
Abstract
In 2020, the world started a fight against a pandemic that has severely disrupted commercial and humanitarian supply chains. Humanitarian organizations (HOs), like the World Food Programme (WFP), adjusted their programs in order to manage this pandemic. One such program is cash and voucher assistance (CVA), which is used to bolster beneficiaries' freedom of choice regarding their consumption. In this vein, WFP supports local retailers to provide CVA to beneficiaries who do not have access to a functioning market. However, the operations of these stores can suffer from a very high transmission risk of COVID‐19 unless preventive measures are put in place to reduce it. This paper discusses strategies that retailers and HOs can enact to maximize their service and dignity levels while minimizing transmission risk under a CVA program during a pandemic. We argue that HOs providing CVA programs can improve their assistance during a pandemic by implementing strategies that impact the retailing operations of their retailers.
Keywords
INTRODUCTION
In March 2020, the World Health Organization (WHO) declared COVID‐19 a pandemic and in doing so changed the world. Literally within days, the entire world began to grapple with a pandemic that would severely affect the operations of almost every commercial company and humanitarian organization (HO), including their supply chains. While there have been several recent disease outbreaks (e.g., the Ebola outbreak between 2014 and 2016 in West Africa), COVID‐19 was the first to become a full‐blown pandemic. Largely due to its ease of transmission and the fact that COVID‐19 can be spread before a person has any symptoms, it achieved global propagation. In order to contain the pandemic, governments quickly responded with massive mobility restrictions, up to complete lockdowns and tighter measures for cross‐border transits, which dramatically affected all supply chains and economies worldwide.
The specific challenges of pandemics (as shown by COVID‐19) demand that HOs rethink their strategies in order to keep their programs running effectively, which is in the best interest of all stakeholders. Traditionally, HOs have provided in‐kind aid to help beneficiaries satisfy their direct needs. In the past decade, though, HOs and donors have increasingly realized the importance of strengthening local economies and helping beneficiaries retain part of their dignity by letting them choose what to consume (Besiou & Van Wassenhove, 2015). A functioning market can help to achieve these goals. HOs use market‐based interventions (MBI) to assess markets' capacities. One example of this approach is cash and voucher assistance (CVA). HOs' aim is to also run CVA programs during pandemics (in particular, as voucher programs), but research so far has neither looked at how these programs have to be adjusted in the wake of pandemics, nor how these adjustments shape the impact of the pandemic. In CVA programs, HOs typically develop agreements with local retailers to serve beneficiaries with the items that they can procure using their entitlements. While providing a CVA program has many advantages, it is limited by its applicability: namely, areas where a functioning market exists. So the retailers' role in the success of CVA programs is critical. To solve this challenge, the World Food Programme (WFP), one of the leading humanitarian organizations, has gone one step further by introducing a new MBI model called retail‐in‐a‐box (RIB).
RIB introduces fast CVA assistance to areas with no functioning market by either developing or rebuilding damaged retail facilities. It helps retailers identify the most efficient and effective ways for opening and running their stores. WFP supports them in structuring and designing their store's layout (tactical planning) or planning their replenishment and prices (operational planning). For example, whether the store adopts a self‐service (walking freely in the store) or an over‐the‐counter (ordering and picking up from a counter) layout can affect the retailer's service level. To achieve a further improvement in service levels and to diminish price inflation, WFP seeks to collaborate with various competing retailers. Since this is a widely understudied area, Starr and Van Wassenhove (2014) called for more research that looks at innovative business models that support the local economy, and RIB is an excellent example.
CVA programs often take place in crowded or low‐hygiene locations (like refugee camps or disaster‐stricken areas) where the virus can spread rapidly (Truelove et al., 2020; Weill et al., 2020). WFP, for example, initiated three successful RIB innovations during the pandemic: (i) in Cox's Bazar (Bangladesh), one of the world largest refugee camps at that time; (ii) in Masquil Alto (Mozambique), a rural area where beneficiaries had to travel a long way to buy their daily needs; and (iii) in South Sudan where COVID‐related border closures as well as travel and transport restrictions severely affected food supply chains (WFP, 2020b). All three projects had to be set up quickly to ensure resilient food supply chains while guaranteeing safety and hygiene regulations, as the pandemic significantly increased the number of beneficiaries.
WFP's experience in these projects showed that HOs that operate in such environments need to adjust their strategies to the new pandemic reality by considering different objectives. Besides satisfying the daily needs of the beneficiaries, HOs need to consider the virus transmission risk and impose strict preventive measures (e.g., physical distancing) to protect both beneficiaries and staff members. However, to the best of our knowledge, there is no research looking at the interaction of preventive measures imposed during a pandemic and their consequences on retailing operations of CVA programs. Thus, the paper focuses on identifying strategy and policy changes that HOs could adopt in the face of pandemics in order to achieve humanitarian objectives while reducing transmission risk. To that end, this paper analyzes the management and operations of retailers operating CVA programs during the COVID‐19 pandemic.
Our objective in this paper is threefold: First, we present the unique case of WFP's RIB initiative. We conduct a study by interviewing WFP's staff from both management and field teams to better understand the specific context and challenges of the RIB. We particularly look at how RIB's strategies have been adjusted in the pandemic and how they impacted retailers' operations. We show that retailers working with HOs under CVA programs are different from typical commercial sectors in aspects like (i) having HOs as governing partners regulating the number of competing retailers in the market and monitoring the prices, setting rules like pandemic preventive measures (e.g., requiring physical distancing, mask wearing, and hygiene rules), and requiring a minimum list of products that should be available in the stores; (ii) having a more predictable demand, as the number of beneficiaries in certain areas is typically known; and (iii) HOs giving retailers guidance on store layout designs and operations. However, there is insufficient understanding of these retailers' operations not only during pandemic response but also under normal conditions.
Second, the findings from the case study led us to investigate the impact of pandemics on two critical economic features of CVA programs with competing retailers on the (i) equilibrium assortment size offered to beneficiaries and (ii) equilibrium price. Capturing the retailers' operational decisions, we modeled a two‐retailer assortment and price competition game inspired by the Bertrand competition game. We derived two main analytical findings. First, we show that during a pandemic like COVID‐19, providing beneficiaries with appointments—which was a preventive action taken by WFP to manage the pandemic—increases the competition between retailers, leading to larger assortments. Second, in the price competition under the COVID case, retailers are more cautious about increasing their prices compared to the pre‐COVID case, and try to keep the prices as competitive as possible. So we show that giving an appointment to beneficiaries as a preventive action during a pandemic can indirectly improve the assortment and price for beneficiaries. Our findings can help WFP better implement their CVA programs by understanding how competing retailers would adjust their assortments and prices in a pandemic.
