
Abstract
Commentary
The incidence of PNES is reported to be 1.5 per 100,000 per year that is approximately 4% of the incidence of all epilepsy (1). Yet, PNES accounts for between 25% and 45% of all video-EEG admissions to epilepsy monitoring units (2). In this Benbadis et al. investigation, 22 reviewers analyzed 22 consecutive single events recorded with video-EEG for the purpose of assessing interrater reliability. The reviewers were blinded to a detailed clinical history and other events documented on the patient (3). Although there was substantial concordance for the diagnosis of epilepsy, overall there was actually “low agreement for physiologic nonepileptic events and moderate agreement for psychogenic nonepileptic events.” This study helps to underscore the inherent difficulties associated with the diagnosis of PNES in video-EEG monitoring units based on the evaluation of a single event in isolation. Perhaps, the interrater reliability would have been improved considerably with assessment of multiple events.
Because epilepsy is often diagnosed by a change in the EEG, it was no surprise to find substantial concurrence for an epilepsy diagnosis. There should have been even high interrater reliability, given that there were 22 raters, and if all of the EEG samples had had an unequivocal, easily interpreted change. However, scenarios in which the significance of a video-EEG change may not be readily apparent make correctly diagnosing epilepsy versus PNES difficult. In particular, it can be difficult to discriminate between PNES and simple partial seizures, because only approximately 20% of patients have an EEG accompaniment, and complex partial seizures arise from deep convexities within the frontal lobe, making them difficult to record on scalp electrodes (4).
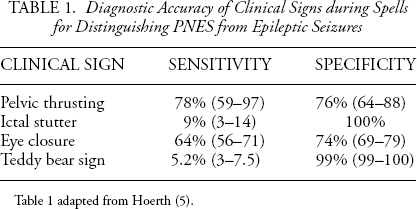
One issue that arises from the study pertains to the identification of the semiologic characteristic of the EEG event that led to each of the reviewers’ diagnosis. Recently, Hoerth and colleagues systematically analyzed clinical signs that may be useful for discriminating between the diagnosis of epilepsy and PNES in video monitoring studies (5). The isolated behaviors they identified included pelvic thrusting, ictal stuttering, ictal eye closure, and the teddy bear sign. Table 1 lists the diagnostic accuracy of these clinical signs. Ictal stuttering and teddy bear sign were often the most significant predictors of psychogenic nonepileptic events. Among the EEG reviewers, those who had a moderate level of interrater reliability for the psychogenic nonepileptic events, perhaps, represent a bias towards analyzing specific semiological component of the clinical signs to inform a particular diagnosis. In contrast, other reviewers may have primarily relied on the clinical gestalt, when other variables such as medical history and heterogeneity of multiple spells, were not available to factor into the diagnosis.
Diagnostic Accuracy of Clinical Signs during Spells for Distinguishing PNES from Epileptic Seizures
Moreover, the low interrater reliability for physiologic nonepileptic events is not surprising, given the authors’ explanation that these events were an infrequent diagnostic category and more importantly, that the physiologic event could have represented a number of other neurologic conditions. Perhaps, a neurologist or other neurological subspecialist, who is accustomed to diagnosing paroxysmal events and has had a significant amount of exposure to diagnosing numerous spells types, could better identify episodes of physiological nonepileptic events that mimick epilepsy (e.g., movement disorders) than could this group of “board-certified neurologists and practicing epileptologists at epilepsy centers.”
In summary, the study by Benbadis et al. is a reminder that there is no one clinical factor, whether video-EEG, history, or an examination, that is going to 100% accurately identify a patient with a given diagnosis. The authors were quite correct in stating that the diagnosis of PNES represents the art of medicine, as different lines of converging evidence need to be assimilated in order to arrive at its correct diagnosis. This study also underscores the fact that video monitoring of a single event cannot be utilized in isolation, without also evaluating the clinical history and other records. Doing so, is akin to judging a book by its cover and not by reading what is inside.
Clearly much more work is needed in order to better standardize video-EEG interpretation and perhaps find better biomarkers to confirm a diagnosis of PNES with high specificity and sensitivity. Benbadis and colleagues have done excellent work in advancing the knowledge of interrater reliability for interpretation of individual nonepileptic events. Consistent use of video-EEG monitoring, along with itemizing the clinical signs that help assess whether an event is epileptic or nonepileptic, may allow for the development of more sophisticated models that accurately represent the true complexity of these events.