
Abstract
Hemicrania continua (HC) is a primary headache disorder characterized by a continuous, moderate to severe, unilateral headache and defined by its absolute responsiveness to indomethacin. However, some patients with the clinical phenotype of HC do not respond to indomethacin. We reviewed the records of 192 patients with the putative diagnosis of HC and divided them into groups based on their headaches' response to indomethacin. They were compared for age, gender, presence or absence of specific autonomic symptoms, medication overuse, rapidity of headache onset, and whether or not the headaches met criteria for migraine when severe. Forty-three patients had an absolute response and 122 patients did not respond to adequate doses of indomethacin. The two groups did not differ significantly in terms of age, sex, presence of rapid-onset headache, or medication overuse. Autonomic symptoms, based on a questionnaire, did not predict response. Eighteen patients could not complete a trial of indomethacin due to adverse events. Nine patients could not be included in the HC group despite improvement with indomethacin: one patient probably had primary cough headache, another paroxysmal hemicrania; three patients improved but it was uncertain if they were absolutely pain free, and four patients dramatically improved but still had a baseline headache. We found no statistically significant differences between patients who did and did not respond to indomethacin. All patients with continuous, unilateral headache should receive an adequate trial of indomethacin. Most patients with unilateral headache suggestive of HC did not respond to indomethacin.
Introduction
Hemicrania continua (HC) is a primary headache disorder first designated in 1984 by Sjaastaad and Spierings (1). They reported two patients, a woman aged 63 years and a man aged 53 years, who developed strictly unilateral headaches that were continuous from onset and absolutely responsive to indomethacin. HC may be more common than previously appreciated, as > 100 cases have been reported (2). HC is a unilateral, continuous, indomethacin-responsive headache with periodic exacerbations. Its main features are (i) unilaterality of pain, and (ii) absolute response to indomethacin (Table 1). Atypical cases (bilateral or alternating sides) have been reported (3). HC exists in both continuous and remitting forms, although the remitting form is less common. HC is usually associated with autonomic symptoms, such as conjunctival hyperaemia, tearing, rhinorrhoea, nasal congestion, ptosis and miosis. Jabs and jolts (4) and migrainous features (5) are also common.
The International Classification of Headache Disorders 2nd edition diagnostic criteria for hemicrania continua

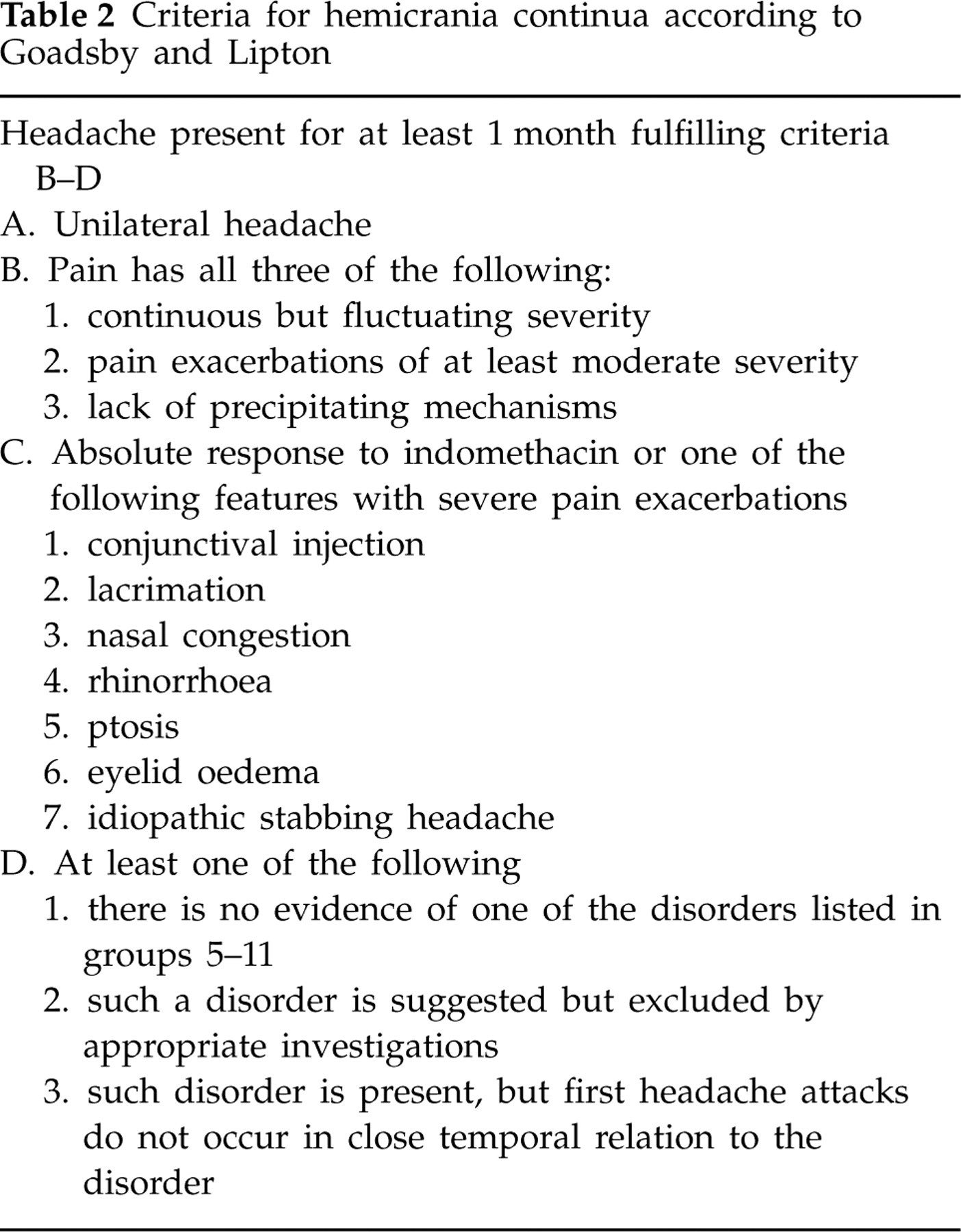
HC as currently defined requires an absolute response to indomethacin, but some patients do not respond to indomethacin despite meeting the clinical phenotype (6, 7). Goadsby and Lipton have provided an alternative diagnostic criterion to include indomethacin non-responders (8) (Table 2). Some have proposed categorizing patients into groups based on their treatment response. Patients who have headache relief with indomethacin would be called ‘hemicrania continua vera’ and patients without improvement would be called ‘hemicrania generic incerti’ (of undetermined nature) (9). There also have been case reports of patients with indomethacin-responsive HC who experienced pain relief from cyclooxygenase-2 inhibitors (10), verapamil (11), topiramate (12) and melatonin (13). Secondary phenotypic HC may also be seen in patients with carotid artery dissection (14) or brainstem infarct (15). Functional neuroimaging of patients with HC using positron emission tomography scans demonstrates activation in both the posterior hypothalamus (similar to cluster headache) and the brainstem (similar to migraine) (16). Greater occipital nerve stimulation may be effective in treating HC (17). One patient with a history of episodic paroxysmal hemicrania developed HC 2 years later (18). This suggests that HC may overlap with other primary headache disorders.
Criteria for hemicrania continua according to Goadsby and Lipton
The clinical characteristics that make patients more likely to respond to indomethacin are not known. As a result, it is recommended that all patients with unilateral, unremitting headache receive a trial of indomethacin unless it is contraindicated. The purpose of this study was to see if any clinical characteristics predict a response to indomethacin.
