
Abstract
Universal health coverage (UHC) is an integral part of the United Nations sustainable development goals. The private sector plays a prominent role in achieving UHC, being the primary source of essential medicines for many people. However, many private healthcare facilities in low‐ and middle‐income countries (LMICs) have insufficient stocks of essential medicines. Simultaneously, these same facilities carry excessive quantities of other drugs, leading to obsolescence. This suggests poor inventory control. To propose potential remedies it is vital to fully understand the underlying causes. In semi‐structured interviews with managers of private healthcare facilities in Nairobi, we asked them about their (1) inventory control systems, (2) inventory control skills, (3) time/human resource constraints, (4) budget constraints, (5) motivations for inventory control, and (6) suppliers. Our results suggest that the problems are driven by resource limitations (budget and time/human resources), managerial issues (relating to skills and systems), and market mechanisms that limit overage and underage costs. Unavailability at the supplier level and motivations for inventory control are relatively minor issues. We posit that the key causes are interlinked and stem from wider issues in the market and regulatory environment. Our results challenge prevalent beliefs about medicine supply chains in LMICs and lead to novel hypotheses. Testing these hypotheses could improve our understanding of inventory management in private healthcare facilities and aid progress in achieving UHC.
Keywords
Introduction
“Nearly 2 billion people have no access to basic medicines, causing a cascade of preventable misery and suffering.”—Dr. Margaret Chan, Director‐General of WHO, 2007–2017
Universal health coverage (UHC) is an integral part of the United Nations sustainable development goals (UNSDG 2015). It is encompassed within UNSDG #3 in a reference to “…access to safe, effective, quality and affordable essential medicines and vaccines for all” by the year 2030. However, availability of essential medicines remains poor in many low‐ and middle‐income countries (LMICs) (Ewen et al. 2017, WHO 2013), and this can lead to adverse outcomes for patients as a result of not receiving treatment or treatment being delayed or discontinued (Elbireer et al. 2011, Mendis et al. 2007, Pasquet et al. 2010).
The private sector has an important role in achieving UHC in general, and specifically in improving access to essential medicines in LMICs (Frohlicher and Nouwen 2019, Yadav and Glassman 2019), where a very significant part of healthcare expenditure is not publicly funded (Chan 2018). However, availability targets for essential medicines are far from being met by private healthcare facilities, particularly in low‐income settings. For instance, using data from 36 LMICs, Cameron et al. (2009) calculated that the availability of 15 important generic medicines averaged 64.2% in the private sector (and 38.4% in the public sector).
Other studies too have identified a mismatch between demand and supply in private healthcare facilities (Ewen et al. 2017, Ongarora et al. 2019, WHO 2013), but rigorous and data‐based analyses of the underlying causes are lacking and the causes cited are rarely supported by solid evidence. Articles that do present data‐based analyses usually take a limited perspective—for example, focusing solely on supply issues or skills. This raises the risk of policy‐makers jumping to premature conclusions and focusing on ineffectual remedies.
In the context of LMICs, this exploratory study aims to answer the following research question: Why is there a mismatch between demand and supply in private healthcare facilities? Remedying the mismatch between supply and demand in private healthcare facilities is a key development priority and having a comprehensive understanding of the underlying causes is vital for proposing effective remedies (Yadav 2015). Availability of essential medicines not only impacts “health and well‐being” but also progress with other UNSDGs (Tosun and Leininger 2017). UHC can decrease poverty (UNSDG #1) and reduce social inequality (UNSDG #10). Health and well‐being are also closely related to economic growth and the ability to work (UNSDG #8).
Our work makes two major contributions to the Operations Management literature. First, it advances understanding of the inventory management practices in private healthcare facilities in resource‐limited settings. Since existing literature offers scant explanation for the observed mismatch between supply and demand, and findings from the public sector cannot easily be transferred to the private health facilities (see section 3), we use an exploratory research methodology. Based on our analysis, we put forward several propositions that should be tested in future work to further our understanding of inventory management in healthcare facilities in LMICs.
Second, we question the validity of mainstream assumptions in retail supply chain management models when applied to resource‐constrained settings. Penetration of point of sale (POS) data systems and automated inventory management systems in the last decade has improved inventory replenishment decisions in retail stores in industrialized settings, enabling inventory managers to focus more on (a) store execution (Chuang et al. 2016, Fisher et al. 2006, Raman et al. 2001, Xue et al. 2017), (b) improving assortment (Ton and Raman 2010) and replenishment decisions (Cachon and Fisher 1997, Fisher et al. 2001, Van Donselaar et al. 2010), and (c) understanding supplier‐retailer interactions. When applying mainstream retail supply chain management models to health product retailing in resource‐limited settings, it is not clear which deviations from the accepted modeling constructs are the most significant. 1 We highlight some of these deviations (see Table 4) in the belief they will help others select the right assumptions (and constraints) in future modeling‐based research in this domain.
Data for this study were collected through in‐depth, on‐site interviews with 39 facility managers making inventory decisions in private healthcare facilities located in low‐income areas of Nairobi. The sample is academically interesting for three reasons. First, given the pace of urbanization in LMICs, it represents a context that is becoming increasingly relevant (Management Sciences for Health 2014, United Nations 2018). Second, the inventory control decisions taken by the facility managers in our sample are sub‐optimal in a peculiar fashion: we observe low availability of many essential medicines and, at the same time, seemingly excessive quantities of other drugs. Third, as we show, two commonly cited causes of understocking—supply problems and lack of incentives for inventory optimization—are of relatively little importance for our sample (cf. Wagenaar et al. 2014).
Using semi‐structured interviews, we perform an in‐depth exploration of inventory management practices at these facilities on the following dimensions: (a) inventory control systems, (b) inventory control skills, (c) time/human resource constraints, (d) budget constraints, (e) motivations for inventory control, and (f) suppliers.
Our results suggest that poor inventory control skills, inadequate systems, limited overage/underage costs, and resource constraints are major causes of the observed mismatch between demand and supply. The last two seem to be exacerbated in part by two more fundamental issues: lack of regulation in the prescription drug market, and low barriers to entry. Lack of regulation allows healthcare facilities to substitute freely if they run out of stock of a particular drug and prioritize those available over those that are most appropriate. Low entry barriers lead to fierce competition, which appears to underlie budget problems and limit facilities’ opportunities to invest in developing skills and systems. Our results also add nuance to prevailing beliefs about the over‐ and understocking of essential medicines and corresponding solutions, and have implications for the WHO guidelines on quantifying availability.
In the sections below, we review the related literature (section 3), describe our methodology (section 4), and present our results (section 5). Finally, we discuss our conclusions (section 6) and their implications for policy‐makers and others who seek to improve the availability of medicines (section 7).
