
Abstract
A 27-year-old woman was admitted to the Emergency Department with right upper-extremity numbness and mild weakness followed by a bifrontal throbbing headache for 30 min, which was similar to a headache lasting for 12 h that had occurred 3 days ago. Laboratory tests were unremarkable except for cerebrospinal fluid (CSF) lymphocytic pleocytosis. On the following day, a headache episode with left hemiparesis and hemihypoaesthesia, left hemifield visio-spatial inattention, anosagnosia and confusion recurred. The headache was diagnosed as headache and neurological deficits with cerebrospinal fluid lymphocytosis (HaNDL) syndrome according to the criteria of the second edition of the International Classification of Headache Disorders. Simultaneously performed magnetic resonance imaging (MRI) revealed swelling of the grey matter, CSF enhancement in the sulci of the right temporal and occipital regions and hypoperfusion of the same brain regions. During the following 10 days two more similar episodes recurred and during the ensuing 12 months the patient remained headache free. Neuroimaging findings of the HaNDL syndrome are always thought as virtually normal. MRI abnormalities in our patient have not been reported in HaNDL syndrome previously, although they have been reported in hemiplegic migraine patients before. The findings in our case suggest that hemiplegic migraine and HaNDL syndrome may share a common pathophysiological pathway resulting in similar imaging findings and neurological symptoms.
Introduction
Diagnostic criteria for HaNDL according to the International Classification of Headache Disorders, 2nd edn
Here we present a case of a 27-year-old woman who suffered from episodes of headache with transient focal neurological deficits that were consistent with HaNDL and abnormal magnetic resonance imaging (MRI) findings not previously reported in HaNDL syndrome.
Case report
Four days before admission to our emergency department a 27-year-old woman experienced numbness moving from her left hand to the left side of her face in 3–5 min. After the transient neurological symptoms, she developed a bifrontal throbbing headache with nausea, vomiting and photophobia, lasting for 10–12 h. She had no complaints on the following 3 days.
On the day of her admission to our emergency department she experienced a 30-min episode of right upper-extremity numbness and mild weakness followed by a bifrontal throbbing headache with nausea and vomiting. Her neurological examination was unremarkable except for blurring of the temporal margin of the left optic disc, which was later thought to be pseudopapilloedema. She was hospitalized in order to make the differential diagnosis of ongoing intense headache. Brain MRI on admission was unremarkable, but lumbar puncture showed a normal CSF opening pressure and a pleocytosis of 60 cells/mm3 with 99% lymphocytes. CSF protein concentration was slightly elevated at 150 mg/dl and glucose was in normal range. Laboratory studies, including a complete blood count, erythrocyte sedimentation rate, liver and renal function tests, HIV and syphilis serology, prothrombin time, partial thromboplastin time, antinuclear antibody, antineutrophil cytoplasmic autoantibody, brucella agglutination and urine analysis were all unremarkable. The second episode lasted for 5–6 h. Verapamil was started at a dose of 240 mg/day p.o. Her past medical history was unremarkable except for venlafaxine 75 mg/day, which had started 3 months ago for depression; there was no personal or family history of migraine.
