
Abstract

Typical aura with migraine headache occurs in approximately one-third of migraineurs and consists of transient and focal neurological symptoms and/or signs that usually occur just prior to or at the onset of migraine headache. The aura is visual in > 90% of patients and can be distinguished from transient cerebral ischaemic attack and ocular pathology by the gradual expansion and evolution of the visual illusion over at least 5 min, and its complete resolution within 60 min (1).
We report a patient with an established history of migraine with aura who presented with her typical migraine headache but an atypical (acute and prolonged at 1 h) presentation of her aura. Severe visual deterioration finally led to a diagnosis of acute multifocal posterior placoid pigment epitheliopathy (AMPPPE) and appropriate vision sparing therapy was initiated. This case illustrates the importance of careful evaluation of the patient who presents with abrupt and/or prolonged aura, especially in those with established migraine with aura, and raises the awareness of AMPPPE and its potential to closely mimic migraine with aura.
Case report
A 37-year-old White woman with a 24-year history of typical aura (visual) with migraine headache developed what she considered to be a typical visual aura of flashing bright lights in both visual fields with an associated headache. She presented to medical attention 3 days later because the visual symptoms persisted—in the past, the aura had never lasted > 60 min.
In addition, she also reported that this particular aura was atypical in that it was isolated to the central visual field of her right eye and consisted of a bright yellow/green light. While the headache persisted, it was mild, not disabling, and according to the patient was not the reason she sought medical attention. Past medical history was remarkable for a recent upper respiratory tract infection and a longstanding history of bipolar disorder, chronic neck pain, and cervical radicular pain. Family history was notable for migraine headaches in her mother and migraines with aura in her sister. Medications included lamotrigine 50 mg twice daily and gabapentin 300 mg three times daily. Initial general medical and neurological examination was normal, including visual fields and ocular motility. Visual acuity corrected was 20/20 OS and 20/25 OD.
Brain magnetic resonance imaging without gadolinium, including diffusion-weighted images, was obtained and interpreted to be normal. Based on her presentation, a presumptive diagnosis of probable migraine with aura according to the criteria of the International Classification of Headache Disorders, 2nd edn (ICHD-II) was made and she was treated unsuccessfully with the following medications in sequential fashion in an attempt to terminate the aura; magnesium sulphate 1 g i.v., Compazine 10 mg i.v. Two days after hospital discharge (8 days after symptom onset) the symptoms persisted, her visual acuity was decreasing, and she was referred to ophthalmology. Eye examination revealed severely impaired visual acuity OD (20/400) and retinal oedema. She was subsequently seen by a retina specialist, who found evidence of choroidal neovascularization OD with a centrocecal scotoma (Fig. 1). The patient was diagnosed with AMPPPE and treated with one intravitreal injection (3.2 mm retrolimbus injection into the intravitreous cavity) of Avastin [(bevacizumab) 1.25 mg (0.05 ml) for concentration of 25 mg/ml]. On follow-up retinal examination 10 days later, early retinal pigment changes, consistent with AMPPPE, were seen (Figs 2–4). OCT testing done on her initial retinal examination and on her subsequent examination 10 days later were both considered normal (Figs 5 and 6).