Methods
We reviewed the electronic medical records (EMR) of all patients with the putative diagnosis of HC seen from 1998 to 2007 at our tertiary out-patient centre. Approval for this study was obtained from the Thomas Jefferson University Institutional Review Board. We reviewed each individual chart to confirm that each patient had a unilateral, constant headache and assessed which patients had received a trial of indomethacin. Patients who had not received an indomethacin trial or did not follow up for reassessment were excluded.
We defined an adequate trial of indomethacin as ≥ 150 mg for 2 weeks or 225 mg for 1 week. We identified 192 patients with a putative diagnosis of HC, as entered in the EMR by the treating physician.
Patients were divided into groups of indomethacin responders (if they had an absolute response to indomethacin) and non-responders. Based on the International Headache Society (IHS) classification, we classified patients who said they had had improvement but no headache-free time as non-responders. Patients who stopped the medication due to adverse events (AEs) before completing an adequate trial and patients with an unclear response were listed separately.
We compared the indomethacin-responsive and non-responsive groups for age, gender, presence or absence of specific autonomic symptoms, medication overuse, and if the headaches met IHS criteria for migraine when severe. Based on IHS classification of new daily-persistent headache as a headache disorder that becomes daily and unremitting within 3 days of onset, patients with this type of onset were classified as ‘rapid-onset headache’.
From the EMR, we determined the patient's gender and their age at the time the physician prescribed indomethacin. All new patients filled out an encounter form at their first visit, at which time we asked them about typical migraine symptoms, such as the headache's character and location, associated symptoms, autonomic symptoms, and presence or absence of aura. Autonomic symptoms were determined based on the patient response on the questionnaire, which was entered into the EMR prior to the initial visit. After performing the initial history and physical, the treating physician corrected any errors in the EMR. We reviewed each patient's medical record to determine whether or not the constant headache evolved rapidly (< 3 days). We also determined whether medication overuse, defined as the use of simple analgesics > 3 days/week or the use of opioids, triptans, barbiturates, or combination analgesics more than twice per week, existed.
Results
We identified 43 patients with an absolute response (I+) and 122 patients who did not respond to adequate doses of indomethacin (I−); 18 patients were not able to complete an adequate indomethacin trial due to AEs, and nine patients were difficult to classify. Although the minimum adequate indomethacin trial was at least 150 mg for 2 weeks or 225 mg for 1 week, the majority were on it for a longer period of time.
Of the 43 I+ HC patients, 24 (59%) were women, with an average age of 40.5 years (range 16–82 years). Of the 42 patients who were asked about autonomic symptoms, nine (21%) had congestion or rhinorrhoea with their attacks, 12 (29%) had either lacrimation or injection, and 14 (33%) had either ptosis or miosis. One patient's chart did not list autonomic symptoms. Twenty-four of 42 patients (57%) reported at least one of these three autonomic symptoms. Fifteen of 42 patients (36%) presented with a rapid-onset headache, 21 (50%) met criteria for migraine during attacks and 24 (55%) had medication overuse. The average dose of indomethacin used to treat these patients was 194 mg (see Table 3).