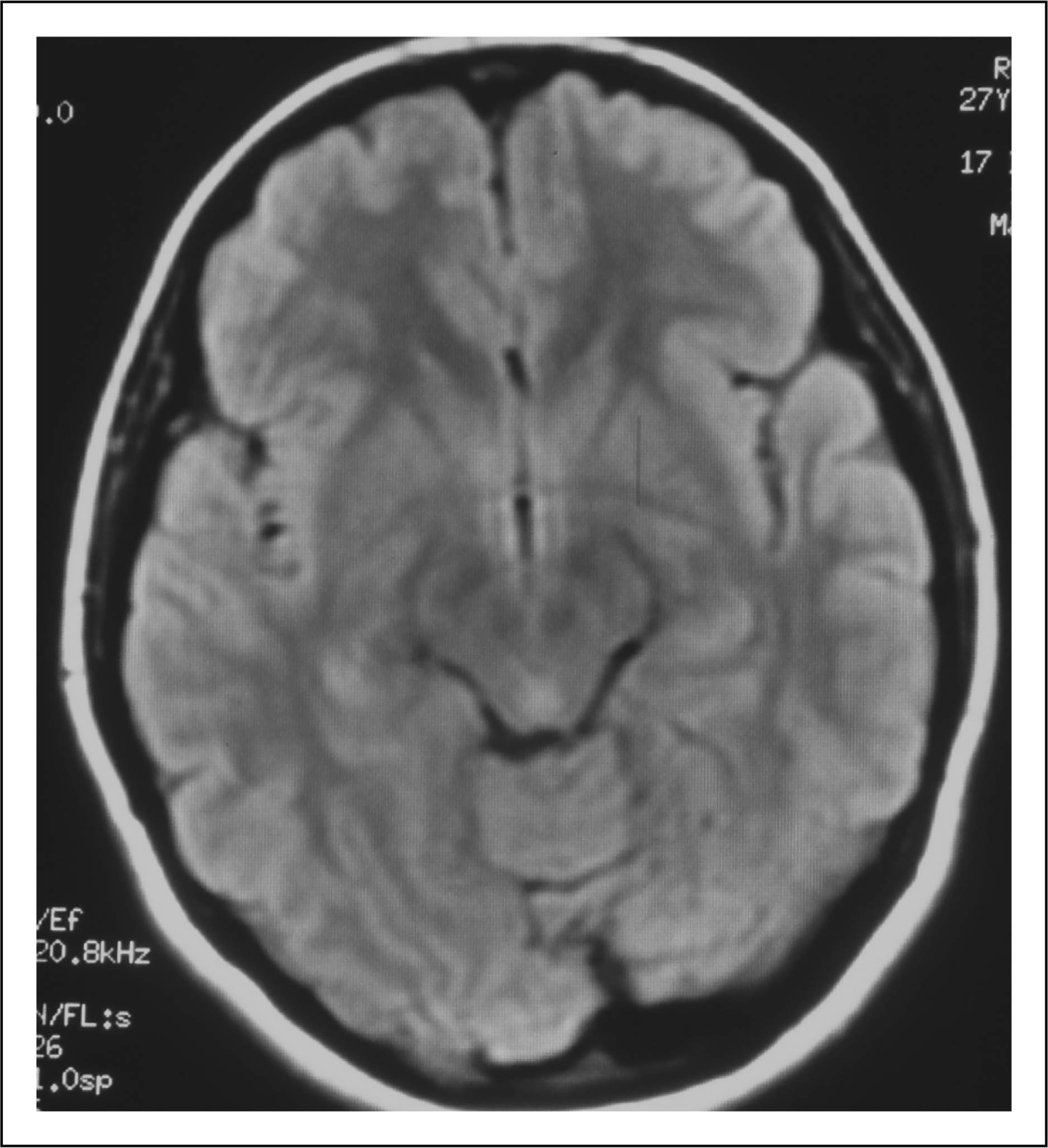
On day 2 of her hospitalization she had an episode of left hemiparesis (Medical Research Council grade 3/5), which was followed by central facial palsy 5 min later. She also had left hemihypoaesthesia, left hemifield visuo-spatial inattention, anosagnosia and confusion. She underwent urgent T1, T2 weighted, fluid attenuated inversion recovery (FLAIR) MRI and MR angiography with diffusion (DWI) and perfusion weighted imaging (PWI). These sequences revealed normal DWI and no large vessel obstruction was observed. However, there was swelling of the grey matter and CSF enhancement in the sulci of the temporal and occipital regions (more pronounced on the right hemisphere) on FLAIR images (Figure 1) and hypoperfusion of the right parieto-occipital regions on PWI (Figure 2).
Fluid attenuated inversion recovery images reveal swelling of the grey matter and cerebrospinal fluid enhancement in the sulci of the temporal and occipital regions, more pronounced on the right hemisphere. Hypoperfusion of the right parieto-occipital regions (at two different levels) on perfusion weighted imaging.