Third, we looked at retailers' tactical decisions by comparing self‐service (SFS) and over‐the‐counter (OTC) layouts in terms of their service level (i.e., the number of served beneficiaries in a specific time frame) and transmission risk under different preventive measures taken to manage the COVID‐19 pandemic. By coupling a queuing model with a discrete event simulation, we arrived at three main findings: (i) contradicting the common belief that the SFS layout increases the service level, we show that managing pandemics by increasing the social distancing significantly impairs the performance of the SFS layout, but has little effect on the OTC layout; (ii) while the SFS layout might provide lower transmission risk under the “no social distancing” scenario, the OTC layout is better under higher social distancing scenarios; and (iii) we show that providing beneficiaries with appointments as a preventive action has a larger effect on controlling the transmission risk than common social distancing measures. We argue that when the beneficiaries constitute a large population and are culturally accustomed to the SFS layout, then the SFS layout with an appointment is the best choice. It serves more people in a shorter time, provides a higher dignity level, and more importantly, it is relatively safe in terms of transmission risk. We validated our model through WFP's RIB case in Mozambique.
The structure of the paper is as follows: Section 2 presents a literature review looking at MBI and CVA humanitarian operations and disease spreading. In Section 3, we discuss the RIB case study. Sections 4 and 5 discuss the retail competition and operations models, respectively. Section 6 presents the discussion, contributions, and future research. Section 7 concludes this paper.
LITERATURE
Market‐based interventions and cash and voucher assistance programs
In‐kind aid consists mainly of foodstuffs, medicine, shelter, household goods, and tools. The focus of humanitarian aid on in‐kind aid stems largely from a long‐standing tradition of governments and HOs deciding what meets the best interests of the populations receiving the aid. However, the humanitarian response should help local communities achieve a faster and more sustainable economic recovery. MBI does that by supporting or developing local markets, which can be achieved by either in‐kind aid through local procurement or through CVA. In general, humanitarian aid has recently shifted from in‐kind aid systems to MBI, which mainly focuses on infusing cash into in‐need communities (Heaslip et al., 2018; Sahinyazan et al., 2021). Notably, CVA has been used in governmental responses to the COVID‐19 pandemic (Jerving, 2020).
Daar et al. (2018) identified “strengthening economies” as one of the top 10 humanitarian challenges and suggested restoring markets by scaling up CVA. Lewin et al. (2018) highlighted CVA as an important program for strengthening local economies. Published reports heavily emphasize the strengths of CVA programs (UNHCR, 2012), which can play a major role in assisting people during or after emergencies. Vouchers represent a form of cash distribution in which a paper or electronic voucher may be exchanged for a predetermined value of goods with preselected vendors. Nowadays, voucher programs are growing quickly due to being implemented in both short‐term (postdisaster relief) and long‐term (development programs) aids. For example, in 2020, voucher programs accounted for over one third of WFP's assistance (WFP, 2020c). CVA programs represent a fascinating state‐of‐the‐art business model with strengths and weaknesses (Besiou & Van Wassenhove, 2015). However, even as the ratio of CVA programs over in‐kind aid increases, research continues to focus mainly on in‐kind aid (Besiou & Van Wassenhove, 2020).
So far, most of the papers on CVA have explored their strengths and weaknesses, along with their impact on logistics (Bailey & Harvey, 2015; Heaslip et al., 2018). There is growing evidence that voucher distribution impacts HOs and their beneficiaries (Bailey & Harvey, 2015). For example, voucher programs not only reduce transportation costs needed to effectively distribute in‐kind aid but also support local retailers, facilitate competition, and strengthen local economies. Moreover, CVA helps individuals reclaim some of their dignity by letting them choose what to buy. However, while research acknowledges that retailers are necessary for implementing CVA, the literature has largely ignored how the process works—especially in the challenging context of pandemics—and instead focused on the impracticality of implementing CVA in weak markets.
CVA programs frequently arise following natural disasters, in cases of conflict (like in refugee camps where there were concerns of misusage and fraud; Voge et al., 2021), or when such programs can reduce gender‐based violence (Slim et al., 2020). Implementing a voucher exchange may take up to 6 weeks to properly organize (Creti, 2006) due to needing to reach agreements with local suppliers on processes, quality, and availability. At the same time, humanitarian organizations that operate CVA programs, like the International Committee of Red Cross (Slim et al., 2020), face the challenges of weak or nonfunctional local market systems, alongside highly volatile prices. These challenges worsen during a pandemic, since the demand may reduce due to consumers' fear of being in crowded places and the retailers' need to implement safety measures that may affect service.
The success of CVA depends on several factors: the willingness of donors to provide funding, the willingness of HOs to run these programs, and the capacity of local retailers to maximize profit while adhering to the HOs' dignity and service‐level objectives. As the largest HO operating CVA, WFP has realized that local retailers in developing countries may not have the proper infrastructure or knowledge to respond to the increase in need following a disaster. This realization gave rise to the MBI of RIB initiative, which seeks to bolster the strength of local retailers to the point that their operations do not need WFP's support. However, the COVID‐19 pandemic has complicated these efforts; RIB needed to adjust to the new reality of managing the pandemic. In this paper, we respond to Starr and Van Wassenhove (2014) and Voge et al. (2021), who have called for research on innovative business models that build upon local strengths by considering ways to improve local retailers' operations within CVA programs, especially during a pandemic. The authors also noted that research should include the beneficiaries' experience, which we incorporate here by looking at beneficiaries' dignity and empowerment. By setting up agreements with retailers, RIB can serve as a solution to the challenges that Slim et al. (2020) articulated. One of our objectives is also to better understand how retailers compete on price and assortment, which are two critical operational challenges of CVA programs according to Ferrão et al. (2020).
Disease spreading literature
The scientific literature has published many articles on COVID‐19 since the virus began spreading at the end of 2019. Here, we will mainly focus on studies that relate to the transmission and infection risks of COVID‐19, which are important to our assumptions and modeling. For an overview of the literature on the air‐based transmission of SARS‐CoV‐2, we refer to Delikhoon et al. (2021).
In a scientific brief in July 2020, the WHO (2020) provided an overview of the modes of transmission of SARS‐CoV‐2, emphasizing how and when the virus is likely to spread. Major attention was given to respiratory transmissions by airborne mechanisms (e.g., from droplets and aerosols). Indeed, it appears that individuals can become infected simply by inhaling a sufficient amount of other people's droplets that contain the virus (WHO, 2020). In response, various studies have investigated factors that influence the risk of airborne transmission (e.g., Alsved et al., 2020; Luo et al., 2020).
Scholars have applied different methodologies to estimate the risk of virus transmission and the effects of various interventions. Beyond original clinical trials and experimental research, one can find meta‐analyses that aggregate information. In an early study sponsored by the WHO, Chu et al. (2020) found that the risk of person‐to‐person transmission of SARS‐CoV‐2 can be reduced by 80% through measures such as face masks and physical distancing of at least 1 m. The authors used a systematic literature review and meta‐analysis to investigate the optimum distance for avoiding person‐to‐person virus transmission. However, their research involved a limited number of studies and included other virus types such as SARS and MERS. Later studies recommended a larger physical distance of 1.5 or even 2 m because of the high risk of aerosol transmission (CDC, 2020; Jones et al., 2020). Similarly, Weill et al. (2020) discussed how the risk of transmission is much higher in places that are crowded and/or feature low hygiene.