Patients with putative hemicrania continua, responsive to indomethacin
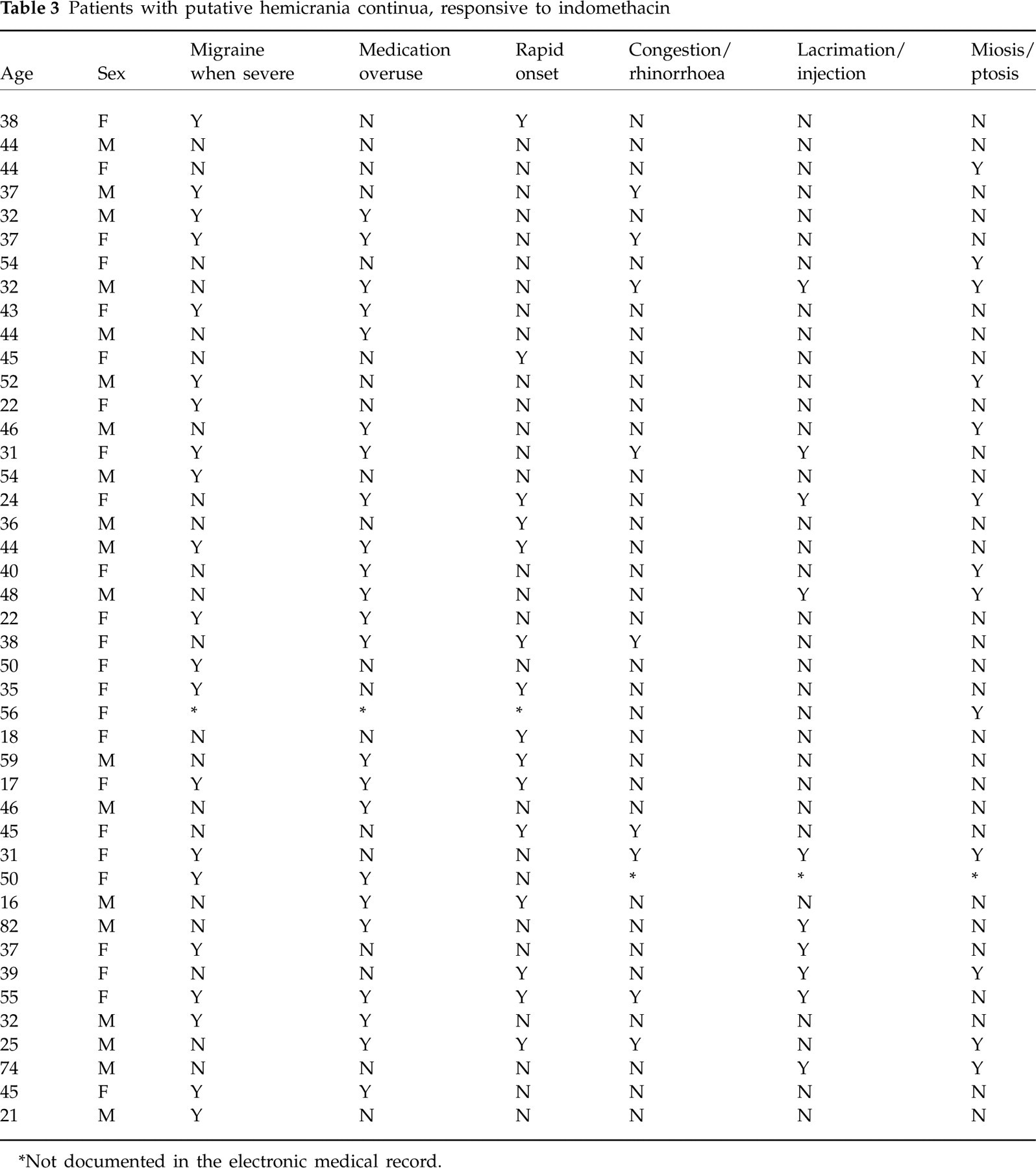
∗Not documented in the electronic medical record.
Among the 122 I− HC patients, 75 (61%) were women, average age 42.9 years. Of these patients, 120 were asked about autonomic symptoms. Eighteen patients (15%) reported congestion or rhinorrhoea, 36 (30%) either lacrimation or injection and 34 (28%) either ptosis or miosis. In all, 73 (61%) of the I− patients reported at least one autonomic symptom during attacks. Fifty-six of 121 patients (46%) presented with rapid-onset headache, 74 of 122 (61%) had attacks that met criteria for migraine and 67 patients (55%) overused acute medications (see Table 4).
Putative hemicrania continua, not responsive to indomethacin



∗Not documented in the electronic medical record.