Prednisolone 50 mg/day p.o. and valproic acid 1000 mg/day p.o. were started, the next day she became agitated, prednisolone and venlafaxine were discontinued and risperidone 1 mg/day p.o. was started. In order to exclude an epileptic seizure in the differential diagnosis of prolonged confusional state, an EEG was performed, which showed diffuse slow wave activity (6–7 Hz diffuse θ activity) consistent with her altered mental status. Although photoparoxysmal response was not seen with photic stimulation during EEG, she developed similar attacks with headache and right hemiparesis just after the photic stimulation. The ongoing EEG recordings revealed similar slow wave activity that was not localized in areas consistent with the focal neurological deficits. Her confusional agitated state ended after 2 days, but she then became hypomanic. On the following days she had two more similar attacks of headache and hemiparesis of shorter duration. Her confusional state and hypomanic episodes gradually improved and after 15 days' hospitalization she was discharged under verapamil treatment that was discontinued 3 months later. In the ensuing 12 months she had no further episodes and has remained neurologically normal. Also at the end of 12 months PWI and FLAIR MRI were performed again and showed no pathological findings (Figures 3 and 4).
Perfusion weighted imaging studies at 12 months showed near normal findings. Fluid attenuated inversion recovery images showed resolution of gyral oedema after 12 months.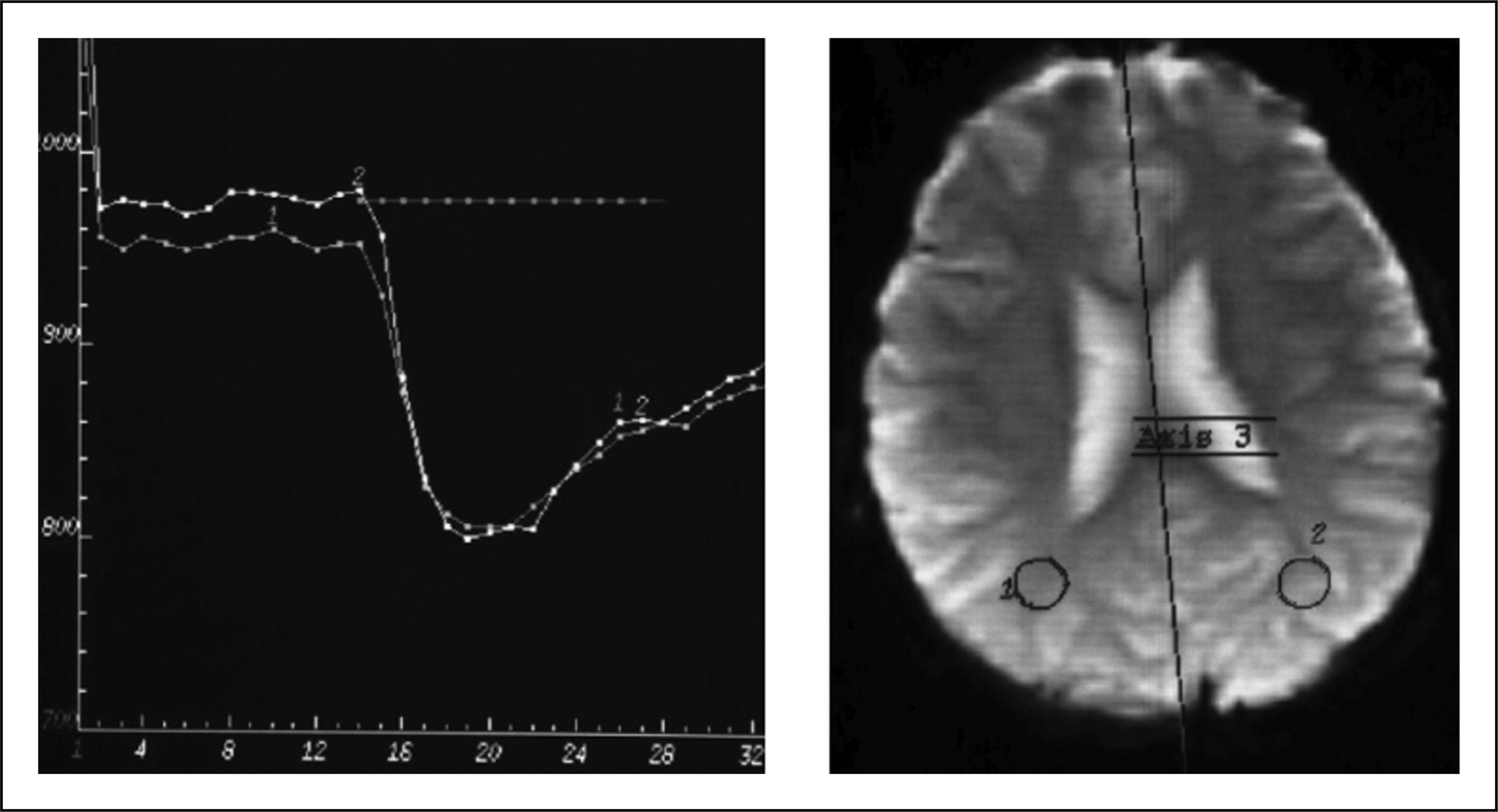
Discussion
Differences between HaNDL syndrome and sporadic hemiplegic migraine (SHM)

The HaNDL syndrome can be differentiated from hemiplegic migraine by abnormal CSF findings (1). Lymphocytic pleocytosis is always present in HaNDL syndrome, and the reported mean lymphocyte count is 199 ± 174/mm3 (2). However, elevated CSF protein levels and pleocytosis have been also reported in both familial and sporadic hemiplegic migraine patients (3). Our case had neither migraine history nor further attacks during a follow-up period of 12 months. For these reasons, the diagnosis of HaNDL syndrome was made, instead of hemiplegic migraine.