One useful model that scholars have utilized to predict airborne transmission risk is the Wells–Riley equation (Riley et al., 1978). This simple evaluation function predicts the risk of an airborne infection based on the concept of “quantum of infection”: a hypothetical infectious dose proposed by Wells (1955). The quantum characterizes the number of infectious airborne pathogens randomly distributed throughout the air of a confined space (following a Poisson distribution) required to infect a person. The Wells–Riley equation calculates the infection's probability by considering the number of susceptible people in the confined space, the number of infectious people, the room ventilation rate with clean air, and the exposure time (Sze To & Chao, 2010). A number of studies use the Wells–Riley model to simulate driving factors and the effects of intervention strategies; for example, the quantum rates' impact (Buonanno et al., 2020) or the role of air ventilation (Bhagat et al., 2020). Moreover, scholars have published various modifications and extensions of the Wells–Riley equation. Fennelly and Nardell (1998) added a variable for respirator leakage to evaluate the relative efficacy of personal respiratory protection. Meanwhile, Qian et al. (2009) extended the model by considering the spatial distribution of infection risk (since the original Wells–Riley model is restricted to uniform distribution). Sun and Zhai (2020) introduced a distance and ventilation index to investigate the impact of physical distancing and ventilation effectiveness.
In this paper, we use the modified Wells–Riley model developed by Sun and Zhai (2020) as an index of transmission risk. To the best of our knowledge, this model has not been used before in an operations management setting to integrate health concerns such as a pandemic.
RIB CASE STUDY
In this section, we present the RIB case study. Specifically, Subsection 3.1 describes the context of RIB, Subsection 3.2 illustrates the impact of COVID‐19 on the humanitarian retail operations of RIB, and Subsections 3.3– 3.6, respectively, discuss the differences between RIB and commercial retailing, RIB's objectives, its advantages and disadvantages, and how competition works.
General context
WFP is the world's largest HO that provides food assistance to people recovering from a conflict or natural disaster. From the late 2000s, WFP's strategy has shifted from just getting food to people in need to addressing people's long‐term nutritional needs, known as food assistance (WFP, 2021b). Furthermore, since food assistance is a crucial element of general societal well‐being, WFP continuously tries to give beneficiaries a voice and, if possible, a choice on what food to receive and how to receive it. That is why, over the past decade, WFP has replaced in‐kind with CVA whenever possible. For example, 37% of WFP's total assistance to beneficiaries in 2020 was provided through CVA, reaching a record high of 2.1 billion US dollars (WFP, 2021a); for comparison, that number was 846 million US dollars back in 2014 (WFP, 2015).
Since RIB is a recently developed MBI initiative, we conducted field research to understand its specific characteristics and differences with other assistance programs. Our data consist of eight interviews and internal reports, as well as documentation from the RIB team. The interviewees were drawn from both management and field teams in order to gather different, valuable perspectives about RIB's type of assistance. We asked open questions to avoid bias in our data and collected detailed information. The online supporting information details the location and positions of all interviewees, as well as contains the questionnaire. Collected data from the interviews provided a clear picture of WFP's assistance process. Whenever WFP identifies a new group of beneficiaries, the program office conducts an extensive study to understand the needs, situation, existing market infrastructure, and so on: Where do you buy your food? Do you have access to your regular retailers? How much do you pay for your food? What type of assistance would you rather, e.g., get rice, or would you rather receive the cash? (Interviewee 4, Quote 1)
RIB was one of the five winners of the 2019 WFP Innovation Awards (WFP, 2020a). The RIB concept can be a quick MBI solution when either no retail market is available within a 5‐km radius, like in many places in Africa, or the retail sector is severely damaged after a disaster. The initial idea of RIB was inspired by typical pop‐up stores in the commercial sector, which are an effort to get closer to their final customers. In RIB, the role is to enable the program officer to say cash and voucher is an option, even though markets are not fully functioning […]. The rule is to enable a better type of assistance just because we know that cash over in‐kind has other multiplier effects that provide assortment and choice and dignity to those affected populations. (Interviewee 4, Quote 2)
Therefore, RIB operations start by selecting a few potential retailers who meet the minimum criteria of capacity and cost through a competitive and transparent procurement process and are suitable for the program. RIB pursues multiple retailers to facilitate competition and thereby improve the service offered to the beneficiaries and diminish price inflation. Depending on the retailers' context and capabilities, RIB decides to either provide the retailers with a store infrastructure (like in Cox's Bazar and South Sudan) or support them in building their own stores (like in Mozambique). Moreover, RIB trains retailers to cobuild this initiative rather than just having a pure business relationship in order to further incentivize them to invest in retailing in this location. For example, the program helps retailers with both their tactical (store's layout design) and operational (inventory management) decisions and also train them on how to treat the beneficiaries. Note that WFP earmarks its assistance to ensure that retailers generate enough income, on the one hand, and beneficiaries receive their assistance with the highest standards possible, on the other hand. We come with the whole calculation to see what are their input costs, how long can we secure the assistance, how much is the cost to set up the shop, […] we tell them when is the next distribution, the approximate number of beneficiaries so they can prepare. It's also on this whole retail training curriculum, food safety and quality, replenishment and ordering, and how to organize their shop. (Interviewee 3, Quote 3)
COVID‐19 effects
Like other humanitarian programs, the RIB initiative has been tremendously affected by COVID‐19 and needed to adjust to the new conditions 1 to minimize the transmission risk and avoid harming the beneficiaries through their programs. To this end, stores had to adopt hygiene rules like (i) having employees and beneficiaries wear masks and gloves, (ii) practicing hand hygiene, (iii) getting screened for increased temperatures using contactless thermometers before entering stores (CaLP, 2020), and (iv) regulating physical distancing (e.g., 1 m vs. 1.5 m vs. 2 m depending on the regulations of the country). 2 Moreover, since the transmission risk depends on the distance and the duration of contact time (Jones et al., 2020), it is crucial to reduce the duration of time that beneficiaries spend waiting in line. To minimize the waiting time during COVID‐19, RIB decided to assign appointments to the beneficiaries (via SMS) so they could perform their monthly shopping on an exact date and time. Furthermore, only one family member was allowed to shop only once per month and was supported with transporting the purchases back to their homes. In some cases, to speed up the shopping process even more, retailers were asked to minimize the amount of product variety. WFP also tried to fully replace cash and paper vouchers with e‐card vouchers to avoid contact. In comparison to in‐kind assistance, the use of CVA through appointments generally mitigates the need for gathering and crowds at distribution sites and can help reduce transmission risk.
Structural specifications compared to commercial retailing
Although RIB might seem to parallel the grocery retailing sector in terms of selling food to customers, WFP's involvement shifts some of the initiative's operations and goals. In terms of operations, the RIB's retailers differ from the typical commercial sector concerning:
Governing power of WFP: WFP has a governing power over both beneficiaries and retailers. Concerning retailers, WFP controls the number of retailers operating on the market and their pricing policy to avoid excessive inflation. The price increase is limited to 5–10%. However, there have been observed cases of retailers increasing their prices by more for a while in order to achieve short‐term gains; when WFP realize that, the retailers receive a warning and reduce their prices. In addition, WFP collects feedback from the beneficiaries about how they are treated and responds if necessary. Moreover, WFP requires the retailers to provide a minimum list of available products. This list is developed from the feedback that beneficiaries provide to WFP regarding their preferences. Of course, these retailers can provide more products and brands. Looking at the beneficiaries, WFP initiated an appointment system to control the crowd in the store and reduce transmission risk during the pandemic. Moreover, both paper (quantity or bundle) and e‐card vouchers are earmarked to those retailers and can be redeemed for any product inside the store except for cigarettes and alcoholic drinks. Earmarking the vouchers to a few retailers provides the RIB with a higher monitoring power and the ability to discontinue the contract at any time with a retailer who does not follow the RIB's objectives.
