
Abstract
During the past few decades, much controversy has surrounded the pathophysiology of migraine. Cortical spreading depression (CSD) is widely accepted as the neuronal process underlying visual auras. It has been proposed that CSD can also cause the headaches, at least in migraine with aura. We describe three patients, each fulfilling the International Headache Society criteria for migraine with aura, who suffered from headaches 6–10 days per month. Two patients were treated with flunarizine and the third patient with topiramate for the duration of 4 months. All patients reported that aura symptoms resolved completely, whereas the migraine headache attacks persisted or even increased. These observations question the theory that CSD (silent or not) is a prerequisite for migraine headaches.
Introduction
Migraine is one of the most common neurological disorders and is observed in about 14% of the population. Migraine attacks are characterized by unilateral, throbbing, moderate to severe headache, lasting 4–72 h, typically accompanied by nausea and photo- and phonophobia (1). In approximately 20% of patients, the headache may be preceded by transient neurological symptoms that usually develop gradually over > 5 min and last for < 60 min (migraine with aura). Auras are most frequently visual (> 90%), but may also involve other sensory symptoms (pins and needles, numbness), hemiparesis or speech deficits (2).
Migraine visual aura frequently begins as a fortification near the centre of vision that slowly expands and propagates towards the periphery of the visual field. These symptoms are typically accompanied by scotoma. Analysing his own visual aura in 1941, Lashley postulated that the fortifications resulted from cortical excitation in the visual cortex and that the adjacent scotoma resulted from subsequently decreased neuronal excitability (3). He calculated that the neural disturbance was propagating across the cortex at approximately 3 mm/min. Only a few years later, Leao reported an electrophysiological correlate in the rabbit cerebral cortex and coined the expression ‘cortical spreading depression (CSD)’ (4). This is characterized by a slowly propagating (2–6 mm/min) wave of neuronal and glial depolarization and is followed by long-lasting suppression of neuronal activity. The depolarization phase is associated with an increase in regional cerebral blood flow (rCBF), whereas the phase of reduced neuronal activity is associated with a reduction in cerebral blood flow. Based on recent magnetoencephalography and neuroimaging studies in humans (5, 6), which have shown several CSD-typical changes in the cortex of migraineurs while experiencing a visual aura, it is nowadays widely accepted that CSD is the neurophysiological correlate of visual aura. Presumably, aura involving sensory symptoms results from CSD-like events within sensory cortices.
Based on a recent study by Bolay and coworkers showing c-fos staining after experimental CSD in the rat trigeminal nucleus caudalis (TNC), it was hypothesized that CSD causes headache in migraineurs by means of activating the trigeminovascular reflex (7). The observation that recurrent experimental CSD of the rat hippocampus evoked an increase in bilateral c-fos immunostaining within the TNC led to the assumption that in patients without aura, CSD might be confined to subcortical regions (i.e. hippocampus) and this may trigger headache in migraine without aura (silent CSD) (8). On the other hand, electrophysiological studies have failed to demonstrate trigeminal activation with CSD (9).
To date, the trigger mechanisms of migraine aura/CSD and the question of whether or not CSD is a prerequisite for developing a migraine headache are controversial (7, 10–12). Here we describe three patients whose aura symptoms resolved under treatment with flunarizine or topiramate, whereas the headaches persisted. Our observations indicate that at least in these patients, migraine headaches may develop without being preceded by CSD.
Case reports
We describe three patients (two of whom are first-degree relatives), each fulfilling the International Headache Society criteria for migraine with and without aura (1).
Patient 1
Starting at 19 years, this 51-year-old woman had suffered from mostly unilateral, right-sided, throbbing headaches, associated with nausea, vomiting and phono-, photo- and osmophobia. Previously, headaches had occurred with menstruation 3 days per month. Since onset of menopause she had suffered from headaches approximately 6 days per month (two to three attacks per month, each lasting 48–72 h). The intensity was reported to be between 6–8 out of 10 and increased with exertion. In 50% of the attacks headaches were preceded by a visual aura with slowly propagating scintillations. Less frequently, the headaches were preceded by sensory deficits of the left arm or dysphasia. There was no family history of migraine. Neurological examination was normal. Magnetic resonance imaging (MRI) of the head 1 year prior to consultation had shown no abnormalities. There was a past history of reflux oesophagitis, hypothyroidism and arterial hypertension that have been treated with L-thyroxin and a β-blocker (nebivolol).
