
Abstract
The revised criteria of the International Headache Society (IHS) for paediatric headache do not differentiate among age groups. This study aims to determine if different symptoms of migraine are specific or typical of different age groups of children. The files of 160 children (79 boys, 81 girls, mean age 10.39 ± 3.71 years) with migraine treated at the paediatric headache clinic of a tertiary centre were reviewed. The diagnosis was based on the criteria of the IHS (ICHD-II). The patients were divided by age into three groups according to educational status, ≤6 years (preschool, group 1), >6 to ≤12 years (elementary school, group 2) and >12 to ≤18 years (secondary school, group 3), and compared by symptoms and signs. Symptoms of migraine with and without aura were also compared. There was no significant difference among the groups in rates of unilateral headache, phonophobia, photophobia, awakening pain, nausea or worsening of pain during physical activity. The parameters found to be statistically significant were dizziness and duration of migraine, and aura which increased with time. Frequency of attacks increased with age. The single statistically significant parameter found to be more frequent in younger age was vomiting. The statistically significant parameters of nausea and duration of migraine were more frequent in migraine with aura compared with migraine without aura. In conclusion, most of the migraine symptoms included in the 2004 recommendations of the IHS are not typical for specific paediatric age groups, probably because brain maturity is a continuous process. A familial history of migraine is a frequent finding among all age groups and should be considered in the paediatric criteria, especially in younger children in whom diagnosis is more difficult. Vomiting may help the diagnosis of migraine in young children with a familial history of migraine.
Introduction
Migraine is recognized as an important cause of paediatric headache. Prompted by findings that the diagnosis of migraine is often missed in children (1, 2), in 2004 the International Headache Society (IHS) broadened its criteria for paediatric migraine [International Classification of Headache Disorders, 2nd edn (ICDH-II)] (3). Nevertheless, the diagnosis remains elusive in many cases (3) owing to the wide heterogeneity of this patient population and differences in the ability of children of different ages to describe pain and disease symptoms.
The aim of the present study was to determine if certain symptoms of migraine are more common or typical to specific paediatric age groups and to compare symptoms of migraine without aura vs. migraine with aura.
Methods
We reviewed the files of 160 children with migraine treated from 2004 to 2006 at the Paediatric Headache Clinic of the Ambulatory Day Care Department of Schneider Children's Medical Centre of Israel, a tertiary, university-affiliated facility. The diagnosis was based on the 2004 criteria of the IHS (ICHD-II) (2). The patients were divided by age into three groups according to educational status: ≤ 6 years (preschool, group 1), > 6 to ≤ 12 years (elementary school, group 2), and >12 to ≤ 18 years (secondary school, group 3). Symptoms and signs were compared among the groups.
All patients were examined by the same paediatrician. Patients were also examined by a paediatric psychiatrist if referred for psychiatric evaluation by the paediatrician.
The study was approved by the institutional Helsinki Committee.
Statistical analysis
Data were managed and analysed with BMPD software (BMPD, Los Angeles, CA, USA)
(4).
Continuous variables were shown as means and
Results
The study sample consisted of 79 boys and 81 girls, mean age (±
There was no statistically significant difference in the following parameters among the three age groups: male : female ratio, family history of migraine, rate of psychiatric diagnosis, unilateral headache, phonophobia or photophobia, awakening pain, nausea, worsening of pain during physical activity, type of pain, family migraine or motion sickness (Table 1).
