
Abstract

Introduction
Transient focal lesions of the splenium of the corpus callosum have repeatedly been observed in epileptic patients (1–14). They have been attributed both to acute seizure activity (4, 12) and to the action of antiepileptic drugs (AEDs), especially to rapid changes in AED serum levels, such as during abrupt withdrawal for presurgical evaluation (7, 11, 13–17). AEDs are increasingly being used for indications different from epilepsy, such as chronic pain or psychiatric diseases. Consistently, similar splenial lesions have been reported in a small number of patients who received AEDs for these indications, showing that AEDs can induce such lesions independently of the underlying disease (Table 1). Here, we report the case of a pain patient treated with carbamazepine.
Summary of reports on patients with AED-associated transient splenial lesions that received AEDs for an indication different from epilepsy or seizure prophylaxis

Case report
A 39-year-old woman with trigeminal neuralgia (left side, second branch) presented to our supraregional headache clinic. Occasional pain attacks had been present for a year, but the frequency had risen to two per week 6 weeks before her first evaluation in our clinic. Cerebral magnetic resonance imaging (MRI, T1- and T2-weighted images) obtained at that time was normal (Fig. 1A), and her neurologist had subsequently started her on carbamazepine. When she first presented in our clinic, she was taking 1600 mg of carbamazepine per day, without effect on attack frequency or intensity. Neurological examination was normal. We started her on misoprostol (3 × 200 μg/day) (18). Carbamazepine was tapered off over 2 weeks, and additional MRI scans were obtained with high resolution of the brainstem that did not reveal a vascular contact of the trigeminal nerve. However, a lesion in the central part of the splenium of the corpus callosum was detected, which was hyperintense in T2-weighted scans and was surrounded by a hemline of intact tissue (Fig. 1B). The lesion was isointense in T1-weighted images and did not enhance after gadolinium administration. When the patient presented for her second appointment in our clinic (3 weeks after her initial appointment and 1 week after the second MRI study), her neurological examination was normal. She had suffered no more pain attacks after starting misoprostol. We diagnosed trigeminal neuralgia of unknown origin and a benign AED-associated splenial lesion and discharged her without further therapeutic measures. A control MRI scan obtained 4 months later showed resolution of the splenial lesion (Fig. 1C).
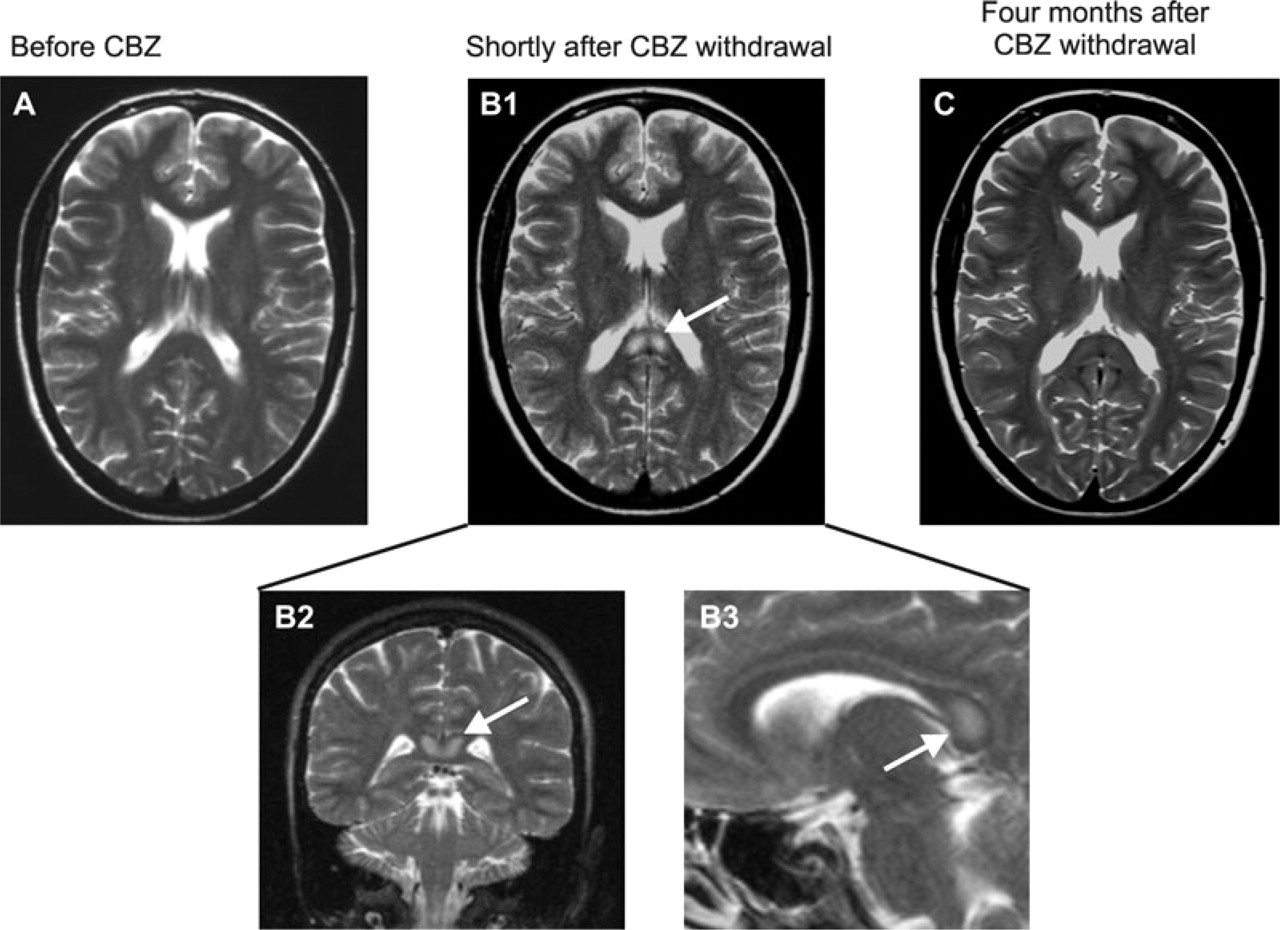
Illustration of the splenial lesion in the presently reported patient with trigeminal neuralgia. (A) T2-weighted image obtained before initiation of carbamazepine (CBZ) therapy. Subsequently, carbamazepine was started and increased up to 1600 mg/day. (B) T2-weighted images obtained shortly after tapering carbamazepine from 1600 mg/day to 0 mg/day over a period of 2 weeks. Arrows point to the splenial lesion. (C) A T2-weighted image obtained 4 months later showed resolution of the lesion.
Discussion
The benign AED-associated splenial lesions reported in the present case and in the literature (see introduction) have a stereotypic appearance on MRI examination, emerge during AED treatment or shortly after AED withdrawal, present with normal or unchanged neurological examination and resolve completely over the course of several weeks (Table 2) (1, 7, 13, 15, 19, 20).
Characteristics of benign AED-associated splenial lesions