According to the patient, paracetamol and ibuprofen did not attenuate the headaches, whereas ergotamine, acetylsalicylic acid (ASA) and naproxen were partially successful. The subcutaneous application of sumatriptan led to intolerable side-effects. Other triptans did not allay the pain. Previous prophylactic therapy with metoprolol and flunarizine had had no effect on aura or headache, respectively. Oestradiol valerate brought about only some abatement. Lamotrigine was stopped after a short period due to sleep disturbance, palpitations and flu-like symptoms. We started prophylactic treatment with 100 mg topiramate, which was given for 4 months. The patient reported taste disturbances and hyperosmia, but otherwise tolerated topiramate well. Aura symptoms resolved completely and headache intensity only slightly decreased, whereas headache frequency increased from approximately 6 days/month to 8 days/month. After discontinuation of the prophylactic medication, auras recurred.
Patient 2
This 47-year-old lady presented to our out-patient clinic with a 30-year history of bifrontal and parietal pressing or throbbing headache, accompanied by nausea, vomiting, phono- and photophobia, palpitations (during the past year) and, less often, brachiofacial allodynia. Initially, attacks lasted 12–24 h, were particularly associated with menstruation and responded well to ASA. All symptoms resolved during pregnancy and lactation. Over the years, frequency and intensity had increased, so that at consultation she suffered from moderate to severe headaches 8 days per month (two attacks per month, each lasting 3–4 days). Eighty per cent of these attacks were preceded by visual aura (slowly propagating fortifications), and 20% of the time a headache did not follow the visual aura. Her daughter (patient 3) also suffered form migraine with and without aura. Neurological examination was normal. Cranial computed tomography 3 years prior to consultation had revealed no abnormalities. A 24-h ECG performed because of palpitations associated with the headaches was also normal. There was a past history of rheumatoid arthritis and hypothyroidism, treated with sulfasalazine, etanercept and levothyroxine, respectively. The headaches responded well to rizatriptan and zolmitriptan, which were taken approximately 8 days per month. She had never received prophylactic treatment before coming to our clinic. We started with 5 mg flunarizine for 4 months. Apart from a gain in weight (5 kg), this was well tolerated. The patient reported that aura symptoms resolved completely, whereas the headaches and associated allodynia persisted with the same frequency. Subsequently, lamotrigine (75 mg) was given for 7 months. This led to a transient reduction of headache frequency (2–3 days per month compared with 8 days) and intensity, which unfortunately did not last. Under treatment with lamotrigine she experienced an isolated visual aura only once.
Patient 3
The second patient's daughter, patient 3, an otherwise healthy 17-year-old woman, had begun to suffer at 10 years of age from bifrontal throbbing headache attacks, associated with nausea, vomiting, phono-, photo- and osmophobia and less often with allodynia of the scalp. Intensity was 7–8 out of 10 on the visual analogue scale and increased with exercise. Fifty per cent of the headaches were preceded by visual aura with a slowly expanding skotoma. Less frequently, visual aura occurred without headache. Over the years, the frequency had increased so that when presenting to our out-patient clinic she suffered form headache attacks approximately 10 days per month. Neurological examination was unremarkable. MRI of the brain, performed 7 years prior to consultation, had been normal. Apart from a contraceptive (ethinylestradiol) she took no regular medication. Thomapyrin (Boehringer Ingelheim, 250 mg acetylsalicylic acid, 200 mg paracetamol and 50 mg coffein) and almotriptan alleviated the headaches, whereas zolmitriptan and rizatriptan had no effect. We started prophylactic treatment with 5 mg flunarizine for 4 months. Side-effects were weight gain (3 kg), mood deterioration and tiredness. The patient reported that visual aura had resolved completely, whereas allodynia and headache frequency and intensity remained unchanged. Subsequently, lamotrigine (50 mg) was given, which led to a temporary reduction in headache frequency (3–4 days/month compared with 10 days/month) but did not last. Visual auras remained absent under treatment with lamotrigine, but recurred after prophylactic treatment was stopped.
