
Abstract
We established a cohort of 60 subjects with chronic daily headache (CDH) out of 1533 community-based elderly in 1993 and finished two short-term follow-ups in 1995 and 1997. All of the 26 survivors without dementia (4 M/22 F, mean age 82.7 ± 3.4 years) finished the follow-up in 2006. The mean headache frequency was 8.4 ± 11.8 days per month in the past year, and seven (27±) had persistent CDH. Based on the International Classification of Headache Disorders, 2nd edn, the CDH subtypes diagnoses were chronic migraine in three subjects, chronic tension-type headache in three, and one with medication-overuse headache. All these seven subjects had CDH during the 1995 and 1997 follow-ups. The diagnosis of CDH with migrainous features increased from 25 to 71± in those with CDH from 1993 to 2006. Migraine was the most common headache type in those with CDH resolution. Aggressive treatment should be applied especially for those with persistent CDH at short-term follow-ups.
Introduction
Chronic daily or near-daily headache (CDH), defined as ≥ 15 headache-days/month for > 3 months, is the major reason that patients visit headache centres (1, 2). In 2004, the International Classification of Headache Disorders, 2nd edn (ICHD-2) (3) first adopted CDH subtypes, including chronic migraine (CM), chronic tension-type headache (CTTH), new daily-persistent headache (NDPH), hemicrania continua (HC) and medication-overuse headache (MOH). The diagnostic criteria for CM and MOH were recently revised to be more applicable to patients in clinical practices (4, 5).
The prevalence of CDH in adults was universally around 4–5% from several community-based studies (6–8). Despite a prevalence of migraine reaching a peak in the third and fourth decades of life and declining thereafter (9), we found the prevalence of CDH to be still high in the elderly (3.9%) from a large community cohort study conducted in 1993 (10, 11). In the 1995 and 1997 follow-ups, we found two-thirds of these elderly subjects with CDH continued having CDH (11). Nevertheless, the long-term outcomes, evolution of clinical features and headache diagnoses and relevant predictors for CDH persistence in the elderly remain unclear. In 2006, we again interviewed these CDH elderly to investigate the long-term outcome.
Subjects and methods
Cohort of elderly with CDH
Based on a person-to-person survey given to persons aged ≥ 65 years (n = 1533, 669 M/864 F) in a rural community of Kinmen, Taiwan, 60 subjects (3.9%) were diagnosed to have primary CDH by neurologists from our prevalence study in 1993 (11). They received follow-up examinations in June 1995 and August 1997 to assess the changes of headache profiles. The details of this cohort and initial findings have been described elsewhere (10, 11). This cohort was part of the Kinmen Neurological Disorder Survey, a comprehensive survey of neurological and psychiatric disorders including dementia, headache, essential tremor, stroke, depression and Parkinson's disease (12). About 70% of the elderly were illiterate at that time.
All participants were administered a Chinese version of the Geriatric Depression Scale-Short Form (GDS-S) in 1993. The GDS-S, consisting of 15 items of the original scale, was developed to reduce the fatigue and the effects of deteriorated concentration of older individuals (13). Scores on the GDS-S showed a high correlation with that on the original form, and scores of ≥ 8 on the GDS-S are associated with a clinical diagnosis of depression (14, 15).
Follow-up in 2006
The elderly subjects with CDH were followed up in 2006 by neurologists using a semistructured interview, which was the same as that used in three previous surveys except for minor modifications for the new ICHD-2 criteria. The participants were asked about their headaches within the previous year, including the frequency, severity, characteristics, location, duration, accompanying symptoms, painkiller use, functional impairment due to headache and mood. The subjects rated their functional impairment due to headache on a four-point Likert scale: no, mild, moderate and severe impairment. The subjects also self-reported their mood on a five-point Likert scale: very good, good, average, bad and very bad. The study protocol was approved by the Institutional Review Board of the Kaohsiung Medical University Hospital. A consent form was obtained from the subjects before entering the study.