Background
In 2016, a large descriptive study of private healthcare facilities in Nairobi investigated medicine pricing (Ongarora et al. 2019), adherence to quality standards (Abuga et al. 2019), and availability of essential medicines. During this study, trained field agents did a physical inventory count at participating facilities to determine whether the items included in the Kenya Essential Medicine List (KEML) 2 were in stock. The field agents also used structured questionnaires to record details of all orders placed during an 8‐week period (October to December 2016) to analyze the ordering process (i.e., the rationale behind ordering decisions and selection of suppliers).
Analysis of the physical stock count data found that facilities stocked only 28% of the items on the KEML. 3 In other words, these private healthcare facilities were understocking essential medicines. Simultaneously many stocked excessive quantities of other drugs. 80% of the items recorded in our baseline stock count were not reordered during the next 8 weeks—that is, facilities held at least 8 weeks of stock for 80% of the items. Since lead‐times are very short in our study context (see section 5), and since high stock levels tie up scarce and expensive resources (such as shelf‐space and working capital), this is an indicator of overstocking.
The 2016 study was not designed to systematically and holistically assess why facilities have a shortage of many essential drugs and simultaneously stock excessive quantities of non‐essential drugs. In this study, we aim to fill this gap in our understanding about the causes for this phenomenon. As a first step, we review the possible explanations for this phenomenon based on extant literature.
Since we repeatedly refer to the 2016 study as a basis for our choices and decisions in this study, we outline the key components of both studies and how they relate to each other in Appendix C.
Literature Review
Grey and academic literature analyzing the over‐ and understocking of medicines in Nairobi or Kenya is scant. We found two studies that cover private sector facilities as well as public facilities and faith‐based health services (FBHS). A study by Health Access International (2018) used data from 82 facilities to show that locally produced products were more affordable and more available in the facilities surveyed. This suggests that cost is a driver of availability, which is understandable from an inventory holding costs perspective. Based on data collected from 108 facilities, a report by the Kenyan Ministry of Medical Services (2009) found that about two‐thirds of public and FBHS facilities lack qualified pharmaceutical personnel, which they argue goes hand in hand with stock‐outs and inadequate stock‐keeping records. Hence, qualified personnel appears to be a major driver of availability as well. Three other reports consider only public facilities. Muhia et al. (2017) and Wangu and Osuga (2014) found that problems with the availability of medicines in public hospitals could mainly be attributed to budget shortages, delays due to bureaucracy, distribution problems, lack of skilled personnel, inappropriate selection of medicines, irrational use of medicines, and an inability to accurately estimate requirements. This last issue “led to an overestimation or underestimation of the drugs needed” (Muhia et al. 2017). Budget shortfalls, supplier issues, and lack of skilled personnel were also identified as causes by Muiruri and Mugambi (2017), who studied 94 public healthcare facilities.
To obtain a more comprehensive view of current knowledge relating to over‐ and understocking of medicines in LMICs, we also performed a systematic literature review. We searched the PubMed and Web of Science databases for articles written in English within the last 20 years (going back from 1 October 2018), and available in full text. Search terms (see Appendix A) were chosen so as to find papers relating to (a) medicines, (b) over‐/understocking, (c) healthcare facilities, and (d) low‐income settings. Two authors independently assessed the abstracts of the resulting 150 articles. An article was included if its aim was to analyze availability of medicines in healthcare facilities in a low‐ or middle‐income setting, and if this analysis was based on data (primary or secondary). We subsequently read the resulting 20 articles to assess (a) the study sample, (b) what the causes of over‐ and/or understocking (if any) were said to be, and (c) whether data was presented in the paper to support these claims. Table 1 presents our results.
Causes of Over‐ and Understocking Mentioned in the Literature
Our review of the literature suggests that holistic, data‐based analyses of underlying causes are scant, particularly for private facilities. Only 11 papers discuss causes of over‐ and/or understocking and eight papers present data‐based evidence to support this discussion. Only two of the eight papers that analyze the causes—Ngcobo and Kamupira (2017) and Poku et al. (2017)—cover more than one category. None of the papers appears to take a comprehensive view of the causes. Moreover, none focus on private facilities. A similar conclusion was reached by Yadav (2015): “As with the public sector supply chains, there is lack of a systematic diagnostic methodology on why the private sector supply system cannot meet large public health objectives.”
The main supplier‐related causes of understocking reported include supplier stock‐outs, communication problems with suppliers, and insufficient resources to ensure reliable and frequent distribution. Inadequate inventory management policies (or no policy at all) and non‐adherence to such policies also explain why stock‐outs occur. Harding et al. (2014) found that they occur less in facilities with a reorder point. Leung et al. (2016) show in a simulation study that they occurred more frequently when there are inventory policies that are based on false assumptions regarding lead‐times and seasonality of demand. Other causes of stock‐outs include limited fridge capacity (for vaccines) and lack of pharmacy assistants (Ngcobo and Kamupira 2017). Among the papers we considered, the paper by Lauffenburger et al. (2011) is the only one to report on overstocking—the authors cited medicine donations as the main reason for it.
Our paper endeavors to fill the gap in our understanding of inventory management in private healthcare facilities in LMICs. Through a comprehensive qualitative analysis of possible reasons for the observed mismatch between demand and supply, we test several widely held beliefs about medicine supply chains in LMICs, and either debunk or add nuance to them. We also propose several hypotheses that could help spur much‐needed future work on private healthcare facilities in LMICs.
Sample Selection and Interview Methodology
In section 3, we noted that the existing literature is silent on why private healthcare facilities in Nairobi have a shortage of many essential drugs, while simultaneously stocking excessive quantities of non‐essential drugs. To investigate this phenomenon we went back to the same sample that participated in the 2016 study, with the purpose of understanding, “Why is there a mismatch between demand and supply?”. This is a “why” type question, as opposed to a “what” type. In other words, we do not use data to test an existing theory or a pre‐formulated hypothesis claiming a causal relationship. Our research is exploratory: the exact nature of the theory that would shape up from this study is not known beforehand. For such exploratory questions, taking the context into consideration is crucial, and qualitative studies are seen as most appropriate (Baxter et al. 2008).
The population from which the study sample was drawn consists of 381 private healthcare facilities in Nairobi County that were affiliated to PharmAccess Foundation Kenya, an NGO that offers healthcare financing, digital health and healthcare supply solutions to make quality healthcare accessible and affordable to Kenyans. Ninety‐one facilities met the inclusion criteria of having a valid license and selling drugs to patients at the bottom of the wealth pyramid. Facilities in low‐income areas in Kibera were excluded because in that locality there are several NGOs providing free healthcare services, which may impact competition and the way those private facilities operate. Forty‐eight facilities were subsequently selected for inclusion, considering (a) accessibility, (b) distribution of facilities across parts of the county, and (c) representation of different types of facilities. The selection was done by three co‐authors with expert knowledge of the local market. Forty‐five of the facilities consented to participate in the 2016 phase of the study.