Demand planning: Since RIB explicitly targets a specific number of beneficiaries based on country‐specific voucher amounts, the retailers' demand within RIB settings is typically quite predictable and not as uncertain as in the commercial sector. WFP has control over how and when to distribute the vouchers, which means having more opportunities over controlling the demand.
The store's layout: Because the stores are always either built from scratch or repaired, there is an opportunity (as a tactical decision) to structure the retail store around any specific condition. The most common layout designs are SFS (where beneficiaries can freely walk around, check products, and prices) and OTC (where beneficiaries are individually served by an employee). The preference over the layout depends on what customers are used to and which layout provides the optimal balance between service‐level fulfillment and safety (COVID‐19‐related restriction).
Objectives
WFP aims to fulfill different objectives through RIB:
Social and economic impact: for RIB and its donors, it is essential to not only save beneficiaries from hunger but also give them the opportunity to live better: Distributing a dollar has a multiplier effect on the economy and teaching retailers is providing jobs; that has an accelerating impact on local economies. (Interviewee 5, Quote 4) At the same time, they (retailers) also may empower the local community more. More people are hired from the host, the population of the refugees, etc. (Interviewee 1, Quote 5)
Dignity: RIB tries to achieve dignity by coupling beneficiary services with different measures: (i) retailers need to treat beneficiaries in the same way they treat other customers, for example, WFP staff can also procure from these stores; (ii) depending on the local culture, the layout design (SFS or OTC) may increase the dignity; and (iii) beneficiaries must have the power to choose among different brands of products, sizes, when and with whom to go, and for how long to stay, etc. The dignity comes with the fact that the beneficiaries can choose many more different sizes […], by giving them choices of how much to buy and what to buy. (Interviewee 3, Quote 6)
Service level: RIB aims to have a high service level rate by serving as many beneficiaries as possible in the shortest time. Furthermore, it is crucial not to keep beneficiaries waiting for long: If we have people waiting or crowding in front of the shop for the whole day in the sun, that's something that's very much against what do we want to achieve. (Interviewee 3, Quote 7)
Transmission risk of COVID‐19: RIB tries to reduce transmission risk by implementing the measures discussed in Subsection 3.2.
Advantages and disadvantages
Looking at the RIB from a broader perspective, there are advantages and disadvantages for its four stakeholders:
Beneficiaries: RIB brings various advantages to beneficiaries. First, beneficiaries get the opportunity to benefit from CVA in places that suffer from a lack of retailers. This empowers them with having more choices and higher dignity levels. Second, RIB increases social protection. Almost 60% of the beneficiaries who do the shopping are women. Since they do not need to travel long distances in isolated areas anymore, they feel significantly safer and save time for other tasks. The RIB is also used frequently by elderly people, who are more empowered thanks to the shorter traveling distance. Last but not least, RIB creates new markets in some cases, thereby enabling beneficiaries to produce some products and sell them at a newly created market next to the RIB stores.
Retailers: RIB provides a great opportunity by creating demand for these primarily small retailers to grow their business. They get support on their feasibility studies and operational decisions, and in some cases, receive the necessary infrastructure. The disadvantage is that these stores might end up being idle when the assistance stops. However, depending on the case, retailers may be able to continue their operation, if the assistance helps to grow the local economy: In Mozambique, not only those retailers are still operating, but they have also built new stores even though WFP's assistance ended a while ago. (Interviewee 3, Quote 8)
Donors: The advantage for donors is that RIB provides the opportunity of delivering CVA where it was not possible before. This has a high value for donors because it empowers beneficiaries to choose what they would like to have and supports localization and the local economy.
WFP: WFP is also in favor of RIB as an MBI and that provides more CVA because (i) CVA has a positive impact on the local economy and (ii) it is donors' preferred assistance so it can lead to higher fundraising. As a result, the main advantage of RIB for WFP is giving more power to beneficiaries. The primary disadvantage might be having more workload that requires more staff to push the projects.
So far, RIB is in a pilot stage, but WFP has already decided to use this initiative in a few more places. The organization expects that the RIB will mainly expand in remote areas where the local markets are not fully functioning, as one of our interviewees highlighted: If cash is growing in non‐urban areas, RIB grows. (Interviewee 5, Quote 9)
Competition
We mentioned in Subsection 3.1 that RIB enables a few retailers to start operations in the area. WFP chooses multiple retailers to enhance competition among them regarding product assortment, prices, and services. In doing so, beneficiaries receive greater choice power and quality of service: In Mozambique, we don't need to have three shops. We can have only one. But just to make sure that there is competition, and it is not only about price, it is also about service. (Interviewee 7, Quote 10)
The competition among retailers working with RIB might differ from commercial retailers' typical competition. First, the retailers are highly affected by strategies and policies undertaken by HOs. Second, HOs define the maximum allowed prices to avoid inflation. That is, retailers are allowed to change prices in a certain range. Third, RIB requires retailers to provide a minimum amount of specific products, but they are free to increase their assortment in length (number of different items) and depth (different brands of the same item) to compete with each other. Note that growing the assortment in either length or depth is considered desirable for beneficiaries since it increases their power of choice. Ultimately, beneficiaries' decision to patron a given store depends on the quality of the assortment (the larger, the better), the prices (the lower, the better), and the waiting time (the shorter, the better). In the Mango season, there are so many varieties of Mangoes available, and we have a few retailers who are actually procuring far above the standard that we set […] they want to encourage more beneficiaries into their shops than the competition right next to them. When this happens, then the other retailer take a few money off […] and it's extremely empowering when you see the refugees, sometimes going back and forth and checking the menu, checking the price or checking the different quantities available. (Interviewee 1, Quote 11)
Since there is a limited number of retailers in the area, it is possible that these retailers will collude to jointly raise prices. However, WFP strictly punishes this behavior by either terminating the contract with those retailers or, in severe cases, contracting big suppliers to subcontract all retailers in that area. In the next section, we develop a model to capture the retailers' competition.
RETAIL COMPETITION MODEL
This section studies the assortment (specifically assortment depth) and price competitions among retailers working with RIB both under pre‐COVID (normal) and COVID (pandemic) conditions.
Pre‐COVID condition
Under the pre‐COVID (normal) condition, RIB seeks to increase the power of choice and allow beneficiaries to visit shops whenever it suits them. Since beneficiaries usually wish to shop when they get the vouchers and are allowed to visit the shops as often as they want, stores can get highly crowded. In practice, this means that long queues form in front of retail shops.
Therefore, while retailers are competing to gain higher market share by optimizing their price and assortment size, stores will be getting more crowded and beneficiaries will wait longer to get served. We consider this waiting time to have a counter effect on the beneficiaries' choice of retailer. Thus, it is interesting to assess how the retailers' assortment and price decisions will change based on how waiting time impacts beneficiaries' decisions. Next, we model both assortment and price competitions in the pre‐COVID case while incorporating the waiting time.
Assortment competition
To better understand the impact of competition on the retailers' assortment decisions, we analytically model a competition game similar to an oligopoly
3
game known as the Bertrand competition game (Romp, 1997). We specifically consider two retailers (