Amsler grid with a centrocecal scotoma of the right eye as drawn by the patient.
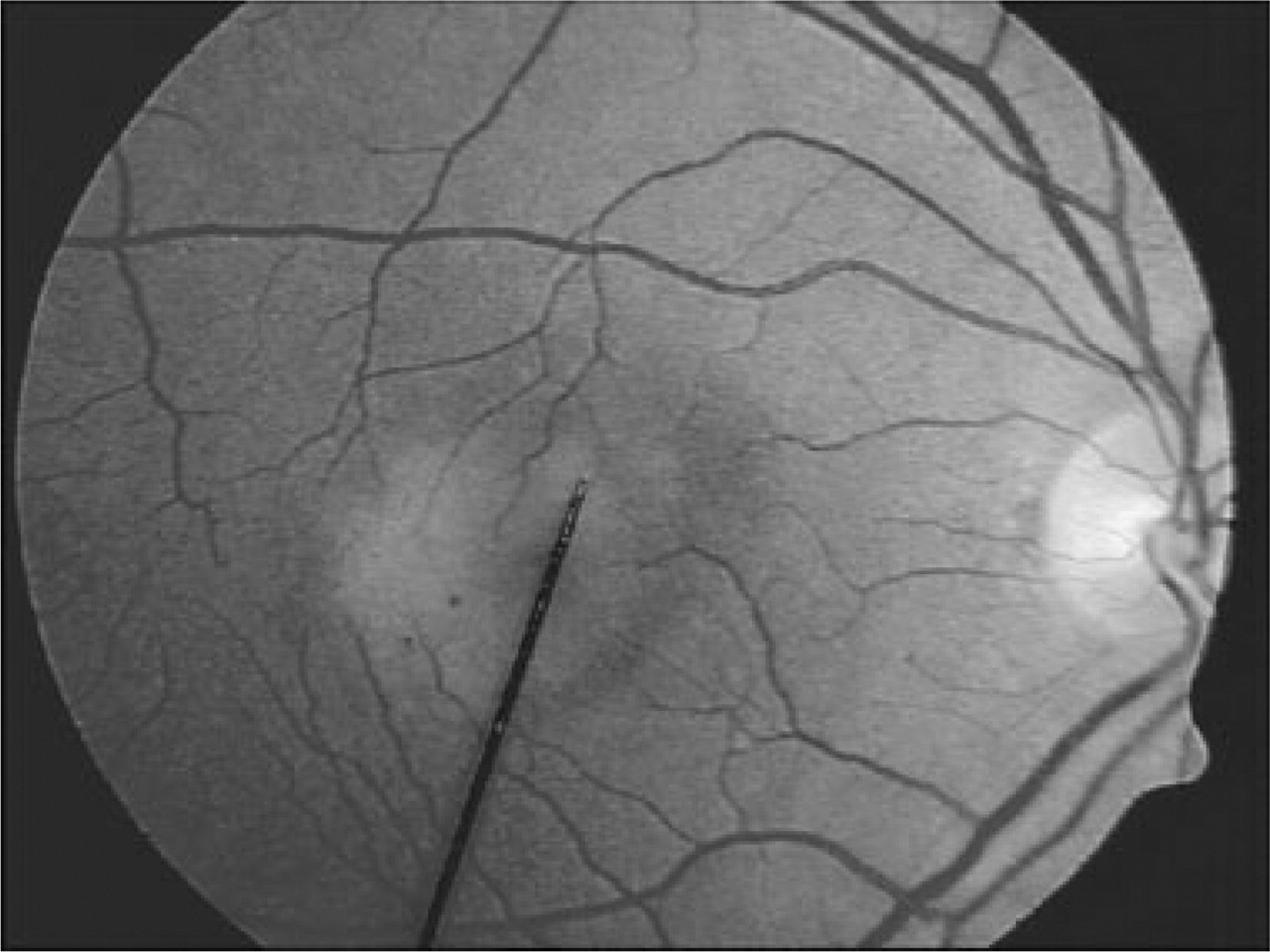
Fundus photo of the right eye.

Fluorescein angiography of the right eye in the early phase.
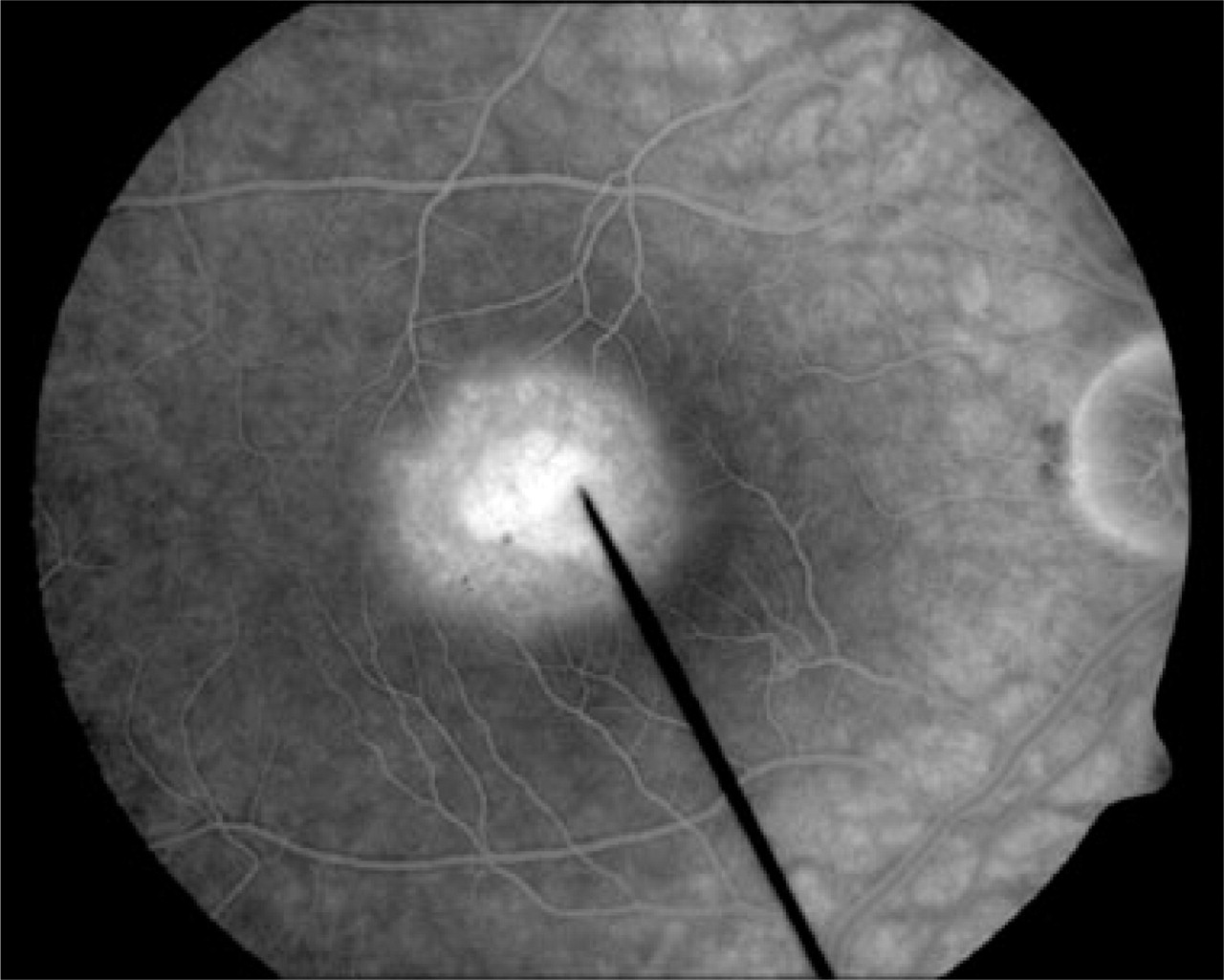
Fluorescein angiography of the right eye in the late phase.

