
Abstract
Understanding the patterns of acute treatment of migraine in the population is a necessary step in evaluating treatment in relation to guidelines, and in improving care. Herein we assess the specific medication used for the acute treatment of migraine and chronic migraine (CM) in the population. We identified 24 000 headache sufferers, drawn from over 165 000 individuals representative of the US population. This sample has been followed with annual surveys using validated questionnaires. As part of the survey, subjects were asked to report the specific medications currently used for their most severe headaches, dose, and number of days per month using medication. Complete responses were obtained from 14 540 individuals, including 9128 with episodic migraine and 503 with CM. For episodic migraine, specific treatment was used by 19.2% of subjects (triptans 18.7%; compounds with ergotamine 0.5%). A total of 11.1% routinely used opiates, whereas 6% used compounds with barbiturates. For CM, 22% used migraine-specific treatment, whereas 34.3% used opiates and barbiturates. Non-prescribed medications were frequently used in both groups. Opiates were more commonly used by those with CM [odds ratio (OR) 2.12, 95% confidence interval (CI) 1.69, 2.65], as were butalbital-containing compounds (OR 2.46, 95% CI 1.88, 3.22). The minority of migraineurs in the USA use specific medication, and one-fifth use opiates or barbiturates. For CM, > 34% use opiates or barbiturates. Accordingly, a sizable proportion use medications that are not firstline according to the US Headache Consortium Guidelines.
Introduction
Migraine is a common neurological disorder, affecting 18% of women and 6% of men in the USA (1, 2). Although the frequency and severity of migraine vary considerably, over half of migraineurs report substantial impairment in daily activities, or require bed rest during their severe headaches, and almost one-third report missing at least 1 day of work or school in the last 3 months due to migraine (2–5). In addition, episodic migraine sometimes evolves to chronic migraine (CM) (6, 7). Both migraine and CM are associated with a profound impact on individuals, their families and society (8).
Although severe and disabling, migraine remains unrecognized, underdiagnosed and undertreated in the USA. Previous studies have shown that only 56% of individuals with migraine were aware of their diagnosis (1, 2). Furthermore, nearly half of migraineurs in the population use exclusively over-the-counter (OTC) medications for treatment of acute attacks (4). Although nearly one-third would require preventive medication according to standard guidelines, only 12% use it (2).
Evaluating patterns of acute migraine treatment in the population is the first step towards assessing the quality of migraine care. Prior studies have shown that > 95% of migraine sufferers use acute treatment, although just a minority use specific agents, and that the overall level of satisfaction with acute treatment is low (1, 2).
In this study we used the enormous database from the American Migraine Prevalence and Prevention study (AMPP) to assess patterns of acute treatment for both episodic and chronic migraine. In the AMPP we screened 120 000 households (2004) and established a cohort of headache sufferers to be followed over five annual waves of survey. Here we present the most recent analysed data from the 2006 interviews. We emphasize that this study reflects the treatment used by migraine sufferers from the US population, and does not reflect the situation in other countries.
Methods
Study population
The AMPP is a longitudinal study following a cohort of severe headache sufferers selected from a representative sample of the general population, modelled on the methods of the American Migraine Study 1 and 2 (1). Details of the AMPP have been described elsewhere (2, 4). In brief, in 2004 we mailed a validated self-administered headache questionnaire to a stratified random sample of 120 000 US households, selected from a 600 000-household nationwide panel maintained by the National Family Opinion. From 30 721 headache sufferers identified, we randomly established a cohort of 24 000. They were classified as having migraine, probable migraine (PM), severe episodic tension-type headache (S-ETTH), CM, and other chronic daily headache (O-CDH). Migraine, PM and S-ETTH were classified according to the Second Edition of the International Classification of Headache Disorders (ICHD-II) (6). CM was classified in those with headaches on > 15 days per month and migraine headaches on most of the headache days. Although this definition is not identical to the ICHD-II definition, the sensitivity and specificity are high (see below).
Subjects are being followed with annual surveys that started in July 2005. Here we report the data from the second wave of follow-up, conducted in 2006.
Survey
Each household member reported by the head of the household to suffer from at least occasional self-defined severe headaches was asked to complete an 82-item survey assessing headache features, disability, patterns of treatment, health-related quality of life, comorbidities, etc. (4, 9). The headache module of our survey has a sensitivity of 100% and specificity of 82.3% for the diagnosis of migraine (1), and a sensitivity of 93% and specificity of 85% for the diagnosis of CM (10).