To recruit facilities for the 2018 study, we approached the 45 facility managers in November 2018 and told them about the purpose, benefits, and risks of the study. Those who agreed to participate were asked to provide written consent to their data being used for research purposes, but they were allowed to withdraw from the study at any time. No financial incentives were offered to the facilities to participate, nor were there any negative consequences to facilities that chose to not participate. However, during the recruitment phase facilities were promised a post‐analysis town hall meeting where results from our studies would be shared.
Though we believe our results have a reasonable degree of external validity for similar settings in LMICs, we stress that the primary intent of qualitative research “is not to generalize to a population, but to develop an in‐depth exploration of a central phenomenon” (p. 206, Creswell 2009) (we revisit this in section 7). The aim is to learn from “information‐rich” interviewees who can best help in understanding the observed phenomenon—over‐ and understocking in private healthcare facilities—and to reach “information saturation” or the point when “no new information or themes are observed” with each subsequent interview (Guest et al. 2006). Our 2018 sample forms a unique set of “information rich” interviewees. Guidelines suggest that semi‐structured interviews require a sample between 25 and 30 interviewees to achieve information saturation (Lewis 2015, Symon and Cassell 2012), and in this respect, we initially believed our 2018 study sample was sufficiently large despite the withdrawal of few facilities. This belief was confirmed during the actual field work, when interviewers reported information saturation approximately after the first 20 interviews.
The 2016 sample consisted of 18 clinics, 7 hospitals, 2 health centers, 4 medical centers, 2 nursing and maternity homes, and 12 pharmacies. We refer the reader to Ongarora et al. (2019) for details on respondents and additional facility characteristics. Of the 45 facilities that took part in the 2016 phase, 39 did so again in the 2018 phase: one hospital and three pharmacies declined to participate, and two clinics had by then shut up shop. Our 2018 sample therefore consists of 16 clinics, 6 hospitals, 2 health centers, 4 medical centers, 2 nursing and maternity homes, and 9 pharmacies. Interviewees had on average 11.3 years of work experience in the pharmaceutical sector. Among them were 9 clinical officers, 3 doctors, 11 nurses, 9 pharmaceutical technologists, and 6 pharmacists (see Appendix B for the pharmaceutical terminology).
To construct an interview guide for the 2018 study, we followed a commonly accepted methodology formalized by Kallio et al. (2016). Appendix E reviews how our process follows the steps that they laid out. We chose a semi‐structured interview format as it is considered to be “flexible, accessible, intelligible and capable of disclosing important and often hidden facets of human and organizational behavior” (Qu and Dumay 2011). Most importantly, it enables interviewees to provide responses in their own terms and in the way that they think and use language, making it the most effective and convenient means of gathering information for an exploratory descriptive study (Kvale and Brinkmann 2009).
By aggregating the causes suggested in the literature (see Table 1), we formulated a preliminary semi‐structured interview guide designed to assess each facility's (a) inventory control systems, (b) inventory control skills, (c) time/human resource constraints, (d) budget constraints, (e) motivations for inventory control, and (f) relationship/issues with suppliers. Several open questions were included to capture potential causes not covered by these categories. The interview guide was reviewed by each author and two other academics with an advanced knowledge of the topic. We then piloted the guide during three facility visits in August 2018 and finalized it afterwards (e.g., we aligned the jargon with that of the interviewees). We present the final version of the interview guide in Appendix F.
Interview Analysis
In the spirit of semi‐structured interviews, the questionnaire was designed to prompt interviewees to give as full an answer as possible to questions, and thus lead the discussion to other tangentially related issues. Interviewers spent significant amount of time at each facility taking pictures and noting observations about the facilities. In most cases, the facilities were run by just one or two people—thus inventory management is just one aspect among many things they need to look after to keep the facility running. Several times during the interviews the interviewees excused themselves to attend to clients.
Each interview included at least two interviewers: The fourth author was present in every interview to ensure consistency and was accompanied by a Nairobi local. On average the interviews took 83 minutes. They were taped and later transcribed by an independent agency.
The transcripts were analyzed using NVivo 12 text analysis software. Before we began the text analysis, we read through all the transcripts end‐to‐end, to familiarize ourselves with the full content of our interviews. In the first stage of the text analysis, parts of the interview that provided direct answers to the pre‐planned questions (see Appendix F) were identified and tagged to the appropriate question.
For instance, question 14 asked, “Why is it important for you to have drugs on stock?,” and was meant to explore the interviewee's motivations and incentives for stock‐keeping and inventory management. Since our interviews were semi‐structured, the conversation could touch upon motivations and incentives several times throughout the interview. All parts of the interview in which the interviewee discussed motivations and incentives to stock drugs were labeled “Motivations.”
In the next stage of the analysis, we collated all the parts of the transcripts associated with each label, re‐read them, and assigned further lower‐level tags (sub‐labels) to the collated text. For instance, several possible scenarios were identified as answers to the question, “What happens when the drug a client needs is out of stock?” After going through all the answers (across all the transcripts) to that question, we created a list of mutually exclusive and cumulatively exhaustive list of sub‐labels associated with each scenario. Whenever an interviewee mentioned a certain scenario, the corresponding sub‐label was attached to that part of the transcript.
When a discussion topic emerged that was not covered in the questionnaire, a new label was created and all the relevant parts were tagged under that topic. For instance, from Appendix F it is clear that the questionnaire included no mention of “regulatory issues” as a topic, but several interviewees brought up issues related to government regulations when discussing their inventory management practices.
Finally, to perform an objective and quantitative analysis, we formulated several variables, which took a binary value of 0 or 1 based on each facility's responses. One example is, “At least one of the facility's suppliers currently offers a line of credit.” The definitions of these variables and their objectivity were discussed by the co‐authors and iteratively refined until consensus was reached. All the statistics reported from the interviews are based on such objective variables (see Table 3 for a list of variables).
Upon completion of our analyses, we invited all the participants to a workshop at which we presented and discussed the results (see section 4.2). Nineteen participants attended. The workshop allowed us to “member‐check” the results and hypotheses presented in the following sections.
Ethical approval for the study was granted by University of Nairobi‐Kenyatta National Hospital Ethics and Research Committee (UoN‐KNH ERC) under approval number P549/07/2016.
Insights Dissemination Workshop
In August 2019, after completing the bulk of the analysis for this study, we returned to Nairobi and held a workshop for interviewees to share our insights with healthcare facility managers, and corroborated our thought process in this study. The facility managers also participated in a root cause analysis using the “5 times why” approach (Ohno 1988). We will refer to insights from this workshop in our discussion (section 6) and conclusions (section 7).
