
Abstract
Reversible cerebral vasoconstriction syndrome (RCVS) diagnosis is based on the association of thunderclap headache (TH) and multiple vasoconstriction of intracranial arteries, which disappear in the following 3 months (1, 2). The clinical course, usually benign, may be complicated in 25% of cases by ischaemic stroke, intracerebral or subarachnoid haemorrhage (SAH), which impose withdrawal of the precipitating factor when possible (1). A precipitating factor, like postpartum or exposure to various vasoactive substances, is associated with RCVS in two-thirds of cases, defining a secondary RCVS (1). Identifying potential precipitating factors is thus crucial in order to withdraw them, particularly when medication is suspected. We report a patient who suffered from a RCVS with SAH as she was treated with pegylated interferon-alfa-2a and darbepoetin-alfa for chronic hepatitis C.
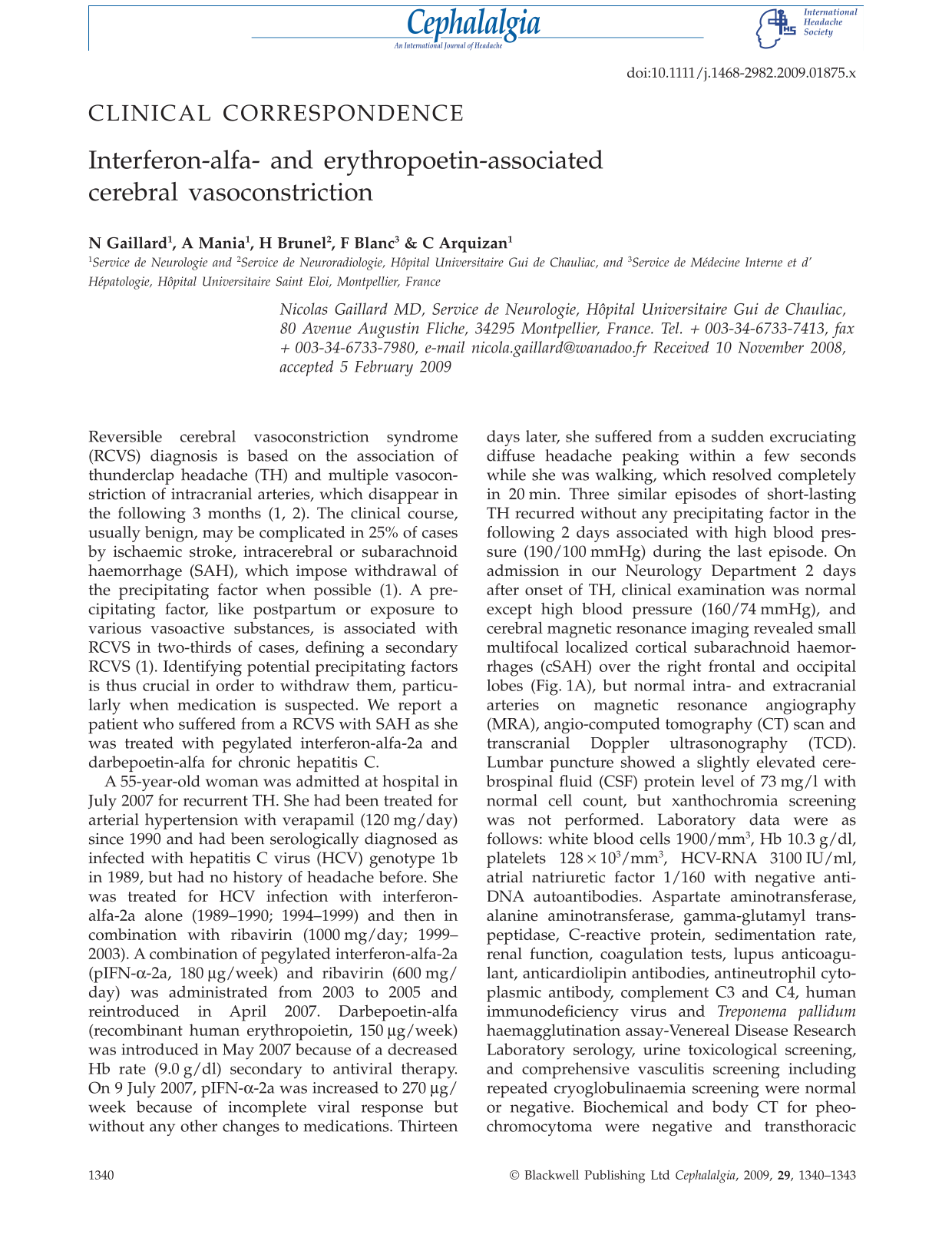
A 55-year-old woman was admitted at hospital in July 2007 for recurrent TH. She had been treated for arterial hypertension with verapamil (120 mg/day) since 1990 and had been serologically diagnosed as infected with hepatitis C virus (HCV) genotype 1b in 1989, but had no history of headache before. She was treated for HCV infection with interferon-alfa-2a alone (1989–1990; 1994–1999) and then in combination with ribavirin (1000 mg/day; 1999–2003). A combination of pegylated interferon-alfa-2a (pIFN-α-2a, 180 µg/week) and ribavirin (600 mg/day) was administrated from 2003 to 2005 and reintroduced in April 2007. Darbepoetin-alfa (recombinant human erythropoietin, 150 µg/week) was introduced in May 2007 because of a decreased Hb rate (9.0 g/dl) secondary to antiviral therapy. On 9 July 2007, pIFN-α-2a was increased to 270 µg/week because of incomplete viral response but without any other changes to medications. Thirteen days later, she suffered from a sudden excruciating diffuse headache peaking within a few seconds while she was walking, which resolved completely in 20 min. Three similar episodes of short-lasting TH recurred without any precipitating factor in the following 2 days associated with high blood pressure (190/100 mmHg) during the last episode. On admission in our Neurology Department 2 days after onset of TH, clinical examination was normal except high blood pressure (160/74 mmHg), and cerebral magnetic resonance imaging revealed small multifocal localized cortical subarachnoid haemorrhages (cSAH) over the right frontal and occipital lobes (Fig. 1A), but normal intra- and extracranial arteries on magnetic resonance angiography (MRA), angio-computed tomography (CT) scan and transcranial Doppler ultrasonography (TCD). Lumbar puncture showed a slightly elevated cerebrospinal fluid (CSF) protein level of 73 mg/l with normal cell count, but xanthochromia screening was not performed. Laboratory data were as follows: white blood cells 1900/mm3, Hb 10.3 g/dl, platelets 128 × 103/mm3, HCV-RNA 3100 IU/ml, atrial natriuretic factor 1/160 with negative anti-DNA autoantibodies. Aspartate aminotransferase, alanine aminotransferase, gamma-glutamyl transpeptidase, C-reactive protein, sedimentation rate, renal function, coagulation tests, lupus anticoagulant, anticardiolipin antibodies, antineutrophil cytoplasmic antibody, complement C3 and C4, human immunodeficiency virus and Treponema pallidum haemagglutination assay-Venereal Disease Research Laboratory serology, urine toxicological screening, and comprehensive vasculitis screening including repeated cryoglobulinaemia screening were normal or negative. Biochemical and body CT for pheochromocytoma were negative and transthoracic echocardiography was normal. Digital cerebral angiography (CA) 1 day after admission revealed multifocal segmental arterial narrowings involving distal middle-sized arteries in both left and right anterior circulations, but no aneurysms (Fig. 1B1). pIFN-α-2a and darbepoetin-alfa were stopped, verapamil was sustained in association with oral nimodipine for a total of 4 weeks and treatment with high-dose intravenous corticosteroid for 5 days was initiated on the hypothesis of cerebral angiitis. Blood pressure normalized from the second day of care. CA was normal with complete resolution of arterial vasoconstriction (Fig. 1B2) 4 months later. Clinical course was also favourable with no recurrence of headache or other symptoms after 12 months' follow-up, with no need for other antihypertensive medication, and hepatitis C was successfully treated with ribavirin alone.