As a part of the survey, subjects were asked a series of questions regarding acute and preventive treatment. Individuals who experienced multiple headache types were asked to report the types of treatment currently used for their most severe headache pain, the specific medications currently used to treat their headaches, and the number of days per month they use the medications. Specific medications inquired about included the seven triptans in their different formulations (oral, nasal and injections), two ergots, seven non-steroidal anti-inflammatory drugs (NSAIDs), nine OTC medications, eight opioids, two butalbital-containing compounds, and isometheptene compounds. Subjects were given an opportunity to write the name of medications not specifically asked. Subjects were oriented to give information on all medications commonly used to treat their headaches.
Data analysis
Data were summarized using frequency counts and descriptive statistics. Patterns of acute treatment were dichotomized into migraine specific and non-migraine specific, and by category of the particular drug (OTCs, NSAIDs, barbiturates, opioids, isometheptene-containing compounds, triptans and ergots). Odds ratios (ORs) were calculated to assess medication use among participants reporting episodic migraine vs. CM. Ninety-five per cent confidence intervals (CIs) are provided for all ORs. All CIs not containing the value 1 indicate a statistically significant predictor, with a P-value of < 0.05.
The study was approved by the Albert Einstein College of Medicine Investigation Review Board.
Results
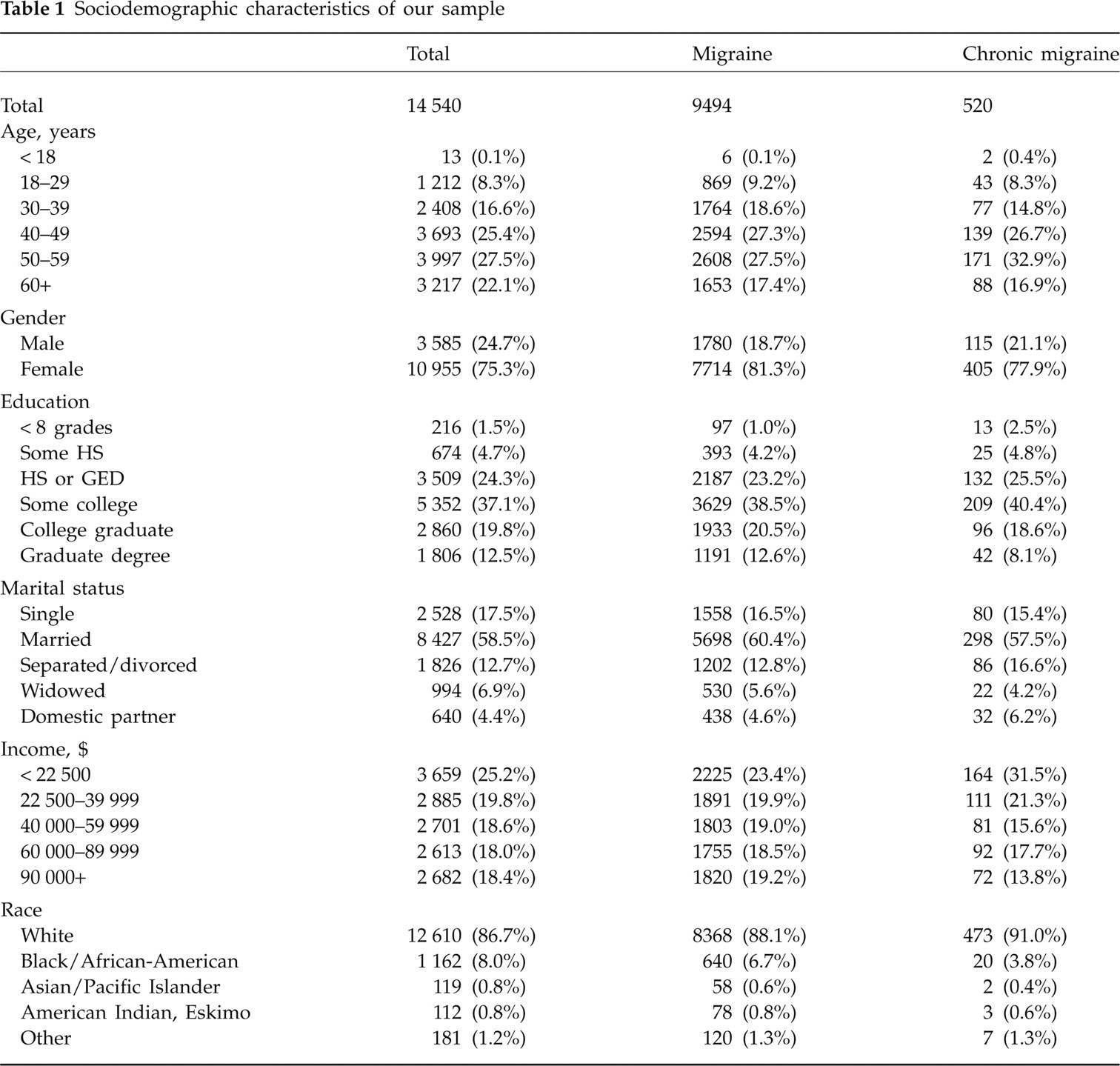
Of 24 000 individuals surveyed in 2004, 16 573 returned complete questionnaires (69.0% response rate) and were re-surveyed in 2006. We obtained 14 540 complete responses (61% response rate regarding the first survey). During that year, 13 638 respondents (94.0%) suffered from at least one headache. A total of 9694 had episodic migraines, and 520 had CM. Of them, 9241 individuals with episodic migraine and 503 with CM used acute treatment. Women comprised 81.3% of episodic and 77.9% of CM sufferers. The majority of respondents with episodic migraine and CM were White (88.1 and 91.0%, respectively), and > 30 years old (90.8 and 91.3%, respectively). Over 71% of episodic and 67% of CM individuals had at least some college education (Table 1).