Patient and headache characteristics in children of different age groups
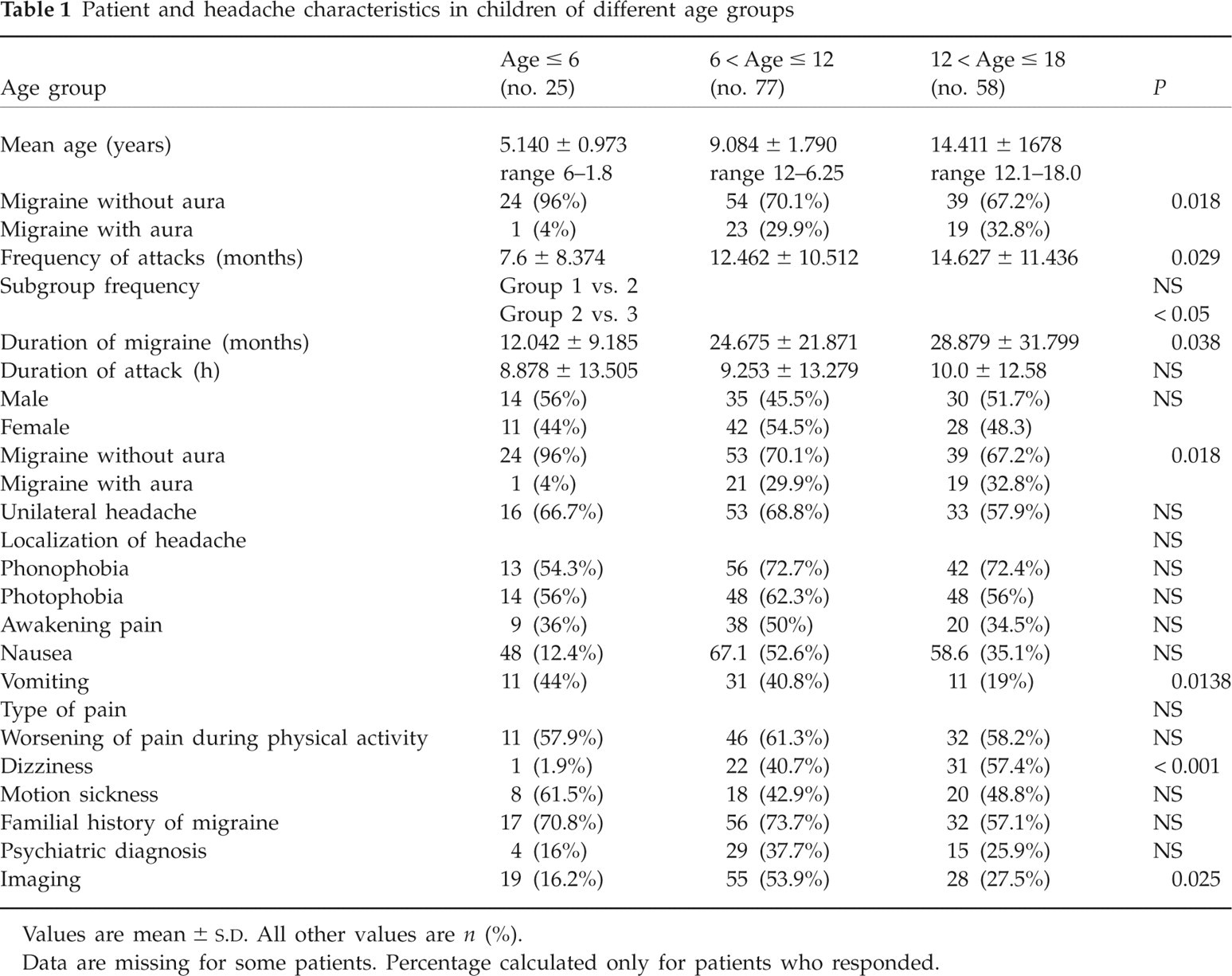
Values are mean ±
Data are missing for some patients. Percentage calculated only for patients who responded.
The parameters that yielded a statistically significant difference among older age groups were symptoms of dizziness, frequency of attacks per month (more frequent with increasing age) and duration of migraine (longer with increasing age). Comparing migraine with and without aura in the three age groups showed that aura was more frequent in older children. Vomiting was found to be the only statistically significant parameter more frequent in younger ages (Table 1).
We found no statistical difference in the following parameters when comparing symptoms according to type of migraine: frequency of attacks per month, duration of migraine attack by hours, male/female ratio, unilateral pain, localization of pain, photophobia, phonophobia, awakening pain, vomiting, type of pain, worsening of pain during physical activity, dizziness, motion sickness, family migraine and psychiatric diagnosis (Table 2).
Patient and headache characteristics in children according to diagnosis

Values are mean ±
Data are missing for some patients. Percentage calculated only for patients who responded.
When comparing the two types of migraine, nausea and duration of migraine before diagnosis were statistically significant and more frequent in older children.
A borderline statistically significant difference was noted when comparing diagnosis of migraine with aura vs. age (more frequent in the oldest group, P = 0.06) (Table 2).
Discussion
In our study no statistically significant difference was found in various symptoms of migraine in different age groups except dizziness, vomiting, migraine frequency and type of migraine.
In a study of the relationship between clinical symptoms of migraine and age, Wöber-Bingöl et al. (5) compared between patients aged < 14, 15–40 and > 40 years, and found a marked decrease in the percentage of males from childhood to adulthood. In females, the duration of headache and the prevalence of unilateral, pulsating pain, photophobia and phonophobia increased with age, whereas the aggravation of the headaches by physical activity decreased with age. In our study an increased female ratio with age for migraine was also found, but with no statistical difference, perhaps due to different age groups in our study (Table 1).
Dizziness and aura were found to be more frequent in older children (P < 0.001). As regards dizziness and aura, we cannot determine from our data if these symptoms are differently perceived and verbally described by patients of different ages, or due to their psychological development, or if their frequency varies by age, due to continuous brain maturation.