In contrast, splenial lesions that are extended and/or present together with additional white or grey matter lesions often present with initial symptoms and may have a worse outcome (20). One such case has been reported when a patient with postherpetic neuralgia presented with nausea, headache and ataxia progressing to delirium after abrupt pregabalin withdrawal. In this case, multiple splenial lesions together with scattered periventricular lesions were present (21). While typical AED-associated splenial lesions do not show gadolinium enhancement, one case has been reported where an enhancing splenial lesion appeared during phenytoin treatment for seizure prophylaxis after removal of a frontal astrocytoma. The lesion was asymptomatic but had not resolved completely 14 months later, confirming that a more intense focal damage was present (15).
The pathogenesis of benign AED-associated splenial lesions is not clear. They constantly present with restricted diffusion (as measured by diffusion-weighted imaging), which points to a cytotoxic oedema (7, 9, 12). DTI fibre tracking and fractional anisotropy analyses showed either an intact or a reversibly disrupted organization of splenial fibres, suggesting that the oedema is glial rather than neuronal, possibly intramyelinic (1, 12, 14). It has been suggested that fluid imbalance, caused by interaction of AEDs with arginine-vasopressin (AVP) might be a factor (13, 14, 22). Excitotoxic injury also has been discussed (19). Splenial lesions with similar imaging characteristics have been detected in other conditions, including encephalitis/encephalopathy, Marchiafava-Bignami disease, hypoglycaemia, haemolytic-uraemic syndrome and chemotherapy (11, 19, 20, 23, 24). Thus, the splenium seems to be a structure with high vulnerability to various causes of cytotoxic injury.
Splenial lesions have been reported to arise during therapy or after withdrawal of almost every AED, including carbamazepine, oxcarbazepine, phenytoin, valproic acid, phenobarbital, vigabatrin, topiramate, lamotrigine, levetiracetam, gabapentin and pregabalin. Most reported cases were on combination therapy, precluding incrimination of a specific drug. AEDs that evoked splenial lesions during monotherapy or withdrawal of monotherapy were phenytoin (four cases), carbamazepine (three), lamotrigine (two), vigabatrin (one), oxcarbazepine (one), valproate (one) and phenobarbital (one). Overall, carbamazepine seems to be the drug most frequently associated with splenial lesions (6, 8, 11); however, this could also be due to frequent prescription.
The frequency of benign AED-associated splenial lesions is not known. In large series of epileptic patients receiving MRI scans for presurgical workup, in most cases during withdrawal of AEDs, the frequency of splenial lesions was between 0.7% and 5% (7, 11).
Conclusion
Transient focal splenial lesions may arise during AED treatment. Our case, as well as some others, shows that this phenomenon is not restricted to patients with epilepsy but can also occur in psychiatric and pain patients. As long as the lesions are asymptomatic and isolated, and conform to the typical imaging characteristics of benign AED-associated splenial lesions (Table 2), no diagnostic or therapeutic interventions are warranted. Nevertheless, in most cases described in the literature, the incriminated AED was discontinued and control MRI scans obtained several weeks after detection of the lesion showed complete resolution.