Discussion
Recent magnetoencephalography and neuroimaging studies in humans have provided inferential evidence that CSD-like phenomena within the occipital lobe generate visual aura in migraine (5, 6). In particular, numerous excellent imaging data have provided strong evidence that the aura phase of migraine, but not the headache phase, is associated with a reduction in cerebral blood flow (6, 13, 14). Measuring cortical thickness and using diffusion tensor imaging (DTI), a recent study examined the motion-processing visual network in migraine patients and compared them with healthy controls (15). This study found an increase in cortical thickness of motion-processing visual areas in migraineurs. These changes were found in an area that has previously been described as a source in spreading changes involved in visual aura (6). In addition, DTI revealed that migraineurs have alterations in the superior colliculus and the lateral geniculate nucleus, which are also involved in visual processing. It has been suggested (15) that structural abnormality in the network of motion-processing areas could account for, or be a result of the cortical hyperexcitability observed in migraineurs. Because patients with migraine without aura have the same changes, the authors suggest that these patients have clinically ‘silent aura’. Further studies have also suggested a relationship between susceptibility to CSD and migraine. An important example is the inherited basis of familial hemiplegic migraine. CACNA 1a knockin mice have a reduced threshold and increased velocity of CSD (16).
Female gender and female sex hormones (oestrogen and progesterone) in mouse models are determinants of lower CSD thresholds (17, 18), consistent with a higher female prevalence of migraine. The results of the latter studies seem in favour of a pathogenic relationship between CSD/aura and headache in migraine. However, the link between aura and headache remains controversial, despite some valuable theoretical considerations (7). It should be remembered that only 30% of migraineurs have aura (2).
In our patients, the migraine prophylactic agents topiramate and flunarizine, which have the potential to suppress CSD or CSD-associated phenomena in animal models (19, 20), impeded aura symptoms (probably by suppressing CSD) without attenuating the patients’ headaches. Similarly, a study of intranasal ketamine in the treatment of aura in familial hemiplegic migraine has demonstrated that in some patients ketamine could reproducibly abort the aura (five out of 11), but did not affect the headache in three of these five patients (21). Studies on the efficacy of lamotrigine in preventing migraine headache have yielded disappointing results (22), whereas it seems to be effective in preventing aura in migraine (23, 24). In contrast, topiramate has proven to be effective in preventing migraine headache in several randomized, placebo-controlled trials (25), but it is not clear whether topiramate is effective in the therapy of migraine aura (26). These observations raise doubts over the theory that CSD is a prerequisite for migraine headache. Doubts are aggravated by the observations of Richter and co-workers, who have demonstrated that the α2-receptor agonist clonidine, which does not attenuate headache frequency in patients with migraine, was effective in suppressing CSD, probably through an action on presynaptic neuronal α2-adrenoceptors (27, 28). Migraineurs without aura also pose a challenge to the hypothesis that CSD is required for triggering a migraine headache. It has been suggested that in these cases, SD might take place in subcortical areas, such as the hippocampus, and may therefore remain clinically unapparent (8). Although most studies including methods such as single-photon emission computed tomography (29, 30), positron emission tomography (PET) (31, 32) and perfusion-weighted imaging (PWI) magnetic resonance (33) did not reveal CSD-like phenomena in migraine without aura, some authors have found such cortical propagating phenomena during migraine without aura using PET (34) or functional MRI (35). Woods and co-workers have described bilateral spreading cerebral hypoperfusion during a spontaneous migraine attack in a patient who suffered from migraine without aura (34). However, the typical hyperperfusion at the front of the wave that has been described in animal experiments (36, 37) was not detected in this patient. One explanation is the spatial and temporal resolution of about 70 s of PET rCBF measurements. On the other hand, the observed changes were relatively short-lasting, with substantial recovery in a relatively short time. Studies not showing cortical propagating phenomena in association with migraine without aura have been few and attacks had already commenced (31, 32), so very early changes in CBF may have been missed. Another possible explanation for the negative results of the study by Sanchez del Rio using PWI of 14 attacks of spontaneous migraine without aura (33) could be that the vascular or electrical wave changes in migraine without aura (but not aura itself) are below the resolution of PWI. Despite all the logistic problems, there is a clear need for further studies to investigate migraine attacks as early as possible to confirm or reject these results.