Neuroimaging findings of HaNDL syndrome are always thought to be virtually always normal (2). To our knowledge, MRI abnormalities determined in our patient have not been reported before.
The FLAIR MRI images showed swelling of the grey matter and CSF enhancement in the sulci of the right temporal and occipital cortex, suggesting the presence of vasogenic leakage from the leptomeningeal vessels. CSF enhancement in the sulci can be seen in various conditions such as meningitis, brain tumours, status epilepticus and stroke, which are unlikely in our patient. It has also been reported in migraine and hemiplegic migraine patients, although never in HaNDL syndrome (4,5). Regional cerebrovascular reactivity under the influence of trigeminovascular activation may be the cause of these MRI findings, including swelling of the grey matter and CSF enhancement in the sulci of the right temporal and occipital cortex.
The imaging was performed approximately 30 min after the onset of neurological symptoms. Focal hypoperfusion was detected in the brain regions corresponding to focal neurological deficits. This finding has also not been reported before in HaNDL syndrome, but has been reported in SHM patients (6–8).
Hemispheric hyperperfusion during a hemiplegic migraine attack, correlating with contralateral hemiplegia, has also been previously reported (6). Hyperperfusion was not demonstrated in our patient, and this may be explained by the timing of the scanning.
Both vasogenic leakage and hypoperfused brain regions were seen at similar brain regions (posterior parts) corresponding to the neurological deficits. It is thought that hypoperfusion might be secondary to hypometabolism of the neurons at the involved areas.
Single photon emission computed tomography images of HaNDL patients have revealed a decrease of radionuclide uptake over the cortical region corresponding to neurological deficits during acute phase (9). Arteriolar vasomotor changes during attacks have also been shown in HaNDL patients by transcranial Doppler sonography (10). Cranial angiography of another previously reported HaNDL patient revealed local inflammation of the arterial wall corresponding to the neurological symptoms, and two small left parietal infarcts have been shown on follow-up MRI (11). All these reported findings may be the indicators of cerebral perfusion abnormalities in HaNDL patients.
The HaNDL syndrome is a benign, self-limiting disease and its pathophysiology is still unclear. Probably due to a reason that has not yet been determined, lymphocytic pleocytosis, recurrent migraine-like headaches and cortical spreading depression occur in a limited period of time, usually once during life. In a recent study, abnormal autoimmune reactivity was shown against central nervous system neurons, supporting the autoimmune hypothesis as a pathogenic factor for HaNDL syndrome (12). This may be the reason for the CSF pleocytosis observed in HaNDL syndrome.
Posterior leukoencephalopathy syndrome (PLES) might be kept in mind in the differential diagnosis of any patient with symptoms such as headache, seizures, visual disturbances, altered mental status and hypertension, but the characteristic MRI findings, hypertension or any of the precipitating factors for PLES (sepsis, electrolyte imbalance, chemotheraphy, etc.) were not observed in our patient.
In conclusion, SHM, FHM and HaNDL syndrome have different underlying mechanisms, but the findings in our case suggest that they may share a common pathophysiological pathway resulting in similar imaging findings and neurological symptoms. According to the current diagnostic criteria, it is not easy to differentiate HaNDL syndrome from sporadic hemiplegic migraine patients.