Optical coherence tomography of both eyes done on initial examination.

Optical coherence tomography of both eyes done on follow up examination 10 days later.
At 6 months' follow-up her visual acuity improved to OD 20/70, but she continued to have difficulty with depth perception, reading, operating a motor vehicle and work performance. She needed to undergo occupational and physical therapy for gait training and to improve functional vision. At 1 year's follow-up the patient has made a full recovery and the current vision in her right eye is 20/20.
Discussion
This patient, with a 24-year history of migraine with visual aura, presented with atypical aura associated with migraine headache. The aura was atypical in that it was abrupt in onset, prolonged in duration, and associated with colour, an unusual feature for migraine aura in general and for this patient in particular. Incorrect diagnosis delayed the time to diagnosis and appropriate treatment, exposed the patient to unnecessary treatments with side-effects, and resulted in persistent visual impairment and functional impairment.
Acute multifocal posterior placoid pigment epitheliopaty is an idiopathic self-limited inflammatory disease of the choroidal vasculature. The disease typically occurs in young adults, who present with binocular visual blurring, metamorphopsia, or scotomas. The clinical course is usually self-limited with return of visual function over weeks to months. The frequent history of a preceding flu-like illness suggests a viral or parainfectious process (2). Gass has suggested an acute cellular response of the retinal pigment epithelium and choroid to an unknown (possibly viral) agent (3, 4). In AMPPPE, the presence of multifocal grey-white flat retinal lesions is seen on fundoscopy and fluorescein angiography findings. Although lesions usually resolve spontaneously, systemic complications and vision loss may occur (3, 5, 6) and respond to corticosteroid therapy. Reported neurological complications include aseptic meningitis (3, 5), headache, transient hearing loss (3, 7), optic neuritis, meningoencephalitis and stroke (3, 8). Although headache is a reported complication, to our knowledge migraine-like headache meeting the pain and associated criteria of the ICHD-II has not been previously described.
Migraine with aura is an important and prevalent neurological condition that occurs in approximately 4% of the population and has been shown to be an independent risk factor for ischaemic stroke and cardiovascular morbidity and mortality (9). The underlying physiological substrate of the migraine aura is now considered to be cortical spreading depression (CSD), which invariably begins in the occipital cortex (10). CSD propagates at a rate of approximately 3 mm/min, which accounts for why the visual symptoms begin focally, expand, and evolve over a period of at least 5 min. According to the recently revised ICHD-II, the previously defined syndromes migraine with prolonged aura and migraine with acute-onset aura have been abandoned, since the great majority of patients with such attacks have other attacks that fulfil criteria for one of the subtypes of typical migraine with aura (1). Therefore, the recommendation is that these patients should be diagnosed with either typical aura with migraine headache or diagnosed and coded as probable migraine with aura, specifying the atypical feature (prolonged aura or acute-onset aura) in parentheses. This case sharply calls into question this recommendation and highlights the need for very careful evaluation, including an ophthalmological examination, of the patient who presents with abrupt onset or prolonged aura, even with an established diagnosis of migraine with aura.