Axial gradient echo T2-weighted and fluid-attenuated inversion recovery magnetic resonance images showing multifocal localized cortical subarachnoid haemorrhages over the right frontal and occipital lobes (A). Digital cerebral angiography reveals diffuse multifocal segmental vasoconstriction in the right middle cerebral artery (B1) with normalization 4 months later (B2).
Discussion
To our knowledge, this is the first case of RCVS associated with the use of erythropoetin (EPO) and IFN-α therapies. RCVS is a rare but increasingly recognized aetiology of TH, particularly when TH recurs over a few days (1, 2). Diagnosis is based on the association of TH and multiple vasoconstriction of intracranial medium and/or large size arteries on angiographic investigations, which disappear in the following 3 months, criteria fulfilled in this case report. Non-invasive cerebral arterial imaging can fail to demonstrate multiple vasoconstriction, as seen in our case, in around 20% of cases for the first MRA and 30% for TCD, particularly when performed early during the course of RCVS, because of the lack of sensitivity of both angioCT, MRA and TCD compared with CA to explore distal medium-sized arteries, which are presumed to be first involved during RCVS pathophysiology (1). In the series of Ducros et al. (1), MRA sensitivity increased from 79 to 88% when repeated after a mean of 5.7 days, but 9% of patients had both normal MRA and TCD, like our patient, whereas CA sensitivity was 100%. Because the best timing and angiographic imaging strategy for RCVS diagnosis remains unclear, CA should still be considered in early management when first-line non-invasive cerebral arterial imaging is normal and angiitis is clinically plausible, or when the clinical course is worsening or complicated. The two main differential diagnoses in the acute phase are cerebral angiitis and ruptured aneurysm, particularly when RCVS is complicated by stroke or SAH, which occurs in around 25% of cases (1). Aneurysmal SAH vasospasm was not plausible because it usually correlates with the location and amount of bleeding, is not multifocal, is delayed from SAH onset and CA ruled out an aneurysm in our patient. In contrast, central nervous system angiitis (CNSA) was initially considered because of concomitant active HCV hepatitis, but the lack of peripheral nervous system or multisystemic involvement and normal parenchymal brain and biological parameters, except slightly elevated CSF protein level, were not suggestive of this diagnosis. CSF analysis in our patient may reflect blood–brain barrier disruption associated with SAH and is consistent with the Ducros et al. series (1), where more than one-third of patients had elevated CSF protein levels ranging from 0.48 to 0.90 mg/l. A few cases of CNSA associated with HCV have been reported, secondary to cryoglobulinaemia syndrome or polyarteritis nodosa systemic vasculitis (3–5). Those patients presented a severe stroke or encephalopathy with brain parenchymal abnormalities on imaging, or preferentially peripheral nervous system and/or systemic involvement (3–5). One case of isolated central nervous system granulomatous angiitis was reported in a patient with brain haemorrhage revealing hepatitis C, but investigations for secondary CNSA were not exhaustive (5). In contrast, the benign and fully regressive clinical and angiographic course of our patient after a short acute phase, without any recurrence or other symptoms and without any immunotherapy, even if she received short intravenous corticosteroid, confirmed the hypothesis of a RCVS. Medical therapy for RCVS remains largely empirical, and arterial vasodilator medications, such as nimodipine, are usually considered. We usually give nimodipine for 4 weeks to our RCVS patients because TH, ischaemic and haemorrhagic complications seem not to occur more than 28 days after TH onset during RCVS course, although vasoconstriction may persist longer (1). Corticosteroid therapy in RCVS should be avoided according to some authors (1), but may appear useful for others (2), and was given to our patient because CNSA could not be excluded within the first days of the acute phase.