We model the assortment competition under the pre‐COVID case while assuming that all different brands have the same price,












We assume having more demand,







Both retailers seek to maximize their profit. Given retailer







By first deriving the best‐response functions The equilibrium assortment










The propositions' proof can be found in the online supporting information. Proposition 1 shows that, in the pre‐COVID condition, having a higher retail price, or having beneficiaries who highly appreciate the large assortment size, leads retailers to increase their equilibrium assortment sizes. Having a product with higher marginal capital cost, or having beneficiaries who are very sensitive to waiting time, reduces retailers' willingness to invest in larger assortments in their stores. Moreover, when retailers' substitutability is very high, retailers know that increasing the assortment has a lower impact on their profit because higher crowding causes a loss in market share. Therefore, they exhibit a diminished tendency to increase the assortment.
Price competition
In the price competition, we follow a similar modeling approach as in the assortment competition. We now consider that the two retailers, A and B, optimize their prices ( The equilibrium price
















We omit the roof of Proposition 2 as one can see it easily from (9). Proposition 2 shows that while the equilibrium price












COVID condition
The RIB initiative was first launched around the time COVID‐19 became a pandemic. Soon after, the program had to adjust all preliminary plans to this new situation as discussed in Section 3. Although some of these preventive changes reduced the beneficiaries' dignity by taking away their freedom of choice (e.g., regarding when and how often to visit the store), they significantly decrease their contact time and thereby promote their safety. Initially, WFP and the retailers were concerned that these changes would significantly deteriorate the beneficiaries' shopping experience. However, they actually received very positive feedback following the implementation. In Mozambique, the feedback that some of the beneficiaries gave is that shops were not crowded. They could walk around and observe the products rather than being in close contact. This was a benefit that they've seen. (Interviewee 6, Quote 12)
One of the primary preventive measures taken by WFP was to give shopping appointments to beneficiaries. This effectively eliminates beneficiaries' waiting time, rendering the retail's assortment and price the critical elements in beneficiaries' patronage decision. To capture the effect of such preventive measure, we developed modified assortment and price competition models.
Assortment competition
In the pre‐COVID case, the retailer i's demand


Both retailers optimize their assortments by anticipating that a larger assortment positively affects demand while implying higher operational costs. Retailer






Note that the participation condition in the COVID case is The equilibrium assortment






Proposition 3 shows that the smaller the marginal capital cost with respect to assortment size, the larger the desirability coefficient of having a larger assortment, the larger the substitutability of retailers, and the larger the price, the more the retailer is willing to have a larger assortment.
One interesting difference in the equilibrium assortment under COVID and pre‐COVID comes with the substitutability of retailers (see Proposition 1). Under pre‐COVID, when retailers' substitutability is high, retailers exhibit a diminished tendency to increase their assortment; this is not the case under COVID. Under the COVID case, when substitutability is high, the competition gets higher and retailers increase their assortment. This only happens due to giving appointments to beneficiaries and eliminating the counter‐effect of the waiting time. The equilibrium assortment in the COVID case is larger than the equilibrium assortment in the pre‐COVID case, that is,

We omit a proof to this proposition, as it easily follows from algebraically comparing (5) and (11). Proposition 4 is somewhat counterintuitive, since one would assume that in the pre‐COVID case, retailers would offer a higher assortment to gain a larger market share. The intuition behind Proposition 4 is that under pre‐COVID, retailers know that a larger assortment size attracts more beneficiaries and this is counteracted by a higher waiting time, which dampens the increase in market share. In the COVID case, the waiting time effect disappears so that the assortment effect dominates and retailers have a higher tendency to increase their assortments.
Price competition
We use the same modeling approach as the price competition under the pre‐COVID condition, while under COVID conditions, the waiting time effect on the demand can be excluded. Hence, the demand function is modeled as

The profit function equation is identical to the pre‐COVID case price competition (8); therefore, the best‐response function is The equilibrium price









The proof is omitted since it can be easily seen from (13). Proposition 5 illustrates that under the COVID condition, the changes in the equilibrium price with respect to The magnitude of effect from changing the assortments (




We omit a proof to this proposition as it easily follows from algebraically comparing the coefficients of








RETAIL OPERATIONS MODEL
While the previous section focuses on how WFP's preventive measures and strategies affect the retailers' competition and their corresponding operational decisions (pricing and assortment), this section analyzes the tactical decisions of retailers under a pandemic. In this section, we focus on tactical retail operational decisions and compare the possible layouts in terms of their service level (i.e., the number of served beneficiaries in a specific time frame) and transmission risk under different preventive measures taken to manage the COVID‐19 pandemic.
The retailing operations in the RIB market involve three stages: (1) the check‐in process, (2) the actual shopping process, and (3) the check‐out process, which can be formulated as a capacitated three‐stage tandem queuing system with blocking and a common waiting room on the first and second stages. Figure 1 illustrates the abstract queuing system.
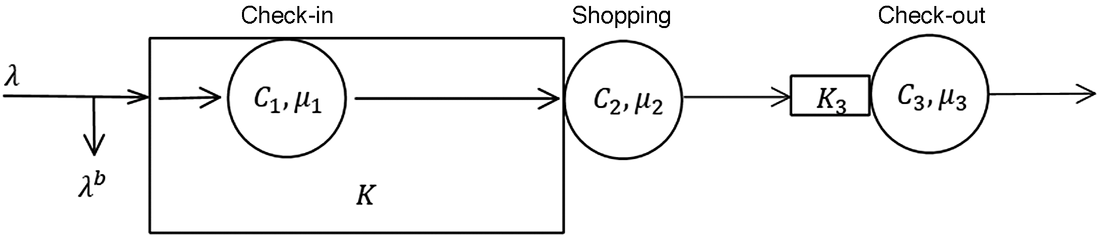
Stylized three‐stage queuing model with a common waiting room for the first and second stages
Beneficiaries arrive at the entrance of the retail store according to a Poisson process with an arrival rate

















Next, we introduce two different possible layout designs and their corresponding mathematical models. Then we introduce a formula for analyzing the transmission risk and finally evaluate layout design and transmission risk based on real data from our case in Mozambique.
Layout designs
Since the RIB is very flexible in designing the store with either SFS or OTC layouts, WFP's goal is to design the stores in the best way possible while considering beneficiaries' past experiences: If the culture is familiar with self‐service, then they consider this as a common culture, and going to self‐service might provide more and more dignity, while over the counter might be more effective for WFP because it is faster. (Interviewee 4, Quote 13)
Therefore, if the culture is familiar with the SFS layout, WFP needs to decide whether they want to implement an SFS or OTC layout. While the perceived dignity level is higher in SFS than OTC, the actual shopping time is typically longer in SFS systems since beneficiaries have to inspect the products on their own, compare prices, and consider their limited voucher budget.
We compare two general layout designs: OTC and SFS. In the OTC layout, the beneficiaries enter the retail store and get served at one of the