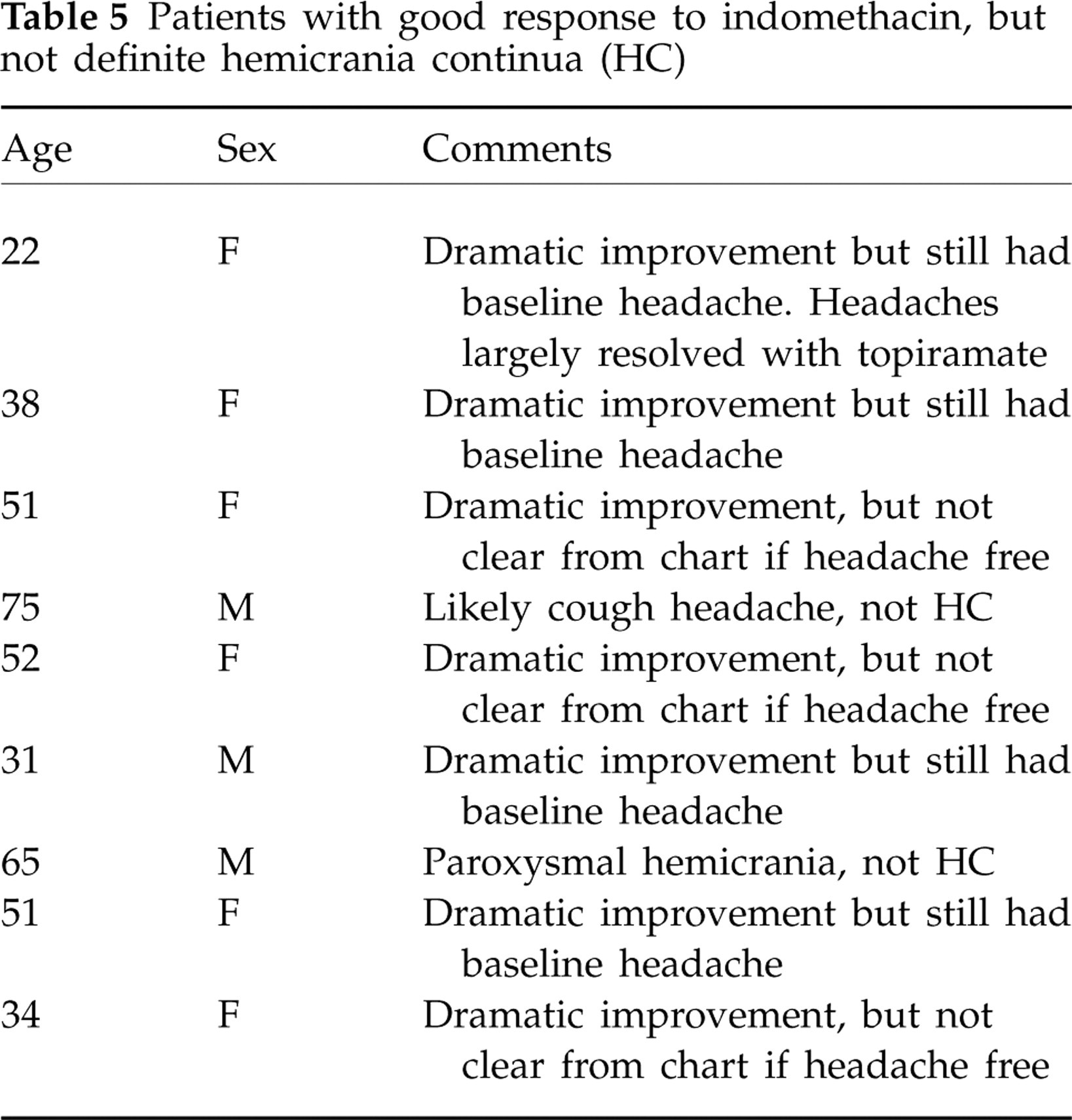
Nine patients were difficult to classify. Two had an incorrect diagnosis. (One had primary cough headache and another paroxysmal hemicrania; both responded absolutely to indomethacin.) Four patients reported dramatic improvement, but were not headache free despite high doses of indomethacin. Three patients also reported dramatic improvement, but we could not determine from the EMR if they were truly headache free (see Table 5).