Results
This section presents our findings on causes of over‐ and understocking related to (a) inventory control systems, (b) inventory control skills, (c) time/human resource constraints, (d) budget constraints, (e) motivations for inventory control, and (f) suppliers.
Our data reveals that the facilities give little consideration to inventory control systems, which may partly explain the over‐ and understocking. Interestingly, while 95% of the facilities (37 out of 39) are familiar with the concept of a “reorder point,” hardly any have formulated an explicit policy stating exactly what the reorder points should be. We find similar patterns for order quantities and review periods. Instead, decisions are largely based on intuition and experience.
Some facility managers make a physical check of inventory levels at the point they decide to place an order and decide to buy new supplies of medicines that they deem most urgent. Others keep a running list of medicines for which they judge the current inventory levels to be too low, which is periodically transformed into an order. Exactly when the order is placed is often an opportunistic decision depending on time and available budget and the urgency of re‐supply (e.g., because a patient is waiting for a drug). The quantity to be ordered is sometimes determined at the last minute.
Facilities make little use of historical data. About 77% of the facilities (30 out of 39) reported keeping sales records and 79% (31 out of 39) reported keeping historical purchase data. Even though 31% (12 out of 39) had an IT system for inventory management, only 10% (4 out of 39) reported using data for decision‐making. Facilities that do so followed a hybrid approach, using historical data to extract demand rates or to obtain a recommended order quantity and combining this with their personal judgment when making ordering decisions.
Use of manual or IT tools for inventory control is also scarce in our sample. Forty‐four percent of the facilities (17 out of 39) had no tools to keep track of their inventory whatsoever—neither manual nor IT based. Twenty‐six percent (10 out of 39) had a bin‐card system in place. However, based on the subjective judgment and interviewers’ notes,
4
9 out of the 10 facilities with a bin‐card system (90%) were not using it properly or consistently.
The same applies to IT tools used for inventory control. Many were not fit for purpose, underutilized, or not consistently used. According to the interviewers’ subjective judgment and their interview notes, in only 42% (5 out of 12) of the facilities could the IT system be considered “adequate” for purpose and used consistently. Twenty‐five percent of the facilities (3 out of 12) had an IT system that was not fit for the purpose of inventory management in the context of that facility. Another 25% (3 out of 12) facilities had an IT system but did not use it consistently; and 8% (1 out of 12) had a system but did not use it at all. These observations raise questions about the cost‐effectiveness of IT solutions for inventory control in the kinds of facilities represented by our sample. We return to this discussion in section 7.
When asked to enumerate the factors that are considered when determining reorder points and order quantities, 97% of the facilities (38 out of 39) mention rate of consumption, but only 13% mention lead‐time. Holding and shortage costs were rarely mentioned explicitly. Most facilities order “when they are almost out of stock.”
Though this decision rule is loosely specified, choosing to order when stock levels are low appears to be rational because lead‐times are small and stock‐out costs tend to be low. We discuss this in more detail later. Hence, although these factors were rarely mentioned explicitly, they may have been implicitly incorporated.
On the other hand, inventory management theory stresses that the stock‐out rate is a choice one can make by setting the reorder point. However, this link between reorder points and stock‐outs appears to be poorly understood and rarely acknowledged by interviewees. They primarily mention external factors as causes, that is, “high consumption by patients” in 69% of cases and “supplier shortage” in 20% of cases. Acknowledging that one “ordered too late,” which is a different way of saying that the reorder point was too low, occurred in only 3% of cases. This may exacerbate understocking.
We also asked interviewees why specific order quantities were chosen. While 46% of the facilities (18 out of 39) are familiar with the concept of “order quantity,” they were unable to offer a satisfactory rationale for the specific order quantities chosen.
When discussing order quantities, interviewees did not mention ordering costs; this is understandable since all of them indicated that they do not pay delivery fees. However, it is surprising that holding costs are rarely accounted for. Only 14% mention that budget (for which holding costs could be seen as an indicator) affects quantity decisions. Instead, 64% report that order quantities are based on consumption rates—more demand means larger order quantities—which can be far from optimal. Facilities also made too much use of stock investment heuristics. This general failure to consider holding costs may at least partly explain the overstocking phenomenon.
Our dataset does not allow us to assess the second aspect of inventory control skills, the capability to devise and adhere to policies and processes, since none of the facilities uses explicit inventory control policies.
We believe that some of the facilities would benefit from hiring staff to take over mundane tasks, as this would free up the manager's time to deal with other issues. However, they report that it is hard to find trustworthy personnel. Pilferage on the premises had been experienced by 69.2% of facilities (27 out of 39), in most cases by a staff member.
We did not explicitly ask interviewees to state the reasons for their financial constraints. However, during the course of a few interviews, delayed payments by the National Hospital Insurance Fund (NHIF) were cited as a reason.
The reported level of cash‐flow constraints is surprising considering that 69% of facilities (27 out of 39) are offered a line of credit by at least one of their suppliers. However, not all interviewees had a positive view of such credit options. Interviewees said that they did not like to be “indebted” to their suppliers. This suggests that facility managers lack the necessary understanding of how risk‐sharing contracts can benefit them. On the other hand, a few interviewees expressed concern that having a line of credit leads them to purchase more than is necessary, because the transfer of money for goods purchased is not immediately salient. This suggests that, similar to inventory decisions, financial decisions are largely driven by intuition (gut feeling).
The findings from the 2016 phase of the study indicated that facilities assigned on average 65% weight to demand and 28% to whether the item is on the KEML list when determining whether or not to stock a drug. They thus have a particular incentive to stock items for which there is high demand, and to stock medicines that are essential for their clients.
As stressed by newsvendor theory (Axsäter 2015), incentives to avoid understocking are stronger when the shortage costs—the opportunity costs of not being able to meet a demand from stock —are high. Interestingly, 74% of the facilities (29 out of 39) indicate that they can backlog demand, suggesting that shortage costs are low. If they run out of a certain medicine, they can order it for the client to pick it up at a later time. A few facilities report that they request partial payment to ensure pickup.
Seventy‐two percent of the facilities (28 out of 39) report that they offer the client a substitute drug when they experience a stock‐out. Fifty‐six percent of the facilities (22 out of 39) report that they turn to neighboring facilities to "borrow" the necessary drugs.
As a last resort, facilities can also give out a prescription that the client can use to purchase the medicine at a different facility. However, this would mean a loss of business for the facility giving out the prescription. Forty‐six percent of the facilities (18 out of 39) report that they would recommend a specific trusted pharmacy to the client when giving out a prescription.