A causal correlation between CSD and headache would not explain why some patients with migraine with aura also experience isolated auras (International Classification of Headache Disorders, 2nd edn, code 1.2.3) and why aura may also occur during or, in up to 3%, even after the headache (38). Furthermore, aura symptoms do not reliably predict the side of the headache (39), and numerous patients suffer from bilateral headache, whereas CSD is confined to one hemisphere and does not spread to the contralateral side. It is important to note that the migraine process does not start with the headache or even the aura (see Table 1). In a study by Giffin and colleagues, > 70% of the headache attacks were preceded by premonitory symptoms (other than aura), starting up to 72 h before the headache (40). This is in accordance with neuropsychological studies that have shown a lack of habituation measured by event-related and evoked potentials in the interictal period with abrupt normalization during the attack (41). The existence of interictal changes, including premonitory symptoms, cannot easily be explained by the CSD theory, just as the pathophysiology of vegetative symptoms during the attack remains unexplained.
Clinical reasons contradicting the theory that aura is a prerequisite for developing headache in migraine
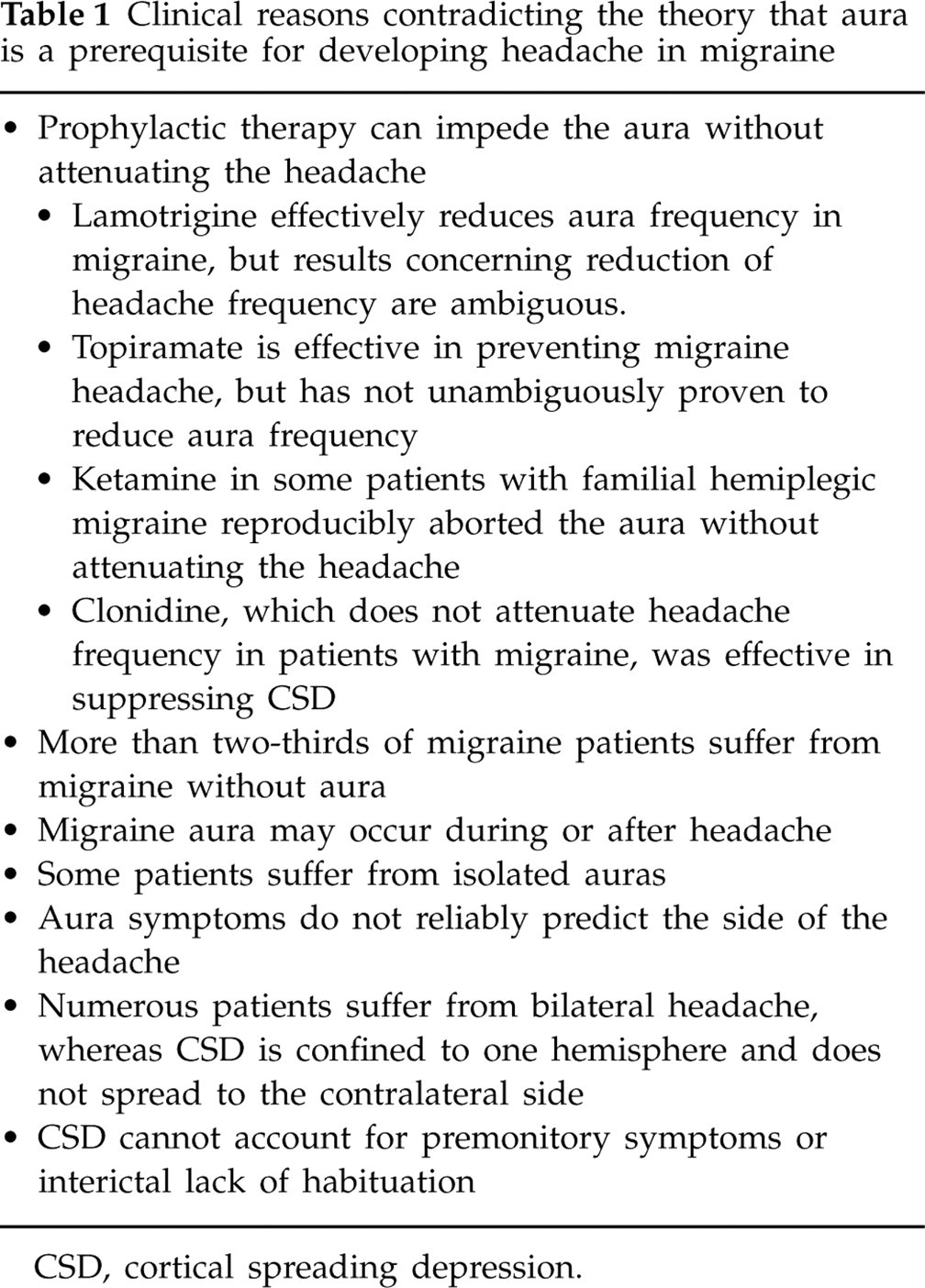
CSD, cortical spreading depression.
The fact that some migraine prophylactic agents are capable of suppressing CSD in animal models does not necessarily prove a causal correlation between aura/CSD and headache in migraineurs. A possible explanation for the dual effects of some agents of reducing nociceptive transmission and inhibiting the aura could be an action at different sites. Indeed, topiramate is capable of inhibiting CSD (42) and also acts on trigeminovascular nociceptive transmission (43). This would explain why topiramate may exert both effects (preventing aura/CSD and reduction of headache frequency and intensity), but not necessarily within the same patient.
