords related to prescription opioids decrease.
In summary, our econometric analysis using difference‐in‐differences provides strong evidence that mandating PDMP use, while reducing prescriptions, inadvertently leads to a significant rise in heroin‐related deaths. In addition, we find no evidence that the effect of the policy has attenuated over time; in fact, our event study analysis suggests that the impact on heroin‐related deaths continuously grew during our data period. We also find larger effects of the policy in states that are more stringent in mandating PDMP usage. Also, we identify certain local environmental factors that mitigate substitution for heroin.
It is important to note that our analysis does not suggest that mandating PDMP use should be discontinued. In principle, reducing the supply of prescription opioids should diminish the likelihood of initiation into opioid misuse and eventually shrink the population that transitions from medically intended opioids to heroin—a desired long‐term outcome. However, for the over 2 million individuals who are estimated to already suffer from OUD, PDMP mandates may be harmful. For example, MAT is one intervention that has been shown to be effective in the treatment of OUD, and there are plans by several government entities, including the Food and Drug Administration to expand therapies in this area. 10 However, the current PDMP laws hinder the prescribing of MAT medications; as such, more flexibility in accommodating prescribing of medication specifically for MAT could be considered. Additionally, a recent report points to the shortage of treatment and rehabilitation capacity for treating opioid patients, as evidenced by long lists of patients waiting to be admitted (UMSPH, 2019). Therefore, demand‐side solutions such as the expansion of treatment and rehabilitation capacity are critical to addressing population‐level substance abuse. One particularly useful policy lever to increase access to MAT is Medicaid expansion. Medicaid covers approximately 40% of people with an OUD nationally and can be used to improve the delivery of and reimbursement for MAT (SAMHSA, 2018). For example, Burke and Sullivan (2021) examine Rhode Island's expansion of access to MAT for OUD in conjunction with Medicaid expansion and find a decline in opioid‐related mortality between 2016 and 2018.
Beyond MAT, several potential areas of policy improvement have been identified. Direct‐to‐physician marketing by pharmaceutical companies has been pointed out as one of the drivers of the widespread use of opioids in the first place. Eisenberg et al. (2020) find that academic medical centers' conflict‐of‐interest policies that restrict direct‐to‐physician marketing can substantially curb opioid prescribing. Another possible policy intervention is increased access to naloxone, an opioid antagonist that can save lives when administered during an overdose. In fact, North Carolina and Maryland enacted laws to increase naloxone distribution by community organizations and police officers. However, Doleac and Mukherjee (2021) find that the expansion can lead to more opioid‐related ER visits and opioid‐related theft, with no net measurable reduction in mortality. Other states are reassessing drug laws and enforcement. In November 2020, Oregon voters approved a measure toward decriminalizing possession of small amounts of heroin. 11 Those found with small amounts of heroin may choose between paying a $100 fine or getting a health screening from a recovery hotline. At this point, it is unclear whether decriminalization without treating OUD can be effective at tackling the epidemic. Overall, to help existing opioid dependency sufferers, further expansion of access to treatment facilities will be required in conjunction with considerations in various areas such as direct‐to‐physician marketing, naloxone distribution, and decriminalization.
Our study has several limitations. First, the implementation of the policy varies from state to state, and we assume that the exposure to PDMP mandates is uniform to simplify our study. Although we have considered major key features of the policies, other minor differences across state policies may not have been fully accounted for. 12 Second, although our model fits are strong and comparable to similar studies in the literature, the sample size is limited by the number of states as with other studies that examine state‐level policy impacts. Finally, while the use of PDMP increases substantially after states mandated PDMP, we do not have access to the actual usage of PDMP. Future research may further pursue this question by directly using PDMP registrations and/or queries once such data become available. Overall, our finding that states implementing PDMP mandates experience a substantial increase in death rates postimplementation is of significant policy concern. More research is needed to fully understand the behavioral mechanisms and the consumption choices of individuals in order to more effectively combat the nationwide opioid epidemic.
Footnotes
ACKNOWLEDGMENTS
We would like to thank the editor and three anonymous reviewers for their constructive comments throughout the review process.
1
The most prominent drug used in MAT is buprenorphine. Dosages of buprenorphine are often higher when used to treat OUD. These higher doses translate to a higher calculation of medication dosage in PDMP systems that can restrict dispensing the drug but may, in fact, be appropriate for treating the disorder. See more details at
2
A summary of relevant past research such as the level of analysis, data source, type of policy analyzed can be found in E‐Companion Table A1.
3
CDC WONDER. Centers for Disease Control and Prevention.
4
The National Center for Health Statistics captures cause of deaths for 1999 and beyond from death certificates using the codes included in ICD‐10. Note that ICD‐10, first published in 1994, is a medical classification listed by the World Health Organization and differs from U.S. variations such as ICD‐10‐CM and ICD‐10‐PCS.
5
Google Trends. Google.
6
However, PDMP mandates were not associated with any significant change in prescription opioid overdose death rates. This implies that the policy led to an appreciable reduction in opioid prescription but did not reduce deaths in the short term.
7
This time period was chosen to be consistent with the data we used to measure the heroin availability, which will be discussed later.
8
The data were provided by the 4‐year Restricted‐use Data Analysis System (
9
Note that the Google trends analysis by itself suggests one of two possibilities: (1) restrictions in the supply of prescription opioids led users to seek out substitutes in the open marketplace or (2) the resulting increase in heroin deaths led to an increase in public interest in the phenomenon. However, given the additional finding that consumption of illicit street drugs increased following the PDMP mandates (Deiana & Giua, ![]() ), the first mechanism seems more plausible. Future research is needed to further pinpoint the causal pathway.
), the first mechanism seems more plausible. Future research is needed to further pinpoint the causal pathway.
10
See more details in the FDA guidance document “Opioid Use Disorder: Endpoints for Demonstrating Effectiveness of Drugs for Treatment Guidance for Industry.” Available at
11
See more details in the NPR Special Series “Oregon's Pioneering Drug Decriminalization Experiment Is Now Facing The Hard Test.” Available at