The fact that delivery lead‐times are short (see below) suggests that stock‐outs have relatively few health implications for patients in terms of their treatment being either delayed or discontinued. Hence, though facilities appear to have a strong drive to minimize costs and maximize service to clients, there is not a strong incentive to avoid stock‐outs.
We now turn our attention to assessing motivations to minimize inventory holding costs. We provide a rough estimate of these costs based on the value (procurement costs) of the inventories recorded during the 2016 baseline assessment. As we did not collect procurement costs directly, we estimate them by applying a 33% sales margin to the retail price (the average margin on products procured during the eight‐week study period). The majority of the facilities (35 out of 45) could not provide any detailed information on retail prices, which were therefore excluded from this analysis. For the remaining 10 facilities, the average inventory value is 229,454 Kenyan Shillings (KShs), which is about 2,200 US dollars. Applying the rule of thumb that annual holding costs are 25% of the average inventory value (Azzi et al. 2014), we estimate that average annual holding costs equal 57,363 KShs (555 dollars), which is a considerable sum in the context of our study. It is therefore surprising that substantial overstocking occurs despite the observation that facilities have a strong drive to minimize costs.
Our interviews also shed light on a worrying practice we call demand shaping, that is, the practice of prescribing and pushing drugs that are available in stock rather than those that are most appropriate for the client's needs. A lack of regulatory oversight incentivizes facilities to stock and prescribe broad‐spectrum and unnecessarily strong drugs for a wide range of patient complaints. Such practices could potentially lead to an increase in anti‐microbial resistance.
However, supplier‐related causes are only a minor issue for several reasons. First, the number of suppliers serving Nairobi is high. In both data‐gathering phases, we asked facilities to list their suppliers, which yielded 112 unique names. Seventy‐seven percent of the facilities (30 out of 39) have at least three suppliers from whom they regularly source medicines, and 90% of the facilities (35 out of 39) report reaching out to other suppliers when their main supplier runs out of stock for a certain drug.
Second, the vast majority of orders (91%) are delivered the same day. Delivery time is so short for most facilities that only 13% of them (5 out of 39) factor delivery lead‐time into their ordering decisions and only 23% of the facilities (9 out of 39) consider maintaining a buffer stock to hedge against unexpected delivery delays. Third, in 84% of cases, facilities received all the medicines they ordered.
Suppliers can also cause overstocking by incentivizing facilities to purchase large quantities through promotions and offers. Almost all the facilities report that they are approached by their suppliers with such offers. While 79.5% of the facilities (31 out of 39) report that they do not budge from their order quantity decisions on the basis of such offers, some respondents may be tempted by these offers.
Table 2 summarizes the key insights generated from our interviews for the six categories of causes we considered. Table 3 contains a list of questions with binary answers used to present the statistics in section 5.
Key Insights from Our Interviews, by Category
Overview of Responses
Discussion
Streamlining medicine supply chains in LMICs is a necessary condition for achieving universal health coverage, as targeted in the United Nations Sustainable Development Goals 2030. Very little healthcare provision in these countries is publicly funded; most patients pay for medical expenses from their own pockets (Chan 2018). Thus, the private sector has an important role to play in achieving these goals.
Field studies conducted in 2016 revealed that private healthcare facilities in Nairobi's low‐income areas stock seemingly excessive quantities of many drugs, yet they have no stock of many essential medicines. Since these facilities are privately owned, they are clearly profit‐driven and have complete control over their inventory management choices. Thus, such a pronounced mismatch between demand and supply would suggest that deeper factors are driving this behavior.
In the interviews conducted in 2018, we investigated this over‐ and understocking of medicines and assessed each facility's (a) inventory control systems, (b) inventory control skills, (c) time/human resource constraints, (d) budget constraints, (e) motivations for inventory control, and (f) relationship/issues with suppliers (see section 5). In this section, we will discuss the causes related to each of these categories, elaborate on the relationships between them, and interpret them in relation to our context. We put forward several propositions that can guide future research into this issue.
As shown in section 5, supply problems play a negligible role in causing over‐ or understocking of medicines. Even when facilities occasionally encounter stock‐outs at their primary supplier, they have access to an abundance of alternative suppliers. Given that availability at the supplier‐level is high in many urban contexts in LMICs (Yadav and Glassman 2019), we hypothesize that:
Low availability of medicines in private healthcare facilities located in urban neighborhoods in LMICs is primarily driven by facility‐level issues rather than by unavailability at the supplier level.
Our analysis shows that these facility‐level issues are weak systems, lack of skills, budget constraints and, to some extent, time/HR issues. Section 5 highlights how facilities do not take advantage of historical orders and sales data to make inventory management decisions but overly rely on their intuition and experience. Facility managers also report inconsistent and ineffective use of inventory control tools. Moreover, many lack an understanding of the link between reorder points, order quantities and stock‐outs. We also find that almost all facilities face budget constraints when implementing their inventory management strategy. These findings coincide with the subjective judgment of the interviewers, who sat together after each interview to assess the scale of the problem faced by that facility in each of the six categories shown in Figure 1.