Therefore, the SFS layout needs fewer employees in this stage compared to OTC. The capacity in the SFS layout can be interpreted as the number of beneficiaries allowed to be in the store at the same time. Figure 2 illustrates these two retail layouts.
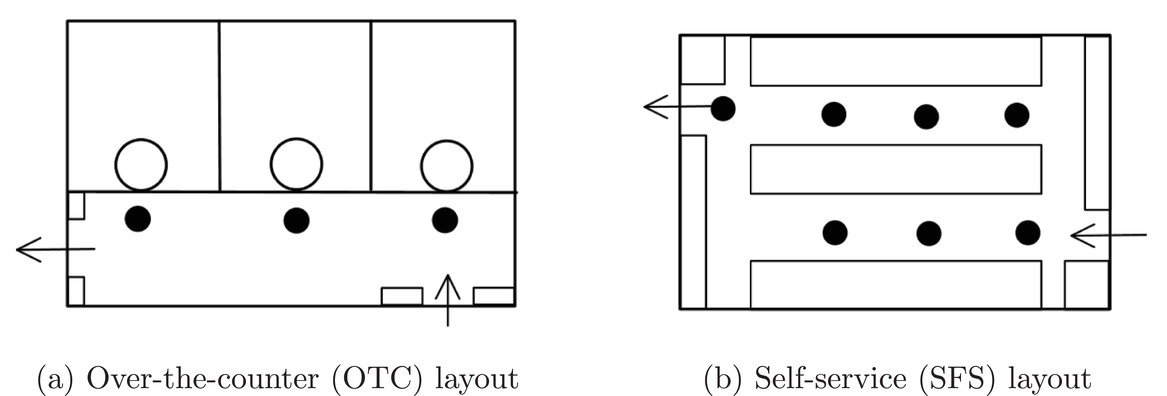
Layout designs of the second‐stage (shopping) process under stylized
The waiting room capacities for both the joint waiting room of stages 1 and 2,












To compare the performance of SFS and OTC, we compare the “number of beneficiaries served,” denoted as






Transmission risk
One of the main objectives of WFP is to minimize the risk of COVID‐19 infections within the retail market, determined by the predicted number of new infections per day. For HOs, it is crucial to know which measures have a higher impact on reducing the transmission risk under both SFS and OTC layouts. The two most common measures under the COVID‐19 condition are increasing the social distancing and allowing beneficiaries to go shopping only at times scheduled through appointments. To assess the infection risk in a confined space, we used the so‐called Wells–Riley equation (WRE), which is one of the most popular models for estimating infection risk (Riley et al., 1978). The WRE allows us to predict the expected number of beneficiaries who can be infected within the retail store in a certain time frame.
We define the transmission risk index as the total number of people who can potentially be infected within the store ( the number of already infectious beneficiaries in the store ( the so‐called “quantum” generation rate produced by one infectious person ( the physical distance of the beneficiaries ( the time beneficiaries spend in the store (exposure time) ( other external factors like the pulmonary ventilation rate (
The functional form of the WR model is














Since our study investigates the impact of physical distancing on the operational and health performance, and given the fact that we do not have specific information on ventilation and quantum data, we aggregated the parameters




















Due to the lack of analytical tractability of the queuing network (a capacitated three‐stage tandem queuing system with blocking and a common waiting room on the first and second stages), we decided to solve the problem by means of discrete event simulation (DES). DES is a powerful tool for modeling and analyzing complex real‐world systems. DES is also useful because we are less interested in the steady‐state results of the queuing system; instead, we want to study the performance of the system during a certain time frame (i.e., store‐opening hours) and therefore use a terminating simulation. Typically, simulations that seek to investigate steady‐state systems remove so‐called start‐up bias by considering a warm‐up period in the simulation. In our case, however, we cannot remove these initial transient periods as they are a specific characteristic of the RIB system, since the retail store slowly fills during the course of a day. Depending on the time horizon, it is even possible that the system does not reach the steady state.
We used the simulation software SIMIO to perform all simulations. The input parameters of the simulation are described in the next section. For every set of input parameters and layout (the so‐called scenario), we performed 100 replications.
Case study: RIB in Mozambique
To analyze the effect of the layout design and preventive actions (for controlling transmission risk) on the retail operations of a RIB store, we collected real data from the RIB case in Mozambique.
Layout design analyses
In the Mozambique case, WFP was initially considering SFS and OTC layouts. The shopping and checkout times under the OTC layout were 10 and 4 min, respectively (







Note that from (14), the capacity of the shopping stage under SFS (















Figure 3 shows that while the NIS under the OTC layout is insensitive to social distancing, it drops significantly under the SFS layout. Under 0.8 and 1 m physical distancing, aligning with common belief, the SFS layout is always capable of serving more beneficiaries with the same number of staff. Hence in these two social distancing cases, the SFS is more profitable for the retailer and, at the same time, provides a higher dignity level when the beneficiaries are used to it. Surprisingly, the negative effect of increasing social distancing on the SFS layout performance is so intense that the SFS layout loses its advantages under 1.5 and 2 m social distancing.
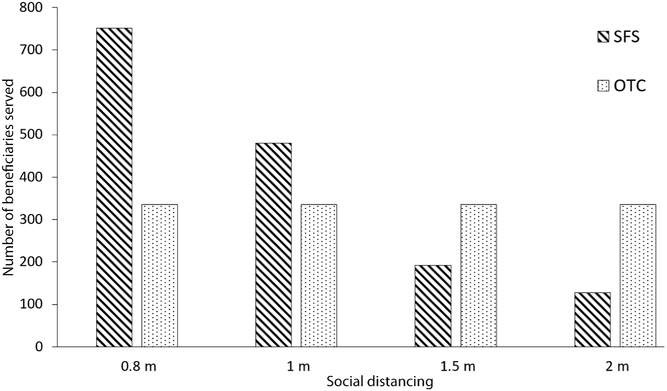
The maximum number of served beneficiaries for each layout design under different social distancing
Transmission risk analyses
We simulated the RIB store based on WFP's data, where the RIB store operates 6 days a week for 8 h per day, typically from 9:00 am to 5:00 pm. We assume that employees in the retail store work nonstop (without a break). Before checking in to the store, all beneficiaries need to sanitize their hands, which takes 15 s on average. The RIB's yard capacity is limited: As described previously, the shared waiting area encompasses both the check‐in and shopping stages, and has a size of






After entering the yard area of the RIB, beneficiaries arrive at the check‐in. The average service time for checking in a beneficiary is around 2 min, such that the service rate of a single check‐in employee is