Sociodemographic characteristics of our sample
Patterns of acute treatment among episodic migraineurs
Prescription medications
Among individuals with episodic migraine, specific treatment was routinely used by 19.3%, with 18.7%% using triptans and 0.6% using ergots (Table 2). Among those using triptans, 85% used exclusively oral forms, and 15% used nasal or subcutaneous routes of administration. The mean number of days of triptan use was 5.7 days. Sumatriptan (54.4%) was the most frequently prescribed migraine-specific medication, followed by rizatriptan (14.9%) and zolmitriptan (12.0%).
Types and frequency of use of acute treatment by migraineurs in the US population in 2006

OTC, over-the-counter; NSAID, non-steroidal anti-inflammatory drugs.
Among non-specific prescribed medications, opioids were routinely used by 11.1%. Oral narcotics containing codeine were the most commonly prescribed, accounting for 74.5% of opiate prescriptions for episodic migraine. Episodic migraine sufferers used opiates on 9.7 days per month, on average.
Butalbital-containing compounds were used by 6% of episodic migraine sufferers for an average of 7.3 days per month. Compounds containing isometheptene were less frequently used (2.8%).
Non-prescription medications
OTC medications containing more than one substance were used by 68% of the migraineurs. NSAIDs were used by 50.4%. Among the NSAIDs, ibuprofen was the most common (47.0% of all NSAIDs), followed by naproxen (29.6%) and aspirin (19.0%). Paracetamol was used by 51.3% of subjects reporting routine use of OTC.
Patterns of acute treatment for CM
Migraine-specific treatments were used by 22% of respondents with CM (Table 3). Over 97% of migraine-specific prescriptions were triptans, mostly oral (83.0%). Sumatriptan (49.7%), zolmitriptan (13.4%) and rizatriptan (11.4%) were the most commonly prescribed triptans for CM.
Types and frequency of use of acute treatment by individuals with chronic migraine in the US population in 2006

OTC, over-the-counter; NSAID, non-steroidal anti-inflammatory drug.
Opioids were frequently used (20.8% of individuals, mean of 18.1 days per month). Butalbital-containing compounds were used by 13.5% of the sample (mean = 15.69 days per month), and compounds containing isometheptene were used by 3.3%.
OTC medications were used by 82.6% of respondents with CM (mean = 15.9 days per month). Combinations were used by 62.8%, whereas paracetamol was used by 45.3%. NSAIDs were used by 43.1% of the sample, with ibuprofen (45.2% of NSAID use), naproxen (26.2%) and aspirin (23.6%) being the most common. Chronic migraineurs used NSAIDs an average of 14.8 days per month.
Differences in the acute treatment of episodic and chronic migraine
Several differences were seen between the acute treatment of CM and that of episodic migraine in the population. Barbiturates were more commonly used by those with CM (crude OR 2.46, 95% CI 1.9, 3.2), as were opioids (OR 2.1, 95% CI 1.9, 2.6). Triptan use was non-significantly increased in CM (OR 1.22. 95% CI 0.98, 1.51) (Table 4).
Odds ratios of medication usage among chronic migraineurs vs. episodic migraineurs

OTC, over-the-counter; NSAID, non-steroidal anti-inflammatory drug.
NSAIDs and combination of OTCs were less frequently used by those with CM than by migraineurs (Table 4).