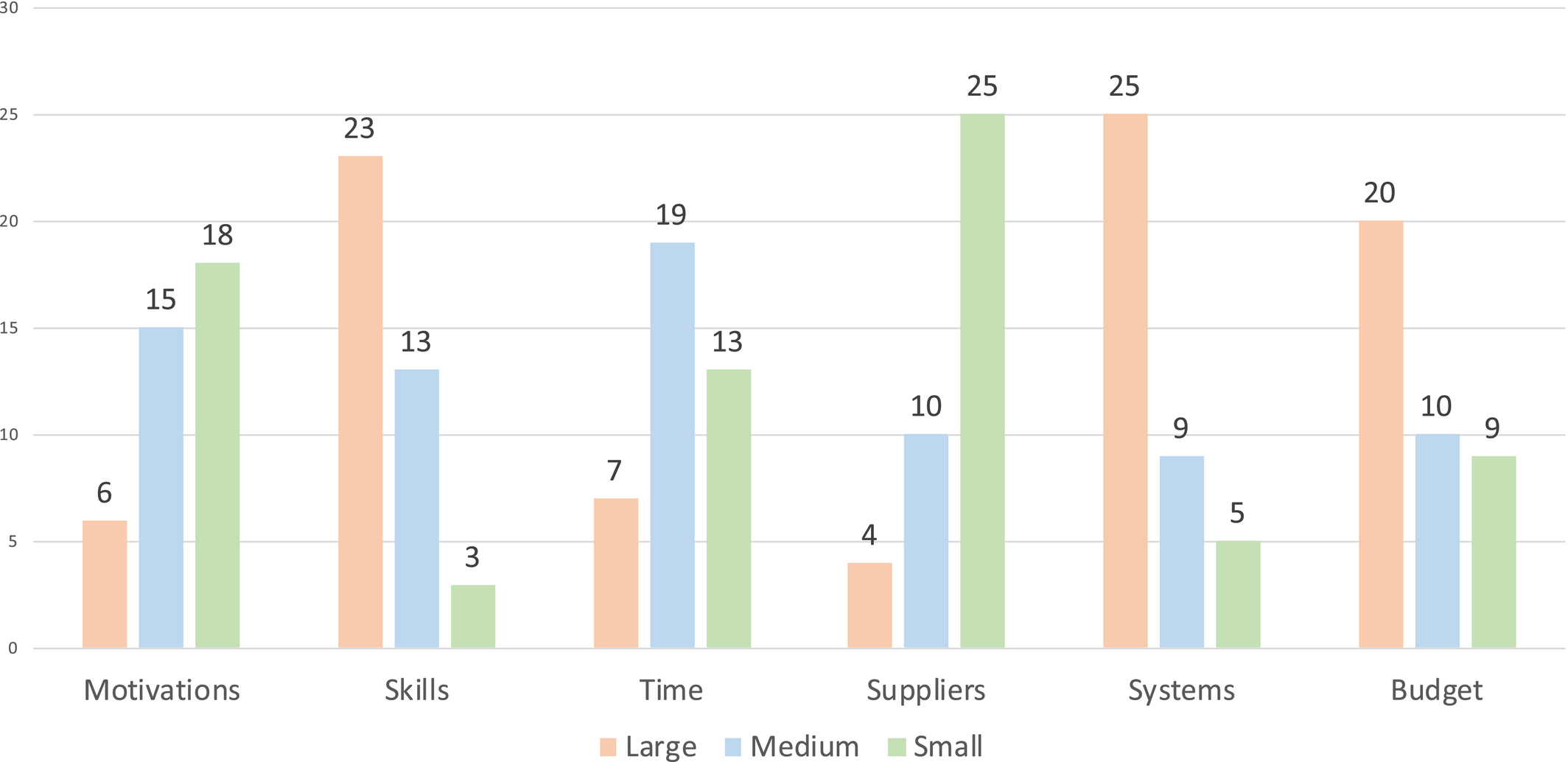
Interviewers’ Subjective Judgement of the Scale of the Problem. Note that motivations and suppliers are usually perceived as minor problems, time as a moderate problem, and skills, systems, and budget as major problems [Color figure can be viewed at
Our analysis also finds that these facility‐level issues are not due to a lack of motivation to ensure inventory control but may be driven by insufficient incentive to optimize those control parameters. That is, we find that facilities are motivated to maximize both profits and patient satisfaction (and therefore aim to stock items in high demand; cf. section 5), but have little incentive to maintain high service levels. Facilities can easily “borrow’ inventory from a neighbor or backlog their demand. This is facilitated by the very short lead‐times and the large number of suppliers in the market, which drastically reduces the facilities’ underage costs and the impact of stock‐outs on their clients. In the 2016 study, when asked to score the importance of attributes by which patients purchase drugs, facility managers assigned only 14% of the total weight to availability (as against 34% to price, 24% to quality, and 16% to efficacy). This leads to the following hypothesis:
Private healthcare facilities in LMICs choose not to stock many essential medicines because they perceive the underage costs for those medicines to be so low that there is no financial rationale for stocking them.
On the other hand, facilities report substituting prescribed drugs with what they have in‐stock. This goes against regulations, but there is little or no enforcement. A consequence is that overage costs are limited, so overstocking is not considered a problem.
Holding too much stock of a certain medicine makes it more likely that the medicine will be prescribed, even though there may be better alternatives.
Figure 2 summarizes the six proximate causes, which we classify into three broad classes: (a) structural causes—external issues that affect the incentives to avoid over‐ and understocking, (b) managerial causes—internal issues relating to the way inventories are being managed, and (c) resource limitations (human and monetary).
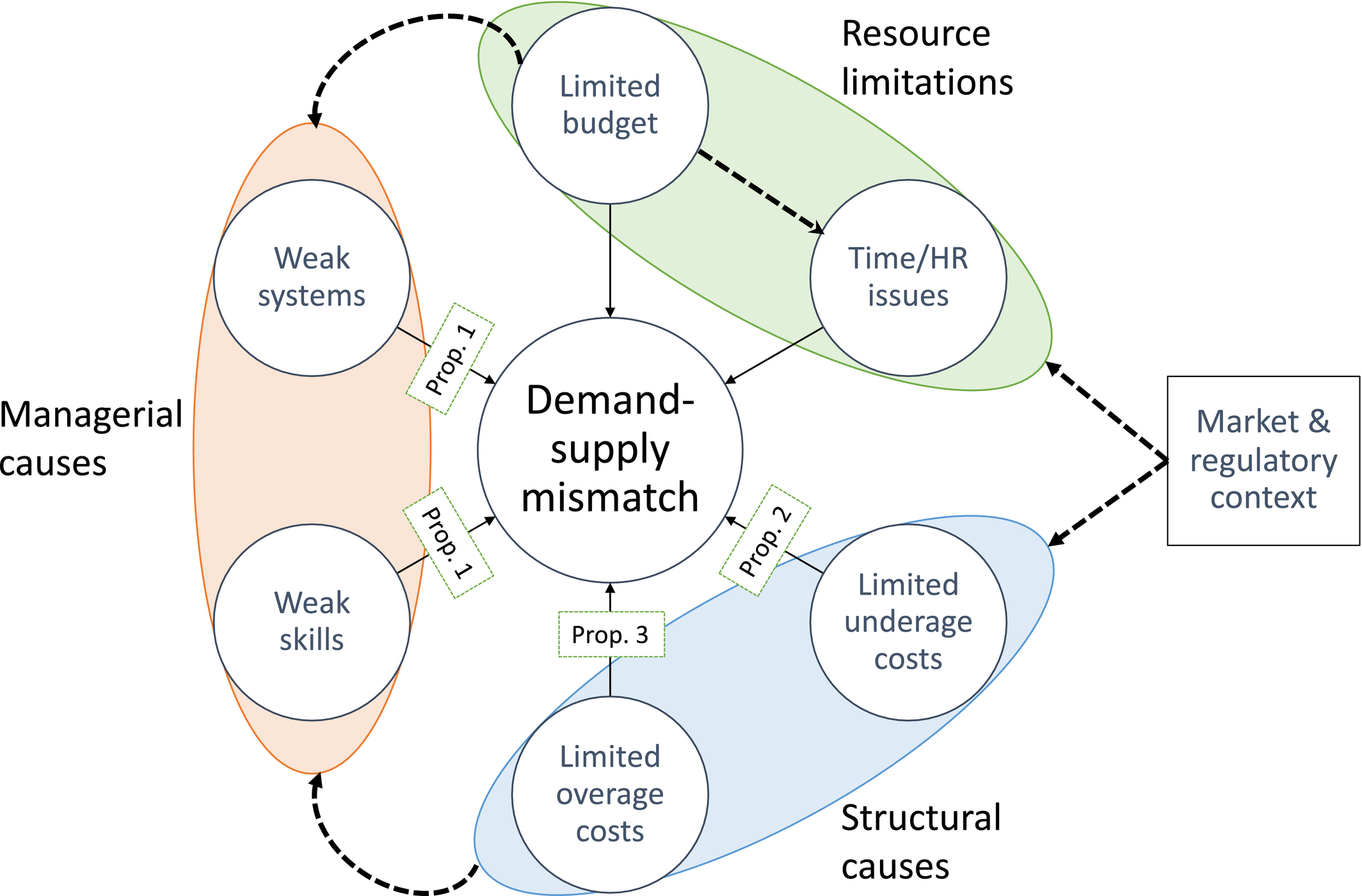
Causes of Demand‐supply Mismatches in Private Healthcare Facilities in Nairobi. Solid arrows indicate a direct link between a cause and demand‐supply mismatch. Dashed arrows indicate hypothetical exacerbating linkages between causes [Color figure can be viewed at
It is important to note that these causes are not independent of each other. We posit strong linkages between them and deeper factors that cause them to spread, 5 as represented in Figure 2 (see the dashed arrows between causes), acknowledging that there is a need for further research to substantiate them.