One possible explanation for these questions could be that it is not CSD itself that triggers the headache, but CSD-related phenomena such as propagated haemodynamic changes or intercellular calcium waves in astrocytes. Using optical intrinsic signal imaging and electrophysiology, Charles and co-workers have shown that dilation of surface arterioles not only propagated with a significantly greater velocity than the parenchymal CSD, but also spread into regions that were not reached by CSD. Propagation of vasodilation was found along individual vessels and never skipped across an area of the cortex without an intervening vessel (44). Of note, CSD determines the velocity of the astrocytic calcium wave. However, the astrocytic calcium wave penetrates a larger territory. Application of the N-methyl-D-aspartate-receptor antagonist MK-801 blocked CSD, but not the astrocyte calcium wave (45). Astrocyte calcium waves are associated with significant active release of neurotransmitters and neuromodulators (i.e. glutamate and adenosine triphosphate) (46) that could activate nociceptive pathways, and both astrocytes and vascular cells are also capable of releasing nitric oxide, another potentially important modulator of pain transmission.
These findings suggest that the vascular and glial propagating waves have independent and possibly active mechanisms of propagation rather than merely following the CSD as passive events. Taking these results into consideration, it would be conceivable that through prophylactic treatment, we blocked CSD without inhibiting the associated glial and vascular phenomena.
If we assume that not the cortical neuronal depolarization wave, but either the haemodynamic changes or the glial calcium wave trigger migraine headaches, and if we postulate that these three phenomena are linked but could also occur independently of one another, this theory would explain why some people suffer from migraine without aura (no neuronal wave), some suffer from migraine with aura (all three phenomena) and some from isolated auras without a headache (isolated neuronal wave). This theory would also explain why some drugs suppress CSD, but do not attenuate migraine headaches (clonidine) and why other drugs may impede the aura without attenuating the headache.
However, the multiplicity of cortically spreading phenomena is an evolving area of investigation and the interaction of these different wave phenomena is not completely understood. There are certainly significant differences between the rodent and human cortex and biology of CSD that limit transferring observations of rodent experiments to human cortical events.
Footnotes
Competing interests
None to declare.