Discussion
The epidemiology of migraine and CM has been extensively studied. In the USA, migraine affects 12%, whereas CM affects around 2% of the population (3). Migraine and CM impose an enormous burden on sufferers, their family, and on society (11–13).
Prior studies generated from the AMPP study have shown that although almost all migraine sufferers in the USA treat their migraine attacks with medications, just 20% use prescription medications to treat most of the attacks (3). Patterns of acute treatment for CM in the population are not well characterized.
Here, we have reported on the acute medications commonly used to treat episodic migraine and CM in the USA. We found that nearly one-quarter of episodic and one-third of chronic migraineurs routinely use migraine-specific treatment. Together, opioids and barbiturates are almost as frequently used for episodic migraine as triptans (17 and 19%, respectively) and are more frequently used than triptans in CM (34% vs. 21%, P < 0.01). We emphasize, however, that most individuals using narcotics used medications containing codeine, not meperidine-like medications. OTC medications are frequently used for both conditions.
Data from epidemiological studies conducted in other countries help to put our findings in context. As a part of the FRAMIG study, a French population-based study assessing adequacy of care and satisfaction with treatment, 1299 episodic migraineurs provided data on their acute care treatment (14). Of these, 38.6% had used a medication recommended by the French regulatory authorities (triptans, ergotamine, aspirin alone or combined with metoclopramide, other NSAIDs). Even though the recommended medications in French include non-specific drugs, the majority did not use any of these recommended strategies.
Similarly, in a population study in Italy, of 224 065 residents 0.55% received at least one prescription of triptans in 1 year. Assuming that the prevalence of migraine was 10%, just 5% of them received triptans, which, according to the authors, suggested suboptimal treatment of migraine (15). Finally, in South America, specific migraine medication was used by only 23% of migraineurs in the population, even though ergotamine compounds are easily accessible (16).
Although our study was not designed to assess adequacy of care, the use of opioids and barbiturates seemed to be disproportionately high. These classes of medications are not recommended by the US Headache Consortium Guideline as first choices for migraine treatment (17). Furthermore, both classes have been suggested to be associated with the development of CM (18, 19). Research conducted by the National Institute of Drug abuse suggests that overuse of medications reached alarming levels for certain agents, especially opioid analgesics and stimulants, and that future research should focus on the identification of clinical practices aiming at treatment of pain that minimizes the risks of addiction or overuse, the development of guidelines for early detection and management of addiction, and the development of clinically effective agents that minimize the risks for abuse (20). Additionally, in the 20 years since analgesic overuse headache was widely recognized, butalbital overuse has remained distressingly common (21). Herein, opioids and barbiturates were used more frequently in CM than in episodic migraine. From cross-sectional data we cannot determine if use of opioids and barbiturates increases the risk of developing or maintaining CM, or if their use arises as a consequence of severe and accelerating headaches. We plan to investigate these issues in longitudinal data.
Our study has limitations. First, we used a validated questionnaire to diagnose migraine and CM just in those with self-defined severe headaches. Since migraine attacks do not have to be severe, our results do not represent a milder spectrum of migraine excluded from our study. We believe we did not exclude a large group, since our estimates on migraine prevalence overall and by age, sex and disability profiles were very similar to other studies that did not select for severe headaches (22, 23). We conclude that substantial under-ascertainment is unlikely. Second, selection bias, whereby individuals with a physician diagnosis of migraine may have been more likely than undiagnosed migraineurs to respond to the survey, might have led to overestimation of the values for some study parameters. Third, information on medication use was self-reported. Finally, according to the ICHD-II, individuals using 10 (or 15 depending on the class of medication) days of acute treatment have medication overuse headache, not CM (6). Since our objective was to describe patterns of medication use, we described individuals as CM even if they met criteria for medication overuse headache. This facilitates the evaluation of the data from a descriptive aspect, but it should be noted that it does not strictly mimic the ICHD-II recommendation for classification. Strengths of this study include the large sample size, and the meticulous collection of information on acute medication use, including OTCs, from a carefully designed population sample.
The minority of migraineurs and individuals with CM in the USA use specific medication, and a sizable proportion use medications that are not first line according to the US Headache Consortium Guidelines. Although studies that correlate the patterns of preventive medication use with expert recommendation are available, similar studies should also be conducted for acute care, as a prelude to the development of healthcare policies.
Footnotes
Acknowledgements
This study was sponsored by the National Headache Foundation through a grant from Ortho-McNeil Neurologics, Inc. M.E.B. is an employee of Merck Research Laboratories.