First, budget constraints not only directly influence stock‐outs but aggravate other problems, potentially leading to a downward spiral in inventory management performance. During a feedback and dissemination workshop for interviewees in 2019, we let participants perform a root cause analysis using the “5 times why” approach (Ohno 1988). Budget came up as an issue that influenced (a) skills (no budget for inventory management training), (b) systems (no budget for professionalizing inventory control systems), and (c) time/HR (no budget to hire extra personnel, and low budget for salaries leads to high staff turnover).
Second, we posit that structural issues also influence managerial factors. Zomerdijk and De Vries (2003) note that, in many cases, poor inventory management performance triggers a “diagnosis” of the situation. However, due to the limited overage and underage costs in our context, that did not seem to happen in many facilities. This keeps the facilities from investing in improving their skills or implementing efficient inventory control systems.
Finally, these proximate causes seem to be driven by deeper issues that are linked to the market and regulatory context. In Nairobi, the client population is poor and the density of facilities is high: 6 1.24 per square kilometer (Baker et al. 2014). Hence catchment areas and sales margins are small, demand is low, and demand variance high. Low demand limits their budgets and opportunities to invest and professionalize, exacerbating the managerial issues. 7 Furthermore, market conditions and regulation also influence the structural causes. As noted in Propositions 2 and 3, market conditions and lack of proper enforcement allows demand‐shaping and informal inventory‐pooling networks to develop, softening both the economic impact of the demand‐supply mismatch and its impact on patients.
We note that our findings cannot be deduced from findings on the public sector healthcare facilities in LMICs. For instance, “diffuse accountability” and “lack of incentives for supply chain staff” was identified as a root cause for stock‐outs in public sector healthcare facilities (Yadav 2015), whereas our interview results suggest that motivations and incentives are not a concern for most of the facilities in our sample. Similarly “long resupply intervals” was identified as another root cause for mismatch between supply and demand in public healthcare facilities. However, our interviews reveal that the delivery lead time for most facilities in our sample is less than one day—in fact it is often in the order of hours.
Our analysis also identifies several differences between mainstream retail inventory management assumptions (typically based on industrialized settings) and the realities of health product retailing in resource limited settings (see Table 4). We hope that the propositions laid out in this study, together with the differences identified in Table 4, will help others make the right assumptions (and constraints) in future modelling‐based research in this area.
Differences Between Mainstream Retail Inventory Management Assumptions and Inventory Management Realities in Private Healthcare Facilities in Low‐ and Middle‐Income Countries (LMICs)
Even though the primary purpose of our study is exploration, we believe our insights have a reasonable degree of external validity. First, we endeavored to ensure the sample was representative of the population of urban private healthcare facilities in Nairobi—by asking three co‐authors with expert knowledge of the local market to select them. Second, our study setting is similar to other urban settings in LMICs, that is, markets with poor clients where there is a high density of severely resource‐constrained facilities and suppliers, and facility managers who have not been well‐trained in inventory management (Yadav and Glassman 2019). In the following section, we discuss the implications of these conclusions and potential avenues for future research.
Conclusions and Further Research
Our results add nuance to prevailing beliefs about medicine supply chains in LMICs, which in turn is crucial to streamlining efforts to achieve universal health coverage. Additionally, they shed light on differences between inventory management in mainstream retail supply chain management models and medicine supply chain management in settings where resources are limited.
The first belief we challenge is the notion that poor availability at the facility level is caused mainly by supply‐related issues (see, e.g., Muiruri and Mugambi 2017, and our literature review). Our results show that facilities in urban settings have access to an abundance of suppliers, and that supply‐related issues are not the cause of low availability or understocking in private healthcare facilities (see Proposition 1).
Second, we challenge the belief that IT provides a solution for medicine supply chain challenges in LMICs. Though IT definitely has great potential there (see Matchaba 2019, USAID 2019, USAID—Deliver Project, 2011), our results show that this applies only to a limited extent. Several facilities in our sample had invested in inventory control software, but had not observed the potential benefits. Our findings show that IT systems are often not fit‐for‐purpose or not consistently used. Many functionalities are not fully utilized. The basic skills and processes required for successful implementation are often lacking, and so too is buy‐in from staff.
Facilities and organizations working toward UNSDG #3 and trying to improve medicine inventory control through IT need to realize the importance of tackling these issues. In line with Yadav (2015), we observe that the return on investment in inventory control systems is heavily influenced by factors such as such as number of products a facility holds, its weekly revenue, and training of staff. A more detailed study is needed in order to make evidence‐based decisions on investing in inventory systems.
A third (latent) belief we challenge is that overstocking is not a major problem. Our interviewees hardly gave it any thought, and it is largely ignored in the academic literature. First, we estimate that overstocking incurs substantial holding costs (cf. Yadav et al. 2012). Overstocking for one product, for example, may tie up the capital required to avoid stock‐outs of other products. Second, many facilities (72%; 28 out of 39) admit that they give alternative or substitute drugs whenever they do not have the prescribed medicine in stock. Worryingly, some admit to changing their prescription behavior based on what drugs they have in stock. This implies that overstocking incentivizes facilities to engage in demand shaping. Such practices can clearly be harmful for patients and should be investigated through further studies. If confirmed by follow‐up studies, appropriate laws and policies may be required to deter such behavior.