According to Piaget (6, 7), prelogical thinking is typical of children between 2 and 6 years. It is characterized by children's inability to distance themselves from their environment, which results in their explaining cause–effect relations in terms of immediate spatial and/or temporal cues that dominate their experience. Children ≥ 11 years old manifest formal logical thinking. At this stage, there is the greatest difference between self and the other (6, 7).
The maturity of the brain influences sensory perception. Brain maturation is a continuous process, and different brain areas mature at different ages (8). Electrophysiological studies of the temporoauditory cortex have shown that the most pronounced qualitative changes occur at 6–7 years and 8–9 years old. In adolescents, the auditory event-related N1b potential reflects the contribution to visual perception by the frontal area. Whereas some frontal functions are important for learning, the automatic activation of secondary motor areas that apparently facilitates reaction times to auditory stimuli continues to decrease with age until adolescence. However, the early selection/inhibition response in the anterior cingulate might follow a different maturation trajectory and may be present already at age 6 years. These findings of continuous brain maturation may explain the heterogeneous symptoms of migraine in the paediatric age groups. Accordingly, Bender et al. (8) examined the involvement of the frontal lobe in the processing of meaningful auditory stimuli in children of different ages with and without migraine, and found no differences within the 6–18-year range.
Recent brain mapping studies have identified three major stages of pain processing: sensory transmission–discrimination, affective–motivational processing and cognitive–evaluative processing, which involve different brain areas (9, 10). These findings stress the importance of the insular, cingulate and cortical and subcortical structures and frontal brain in human pain, which may be explained by different maturation patterns (8).
Vomiting is an important factor, found to be more frequent in younger children. Generally, smaller children have a higher tendency to vomit. Emesis and migraine have a similar pathogenesis that explains the appearance of emesis during a migraine attack. It is known that emesis can be triggered by neural activity in brain regions including area postrema and nucleus tractus solitarius located in the brainstem. Substance P (SP) and its receptor, neurokinin NK1 receptor and the two serotonin receptor subtypes, 5-HT3 and 5-HT4, in the periphery and the cental nervous system, play an important role in the development mechanism of emesis (11).
Brain dysfunction triggered by activation of the trigeminovascular system is believed to be the primary pathway leading to the pain associated with all forms of vascular headache, including migraine. Neurogenic inflammation is caused by the release of neuropeptides from primary sensory nerve fibres involved in pain transmission. The trigeminal sensory C-fibres contain the neuropeptides calcitonin gene-related peptide, SP and neurokinin A. Stimulation of trigeminal nerves causes release of these neuropeptides, resulting in meningeal blood vessel dilation. Migraine sufferers appear to have a hereditary systemic perturbation of 5-HT metabolism and neurotransmission (12, 13). It seems that migraine and emesis have in common some pathophysiological causes that explain the coexistence of migraine and vomiting.
Several comparative analyses of the ICHD-I and ICHD-II have been published in recent years (14–18). Although the use of the revised classification was found to increase the diagnosis of paediatric migraine, it was still too restrictive for small children. It was also unsuitable for long follow-up in this population, as many children with partial migraine initially will meet the full criteria over time.
The present study sought to determine if any symptoms or signs of migraine are typical of specific paediatric age groups among patients who meet the ICHD-II criteria. Patients with probable migraine were excluded. No differences were found for clinical symptoms of unilateral headache, phonophobia, photophobia, awakening pain, nausea or worsening of pain during attacks. As expected, older children suffered from longer periods of migraine.
This study has shown that most clinical symptoms of migraine are not specific to specific age groups. With regard to dizziness and type of pain, we cannot determine from our data if these symptoms are differently perceived and verbally described by patients of different ages, or if their frequency varies by age.
All age groups in the present study showed a high rate of family history of migraine, with no statistically significant differences among them, indicating that a family history of migraine may be a major risk factor in children and may assist diagnosis.
Vomiting is not a verbal descriptive symptom that is statistically more frequent in younger children and, in combination with a family history of migraine, may play an important role in diagnosis.
The greater frequency of migraine in older children may be explained by the pathogenesis of transformed migraine. One risk factor is untreated migraine. None of the children referred to the headache clinic had pharmacological or non-pharmacological preventive treatment. The phenomenon of perpetuation of frequency of migraine attacks with time is well known (19).
In conclusion, most of the migraine symptoms included in the 2004 recommendations of the IHS are not typical of specific paediatric age groups, probably owing, at least in part, to the continuous maturation process of the brain. Our finding that dizziness is more common in children > 11 years old and may aid the diagnostic process in this age group. In younger children, in whom diagnosis is more difficult, a positive family history and vomiting might be considered important criteria.