Patients with good response to indomethacin, but not definite hemicrania continua (HC)
Of the patients who did not respond to indomethacin, some responded to other treatments, some did not improve, and some were lost to follow-up.
Using a paired t-test to compare patient ages and χ2 test for the other variables, we compared the two groups of patients who did and did not respond to indomethacin. There were no significant differences between the two groups in terms of age (P = 0.33), sex (P = 0.51), presence of migraine with severe attacks (P = 0.22), rapidity of headache onset (P = 0.23) or medication overuse (P = 0.98).
Discussion
HC is an uncommon headache disorder defined as a unilateral headache responsive to treatment with indomethacin, yet in this study only a minority of patients with putative HC responded to indomethacin. We found no statistically significant differences in the demographics or clinical characteristics of responders and non-responders. Specific autonomic symptoms, rapid-onset headache, and presence of migraine did not predict response. This suggests that HC is a syndrome that has significant overlap with other primary headache disorders and reinforces that all patients with continuous, unilateral headache should receive an adequate trial of indomethacin.
HC, by the International Classification of Headache Disorders, 2nd edn (ICHD-II) definition, is not a unilateral headache with response to indomethacin (the variable of interest). It is a unilateral headache with autonomic symptoms and response to indomethacin (19). We found that the response to indomethacin is independent of autonomic symptoms. This could be due to underestimating autonomic symptoms, since our study relied on the initial patient questionnaire. Many patients in both groups denied any autonomic symptoms. Technically, these patients did not meet criteria for HC, even if they had headaches that responded absolutely to indomethacin. Perhaps autonomic symptoms in HC are more subtle and underreported than those in trigeminal autonomic cephalgias. Perhaps the ICHD-II classification is wrong, or subsets of HC exist. This is the situation for short-lasting unilateral neuralgiform headache attacks with conjunctival injection and tearing (SUNCT) and short-lasting unilateral neuralgiform headache attacks with cranial autonomic symptoms (SUNA). SUNCT requires both conjunctival injection and tearing, whereas SUNA requires only one autonomic symptom. Perhaps we do not need autonomic symptoms to be present at all.
There are a number of possible reasons why many patients did not improve. Many of the patients with putative HC and migrainous features may simply have what has been described as ‘side-locked’ migraine (20). Because migraine is much more common than HC, it is not surprising that an unusual migraine presentation would be more common than HC. Another possibility is that these non-responders with prominent autonomic symptoms might have a variant of a trigeminal autonomic cephalgia. In a recent descriptive study, 42% of patients with cluster headache reported a painful state between attacks (21), and patients with HC may respond to verapamil. Other patients in the indomethacin non-responsive group may have less common headache types, such as nummular or cervicogenic headache. Ours is a tertiary clinic population, and patients are usually seen after failing treatment with multiple medications. This may lead to bias. Patients with more typical HC and successful treatment with indomethacin are less likely to present to our attention. Other clinical characteristics that might help differentiate HC from putative HC that does not respond to indomethacin are the presence of jabs and jolts or a sensation of ‘sand in the eye’. Because the initial-visit questionnaire did not contain these questions, these symptoms were not systemically examined in the EMR. Although the two groups overused medications at a similar rate, and many patients overused multiple different classes of acute medication, perhaps patients with true HC are more likely to overuse combination analgesics or non-steroidal anti-inflammatory medications than triptans. Another possible reason for the poor response to indomethacin might be the effect of medication overuse. Although many patients respond to indomethacin despite medication overuse, others suggest that pain medications such as opioids prevent non-steroidal medications such as ketorolac or indomethacin from working (22).
This study represents the largest case series of HC to date. We plan to study our patients with HC in more detail in the future.