Figure 4a shows that increasing the social distancing significantly reduces the transmission risk under both layouts. It illustrates that although beneficiaries spend three times longer on the shopping stage under the SFS layout (since many people can get served at the same time), the average time in the system (TIS) can be lower compared to the OTC layout and therefore the transmission risk is lower. Having said that, under higher social distancing (larger than 0.8 m), the SFS loses its advantage since the number of beneficiaries allowed in the store drops significantly while they still spend much more time in the store than in the case of the OTC.
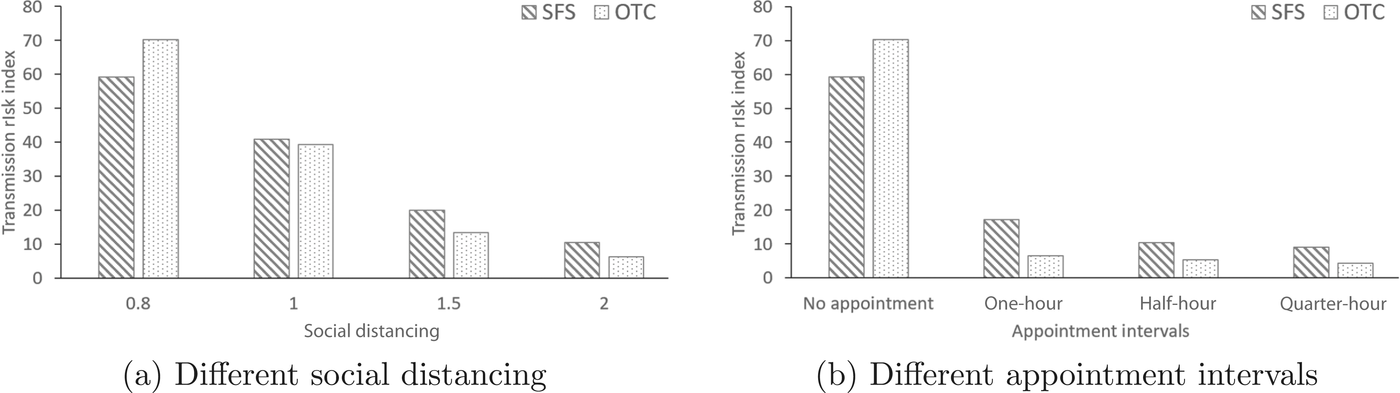
The effect of social distancing and appointment intervals on transmission risk under both layout designs
Besides increasing social distancing, another implemented preventative action was giving appointments to the beneficiaries to control store visits. Figure 4b shows the effect of giving appointments at different intervals on the transmission risk. To see the pure effect of the appointments, we consider no social distancing for all scenarios.
In Figure 4b, we compare four scenarios: (1) no appointment, where beneficiaries arrive based on a random arrival rate (in this case, not everyone gets served); (2) 1‐h, in which WFP gives appointments to the beneficiaries on hourly bases (e.g., 80 beneficiaries/h), considering the store's potential capacity (e.g., 640 beneficiaries/day); (3) half‐hour (e.g., 40 beneficiaries/30 min); or (4) quarter‐hour (e.g., 20 beneficiaries/15 min). It shows that offering fewer appointments in smaller intervals can dramatically reduce the transmission risk under both layouts. Note that arrival rates in all four scenarios are designed in a way to serve the same number of beneficiaries.
DISCUSSION, CONTRIBUTION, AND FUTURE RESEARCH
Discussion
In this study, we aim to better understand the impact of the WFP preventative measures for managing a pandemic‐like COVID‐19 on the operations of its partner retailers, and, consequently, on the performance of WFP's CVA programs. At the same time, we also see how the retailing operations contribute to the pandemic spread. Aligned with our first objective, we introduce RIB as one of WFP's initiatives, which aims to enable the CVA programs in places where they could not be operated before. We focus on the operational details of RIB's retailers and provide a holistic understanding of this initiative that other HOs could also benefit from.
To follow our second objective, in Section 4, we study retail competition in the RIB under a CVA program. We design stylized models with two retailers, who compete on their assortment sizes and prices under pre‐COVID (normal) and COVID (pandemic) conditions. We investigate the effect of WFP's preventive measures in a pandemic on assortments and prices in the RIB program.
We show that providing beneficiaries with appointments to visit the shops, as a preventive measure to manage the pandemic, indirectly affects the assortment competition of retailers, leading to higher assortments offered to beneficiaries. Specifically, we illustrate that when retailers are highly substitutable (e.g., retailers are located very close to each other) under the pre‐COVID condition, there is less competition between retailers and they prefer not to increase their assortments. Surprisingly, this does not occur under the COVID condition. Under the COVID condition, a higher substitutability of retailers always leads to higher competition and therefore larger assortment sizes. For WFP, it means that although giving appointments to beneficiaries to control store arrivals may reduce their power of choice, this has a positive effect on their shopping experience since the stores are less crowded and retailers provide higher assortments. To go one step further, when the COVID‐19 is over, WFP will likely return to normal conditions (like the pre‐COVID case) and stop giving appointments. Doing so, it is expected that retailers will reduce their assortment sizes again and the beneficiaries' choice power will decrease. This might be a crucial point for WFP to keep an eye on. It is vital for HOs to be aware of both the advantages of using the appointment system as a preventive measure during a pandemic like COVID‐19 and its consequences after the pandemic. We further show that under both pre‐COVID and COVID conditions, having a higher retail price and a lower marginal capital cost leads retailers to increase their assortment. Although HOs do not appreciate an increase in retail prices, reducing the procurement cost might be feasible in some cases. For example, if HOs help their retailers to get better deals from their suppliers, retailers will increase their assortment as a natural consequence of their competition on the assortment. This might simply be achieved if HOs support their retailers in their negotiations with their suppliers.
In the price competition, we show that giving appointment to beneficiaries indirectly makes the impact of assortment changes on retailers' prices less extensive, leading to more stable prices. Moreover, looking into the detail of price competition, we illustrate that when one of the retailers changes its assortment, all retailers adjust their prices leading to a new equilibrium. In both the pre‐COVID and COVID conditions, increasing one's assortment enables an increase in its price. However, the opponent's reaction depends on the products' characteristics. When beneficiaries' desirability for the product is rather high (like rice), or its procurement cost is sufficiently low, the opponent needs to either reduce its price or increase its assortment to avoid losing too much market share. The latter is more reasonable since these products bring more value compared to their costs. Therefore, these products are provided with the largest possible assortments and the highest prices allowed by WFP. Meaning, HOs should analyze the prices carefully and set the maximum price limits in a way that protects the beneficiaries while incentivizing retailers to provide enough assortment. However, if the product's procurement cost is high while its assortment is not highly appreciated (like farming tools), then when a retailer increases its assortment and price, the opponent slightly increases the price without expanding its assortment. Although some products (like rice) may have a higher importance from HOs' perspective, it is crucial that HOs monitor other products' prices in case the vouchers can be redeemed for all of a retailer's products.
To achieve our third objective, in Section 5, we analyze the impact of WFP's preventive measures for managing the COVID‐19 pandemic on layout design (as retailers' tactical decision). We considered two perspectives—service level and transmission risk—and modeled the entire shopping process. Due to the flexibility of the RIB initiative, WFP can adopt either a SFS or OTC layout depending on factors, like the local culture, the layout's efficiency, and the transmission risk under each layout (during a pandemic). We designed the model using a queuing network, but due to lack of analytical tractability, we used discrete event simulation. Both analyses were performed on real data from the RIB initiative in the Mozambique case.
First, we studied which layout is more effective and how social distancing (as a common preventive measure during a pandemic) affects the store's service level performance under each layout. Layout design analyses are highly relevant for countries that associate the SFS layout with a higher dignity level, like Middle Eastern countries. We show that under no social distancing, the SFS layout can serve twice as many beneficiaries as the OTC layout. However, increasing social distancing heavily dampens the SFS layout's performance due to limiting the number of allowed beneficiaries in the store. In contrast, the OTC layout is relatively insensitive to this measure. Meaning, while increasing social distancing is HOs' practical preventive measure, it significantly deteriorates the service level performance that one may expect from an SFS layout, but not from an OTC.