A precipitating factor, often exposure to one or several vasoactive substances, is associated with RCVS in two-thirds of cases defining a secondary RCVS (1, 2). Our patient was exposed to two vasoactive medications, EPO and IFN-α, which were definitively stopped after diagnosis of RCVS. EPO, which may favour arterial hypertension, peripheral arterial vasoconstriction, venous and arterial thrombosis risk (6), has been identified as a potential precipitating factor of RCVS (1, 2). EPO may have contributed to RCVS in our patient through several synergistic mechanisms, leading to cerebral vasoconstriction including worsening of pre-existing hypertension, haematocrit-dependent peripheral vascular resistance increase and platelet activation (6). However, EPO may also augment nitric oxide-related endothelial vasodilation in experimental models of SAH, which could in theory prevent or limit cerebral vasoconstriction, but data on man are missing (7). RCVS physiopathology, which remains unclear, is characterized by acute alteration in arterial tone, with association of constriction and dilation (2), leaving speculation on the initial triggering mechanism on vascular tone. Interestingly, EPO, like postpartum, is also recognized as a precipitating factor of reversible posterior leucoencephalopathy syndrome (RPLS), which is sometimes associated with RCVS, suggesting a physiopathological link between these two overlapping syndromes, as a possible acute dysregulation of intracranial arterial vasoregulation related to drug-induced endothelial dysfunction (1, 2, 6, 8–10). IFN-α has been recently identified as a new precipitating factor for RCVS in two patients, in association with another vasoactive substance (cannabis and selective serotonin reuptake inhibitor) in one case (1), and has also been reported to be associated with RPLS in one case (8). Our case thus contributes to increasing evidence that IFN-α may precipitate a RCVS. We report the first case of RCVS associated with IFN-α complicated with cSAH. One of the two patients reported by Ducros et al. (1) with RCVS associated with IFN-α had intracerebral haemorrhage (ICH). Furthermore, it is of interest that four cases of ICH under pIFN-α-2b therapy for hepatitis C have been reported, allowing speculation on a possible increased risk of intracranial haemorrhage related to IFN-α therapy (11). In our patient, an increase in dose regimen of IFN-α about 2 weeks before RCVS may indicate a possible dose–effect in the physiopathological mechanism. Supporting a hypothetical link between IFN-α and acute arterial vasoconstriction, IFN-α is suspected to cause sympathic nerve activation with tachycardia and arterial hypertension, cardiotoxicity related to cases of acute coronary syndrome and cardiomyopathy with possible coronary spasm, and to decrease endothelium-dependent vasodilation (12, 13). We therefore may speculate on an additive or synergic vasoactive effect of pIFN-α-2a and darbepoetin-alfa on cerebral autoregulation and systemic blood pressure which led to RCVS in our patient, in spite of verapamil therapy, a calcium-channel blocker inducing vasodilation, used by some as a first-line therapy in RCVS (2). However, medications such as EPO and IFN-α are more likely to precipitate rather than to cause RCVS, which may occur without any precipitating factor in up to one-third of cases (1). If early withdrawal of such precipitating medications could prevent delayed complications such as ischaemic stroke or haemorrage is ignored since vasoconstriction has a different course from clinical manifestations, worsening for several weeks after the onset of TH. In spite of that, one should stop early and definitively precipitating factors when possible in order to avoid any recurrence of RCVS. (1, 2).
In conclusion, this case contributes to widen the spectrum of unusual vasoactive therapies like IFN-α and EPO as precipitating factors of RCVS and to underline difficulties in early diagnosis management.
Competing interests
None to declare.