A fourth belief is that low availability is harmful for the facility, as is typically assumed in inventory management theory (Axsäter 2015). Simulations by Yadav et al. (2012) confirm this in a context in which travel times to suppliers are long (several hours). However, we find that when a facility runs out of stock of a certain drug, it does not necessarily lead to lost sales. It can often backlog demand (due to short lead‐times), substitute another drug, or get supplies from neighboring facilities (see Proposition 2).
Conventional inventory management wisdom suggests that facilities’ ordering decisions depend on supplier stock levels. The short lead times reported by facilities in our study are an indication that suppliers are holding sufficient stock. However, we know that the preference for centralized holding of inventory at the suppliers vs. decentralized holding at healthcare facilities is determined by market search costs (Anupindi and Bassok 1999). Given our finding that healthcare facilities share stocks with each other and can backlog demand to some degree, it warrants further examination of optimal inventory levels for facilities in this setting.
Finally, our results question the implications for patients’ health due to low availability at the level of individual retail healthcare facility. We believe that in settings where clients have access to many facilities without significant transportation or physical barriers, where facilities themselves have access to many suppliers, and where supply lead‐times are short, the impact of stock‐outs at an individual retail facility may be less severe than commonly believed (Elbireer et al. 2011, Mendis et al. 2007, Pasquet et al. 2010). Further research is needed to determine at which level of aggregation stock‐outs lead to poorer health outcomes, but the issue is pertinent given the substantial resources invested in addressing these perceived challenges.
Our findings also raise questions about the prevailing practice of quantifying availability through stock levels at healthcare facilities, as recommended by the World Health Organization (2008). Holding in stock only 20% of items on the Kenya Essential Medicines List may sound problematic, but may actually be adequate in an urban context like Nairobi. We urge availability studies to take into consideration lead‐times and informal inventory‐pooling networks. Availability at the supplier level or the percentage of client demand met within a specified time frame may be more informative metrics.
Our analysis also suggests that market characteristics partly explain both understocking and overstocking. They also seem to have a substantial negative impact on budget and consequently on service quality. If this is indeed the case, it is a strong argument for rationalizing catchment areas, as also advocated by Abuga et al. (2019). However, competition could also make facilities “listen to their clients” better and lead to improvements in efficiency and quality of their service. Whether and when such benefits outweigh the disadvantages remains a question for future research.
Many organizations aim to achieve UNSDG #3 and related goals by addressing the managerial causes and resource limitations revealed by our analyses: budget, skills, and systems. Future research should try to identify the best ways to mitigate the impact of credit constraints on ordering. Organizations such as the Medical Credit Fund provide small and medium‐sized healthcare providers with fast mobile loans to deal with cash problems or to use for investments (UNSDG #3.8 and #3.C). Groups like mPharma and Shelf Life also provide inventory to the facilities on consignment. The loans alleviate credit constraints while allowing the retailer determine what quantities to order, whereas the consignment facility gives the suppliers more control over order quantities. Which of these approaches is best is a modeling question and also a topic for a future empirical study.
Dozens of pharmaceutical management systems exist, including open source systems, and many organizations offer inventory management training (UNSDG #3.C). We suggest that developing more programs should not be the priority at present. It is more important to investigate what prevents facilities from utilizing their existing systems effectively, as observed in our study. Our workshop, for example, revealed that staff turnover is a key barrier to investing in training of employees. Training was also described as being “too scientific.” Another barrier is that facilities have not seen evidence of a positive return from their investment in IT systems and training. Future research presenting a holistic analysis of such issues is very much needed.
A related open question is whether there is a natural hierarchy of solutions to the six types of issues analyzed here. For instance, is there an optimal order to implementing the solutions? Should one resolve budget, time, and motivation constraints before working on skills and systems? Should one work on developing skills before enhancing systems? Which improvements should be made in parallel as opposed to sequentially? One hypothesis that follows from our observations, for example, is that the impact of system improvement may depend strongly on skills and motivation. Similar to studies on improvements in manufacturing performance (see, e.g., Ferdows and De Meyer 1990, Gardner 2020, Noble 1995, and references within), more empirical research assessing the link between causes and effective use of inventory control would help in determining the optimal sequence of improvement efforts.
We acknowledge that despite our best efforts there are limitations to our study. The descriptive nature of our study allowed us to account for situational complexities and provide deep and rich theoretical descriptions of the phenomena (cf. Gioia et al. 2013). However, the number of observations is too small to study any heterogeneity of the phenomenon across sub‐samples of private healthcare facilities—for instance, we are unable to study if resource limitations are the primary drivers for mismatch in certain facilities and unhealthy levels of competition is the primary cause in others. Furthermore, qualitative research is often thought inappropriate to draw generalizable conclusions on (sub)populations (Creswell 2009). This limitation is also reflected in our sample selection process (see section 4), which was performed “purposively” to achieve information saturation, rather than “randomly” to achieve generalizability. Exploratory studies such as ours lead to hypotheses and propositions, and thereby lay the groundwork for future research. Future empirical research collecting data from a wider range of healthcare facilities and analyzing validity of our results for sub‐samples is needed. We note that this phased approach to research—first perform an exploratory study, then perform confirmatory research—is common and advocated for studying new phenomena (Tukey 1980).
Another limitation is that all the interviews were conducted in Nairobi. Based on the similarity in context and our understanding of the on‐the‐ground realities, we believe that our insights are generalizable to other resource‐constrained settings in LMICs, but this needs to be tested. In particular, field experiments and empirical analyses on data from different LMICs should be conducted to test the causal relationships we proposed in section 6.
We hope that future researchers will build on the propositions that resulted from this analysis, notably by conducting a finer root‐cause analysis of the mismatch between demand and supply in private healthcare facilities, along with an examination of its effect on patients and facilities. Strengthening the private sector will improve the overall healthcare supply chain, foster progress toward universal health coverage and, more generally, the UNSDGs.
Footnotes
The KEML is a list of drugs, drawn up by the Kenyan Ministry of Health, that are “considered to be the most efficacious, safe and cost‐effective for the relevant conditions” and that are “expected to be routinely available in healthcare facilities (at the appropriately designated levels of care)” (Ministry of Health ![]() ).
).
37% of the items stocked by a facility were from the KEML.
The interviewers discussed their observations after each interview and formed a joint judgment.
Though our interviews did not capture these factors systematically, they surfaced regularly. We were able to piece together a framework on the basis of our general understanding of the market structure and regulatory landscape, insights obtained during the interviews, and a dissemination workshop for interviewees held in 2019.
During our interviews, many facilities (51%; 20 out of 39) acknowledged that they face high levels of competition.
During our feedback workshop, 60% of respondents (9 out of 15) agreed with the statement, “There are too many facilities that sell medicines in my area. If there were less competition, I would be able to further professionalize my business."