Second, we compared the impact of enforcing social distancing and giving appointments to the beneficiaries as preventive actions on the transmission risk of COVID‐19. We show that when enforcing social distance is the preferred preventive measure, then the OTC layout is safer in terms of the transmission risk while serving more beneficiaries. Appropriately, WFP has also adopted this approach of giving appointments to the beneficiaries. Being aware that this activity produces a huge workload for HOs, our analyses show that it is significantly more effective at reducing transmission risk than increasing social distancing. For example, in the Mozambique case, we show that giving hourly appointments to beneficiaries is even more effective than increasing social distancing to 1.5 m. This is a valuable insight for all HOs working with retailers under a CVA program or even during in‐kind distribution when beneficiaries are waiting in a queue. In practice, beneficiaries usually do not follow social distancing rules that carefully; this might cause health problems, which is far from HOs' objective. In these cases, giving appointments instead of requiring social distancing can be extremely helpful in reducing transmission risk under both SFS and OTC layouts.
In summary, our layout and transmission studies show that when social distancing is the only preventive measure, the best strategy is to switch to OTC due to it being faster and safer. However, switching to an OTC layout for people who are used to SFS might be perceived as decreasing their dignity. Also, OTC cannot serve as many beneficiaries as SFS under no social distancing. Therefore, if beneficiaries are used to SFS or the number of beneficiaries in need is huge, the best practice for HOs might be to avoid adopting the OTC layout and instead provide beneficiaries with appointments under an SFS layout. This is not only helpful with controlling the transmission risk but also provides the opportunity to serve a higher portion of beneficiaries in a shorter time.
Contribution and future research
Our contribution in this paper is fourfold. First, by introducing the RIB initiative, which acts as a CVA enabler for places without a functioning market, we contradict the common understanding about these programs by showing that they are applicable even in places without a functioning market. This initiative has gone one step further than what has been studied in the CVA literature and opens new frontiers for CVA programs.
Second, although one may expect that preventive measures against a pandemic like COVID‐19 can be restrictive and negatively affect the beneficiaries' experience, we show that this is not necessarily the case. Surprisingly, we illustrate that providing beneficiaries with appointments bolsters the retailers' competition, which leads to more stable prices and larger assortment sizes.
Third, although the OTC layout is perceived as a safer and faster layout, we show that when implementing a preventive measure is not possible, the SFS layout is comparatively safer in terms of transmission risk. The reason is that although beneficiaries spend more time in an SFS than in an OTC layout, the SFS layout can serve a good chunk of people simultaneously and reduces the waiting time outside the store. Moreover, while the common belief is that the SFS layout can increase the service level (serving more beneficiaries in a shorter time), we illustrate that this is not the case when increasing the social distancing is used as a preventive measure.
Last, we indicate that giving appointments to beneficiaries can have a higher impact on reducing transmission risk than increasing social distancing under both the OTC and SFS layouts. Interestingly, this provides the opportunity to take advantage of the higher service and dignity levels under SFS, while keeping the transmission risk relatively low.
Although this paper focuses on a specific case (Mozambique), our competition models, preventive measures analyses, and their consequent results are generalizable and valuable for any HOs providing assistance via a CVA program by contracting a few retailers. Moreover, it is possible to compare SFS and OTC layouts theoretically under different cases, while it might not practically be feasible to implement an SFS layout under all cases. One example is when beneficiaries are not familiar with the SFS layout (like in African countries) and do not perceive it positively. Another example is when the local retailers do not have the capacity to operate under an SFS structure and provide necessary goods and employees (like South Sudan's case).
To understand WFP's reaction to our findings, we shared our results with them and discussed potential follow‐up practice or theory questions. Based on their practical observations, our interviewees mentioned that beneficiaries might not fully follow the regulated social distancing rules, which makes controlling the transmission risk more challenging. Hence setting appointments helps with preventing the transmission risk. Moreover, they noted that using the appointment system as a preventive measure improved beneficiaries' shopping experience. Therefore, considering the positive impact of the appointment system on the retailers' competition and the consequent improved quality of service provided to beneficiaries, our key interviewee highlighted that WFP might use the appointment system more and more in the future, even after the pandemic.
From the practice perspective, WFP is now facing challenges to maximize the beneficiaries' access to highly fresh products by procuring them from local and smallholder farmers. So studying the implementation of inventory management of fresh products would be valuable. Another interesting research direction from WFP's perspective is investigating the impact of its assistance on retailers and the local economy in the long term. More specifically, WFP is interested in measuring how sustainable this business model will be for the retailers after terminating its assistance. Finally, they are considering using mobile RIB systems to improve access to beneficiaries.
Looking at our theoretically developed stylized models, we captured the competition of assortment and pricing in different games. One can extend these games by merging them and finding the simultaneous equilibrium of assortment and pricing. For analytical tractability, we assumed that each retailer provides beneficiaries with a single price no matter the assortment size. Relaxing this assumption provides an excellent opportunity to extend the model in future studies. Finally, we studied a single case of a RIB setting and did not provide comparisons with other HOs' CVA programs that might, for example, be experiencing conflicts. We consider this a limitation of our study that future research could rectify.
CONCLUSION
This paper examines the impact of the WFP's preventive actions for managing a pandemic like COVID‐19 on retailing operations associated with CVA. So far, the literature on humanitarian operations has merely focused on the role of HOs in CVA programs, although also local retailers play a critical role since their decisions have an impact on the whole system. Therefore, we investigate the retailer competition and retail operations based on performance measures like service levels, dignity, and pandemic‐related transmission risks. We specifically analyzed the WFP's RIB initiative, which focuses on enabling CVA in areas without functioning markets to maximize beneficiaries' service and dignity levels.
Our case study focuses on the Mozambique case, which utilized the RIB model. COVID‐19 is a severe concern for this location since the risk of disease transmission is even higher in locations that are marked by crowding and/or low hygiene, as is the case for refugee camps or markets. Although our results are related to WFP's RIB initiative in Mozambique, the results are valuable for other RIB models in different locations, as well as other HOs working with CVA during the pandemic.
Footnotes
ACKNOWLEDGMENTS
The authors would like to thank WFP, specifically the RIB team, for their generous support by providing access to their data and WFP's strategies. A special thanks to all interviewees whose thoughts helped shape this paper. Also, the authors are grateful to the editors and review team for their constructive and helpful comments.
1
Despite all the efforts that HOs like WFP have taken, COVID‐19 has expanded quickly in Cox's Bazar.
2
The WHO suggests adopting a one‐meter social distancing policy, while other countries require up to two meters (
3
Since the vouchers are limited in the RIB setting and earmarked to only a few operating retailers, it is reasonable to model the competition as an oligopoly game.