Headache diagnoses
CDH was diagnosed when the subject had ≥ 15 headache-days/month, average ≥ 4 h/day for > 3 months. Of note, the duration of diagnosis of CDH in the baseline study (1993) was 6 months. For purposes of comparison, our original classifications of CDH in 1995 was used, i.e. three mutually exclusive categories: CTTH; CDH with migrainous features (CDH/MF); and other CDH. For future comparisons, we also followed the ICHD-2 (3) and the most updated appendix criteria (5) to classify CDH subtypes, i.e. CM, CTTH, NDPH, HC and MOH. Notably, the appendix criteria define CM (code A1.5.1) as headache on ≥ 15 days and, of them, migraine ≥ 8 days per month for ≥ 3 months, and recommend that the MOH diagnosis (code A8.2) should no longer request improvement after discontinuation of overused medications, but should be given to patients if they have a primary headache plus ongoing medication overuse (5).
Statistical methods
SPSS Version 11.0 for Windows (SPSS Inc., Chicago, IL, USA) was used for statistical analysis. Means were compared using the unpaired t-test, and proportions were compared using the χ2 or Fisher's exact tests, when appropriate. Hazard ratios (HR) and 95% confidence intervals (CIs) for CDH persistence in 2006 and mortality were estimated utilizing Cox proportional hazard models without adjustment. All P-values were two-tailed, and statistical significance was defined as a P-value < 0.05.
Results
Participants
Of the 60 elderly subjects with CDH in the baseline study, 29 (48%, 4 M/25 F, mean age 83.7 ± 5.1 years, range 78–99 years) survived in 2006 and all of them received the follow-up study. The causes of death listed on the official death certificates of the 31 subjects who had died before 2006 were stroke (n = 5), uraemia (n = 2), malignancy (n = 3), myocardial infarction (n = 1), diabetes (n = 1), infection (n = 3), dementia (n = 2) and unknown cardiopulmonary failure (n = 14). Compared with the survivors, the deceased were older (baseline age 77.1 ± 8.0 vs. 70.7 ± 5.1 years, t-test P < 0.001). Women (52.1 vs. 33.3%, P = 0.245), those who overused medication at baseline (66.7 vs. 42.2%, P = 0.101) and those with aura (66.7 vs. 47.4%, P = 0.514) were non-significantly more likely to survive when compared with their counterparts. Those who had active migraine at baseline had similar survival rates to those without active migraine (50.0 vs. 47.8%, P = 0.887). The subjects with GDS-S score ≥ 8 at baseline were more likely to have died compared with those with a GDS-S score < 8 (64.7 vs. 43.9%, P = 0.149). Cox proportional hazard models, unadjusted for covariates, showed that only the baseline geriatric depression score ≥ 8 was a significant predictor of death (HR 2.3, 95% CI 1.1, 4.9; P = 0.03).
Evolution of headache frequency and diagnoses at the 2006 follow-up
Of the 29 survivors, three (10%) had dementia and two (7%) stroke in the 2006 follow-up. The demented subjects were excluded from analysis because they could not provide a reliable headache history. The final sample thus consisted of 26 persons (4 M/22 F, mean age 82.7 ± 3.4 years, range 78–90 years). At the 2006 follow-up, the mean headache days per month were 8.4 ± 11.8 days. Nine elderly (35%, 2 M/7 F) reported no headache in the past year.
Seventeen elderly (65%) had headache ≥ 1 day per month and seven (all women) (27%) had CDH, including five with daily headache. Notably, all these seven women also had CDH back during the 1995 and 1997 follow-ups. Among those whose CDH disappeared in these two early follow-ups, none had developed CDH in 2006. None of these seven subjects had medication overuse at baseline. Age did not differ between the subjects with or without persistent CDH (83.1 ± 4.3 vs. 82.5 ± 3.1 years, t-test P = 0.66).
Table 1 presents baseline (1993) and 1995, 1997 and 2006 follow-up results. Of note, the percentage of CDH/MF increased and became the most common CDH diagnosis in 2006, whereas that of CTTH declined. Table 2 shows the diagnostic changes in 2006 based on the current ICHD-2 diagnostic criteria. Overall, three subjects (38%) had CM, three (38%) CTTH and one MOH. Of note, one subject with CTTH also had episodic probable migraine attacks, and the subject with MOH had migraine without aura > 8 days per month. Among those without CDH in 2006, the most common headache diagnoses were migraine with or without aura (n = 5, 50%), followed by episodic tension-type headache (n = 3, 30%). Throughout all these years of follow-up, 16 of the 26 participants (62%) had a current or past history of migraine.
Follow-up results of subjects with chronic daily headache (CDH) diagnosed in 1993
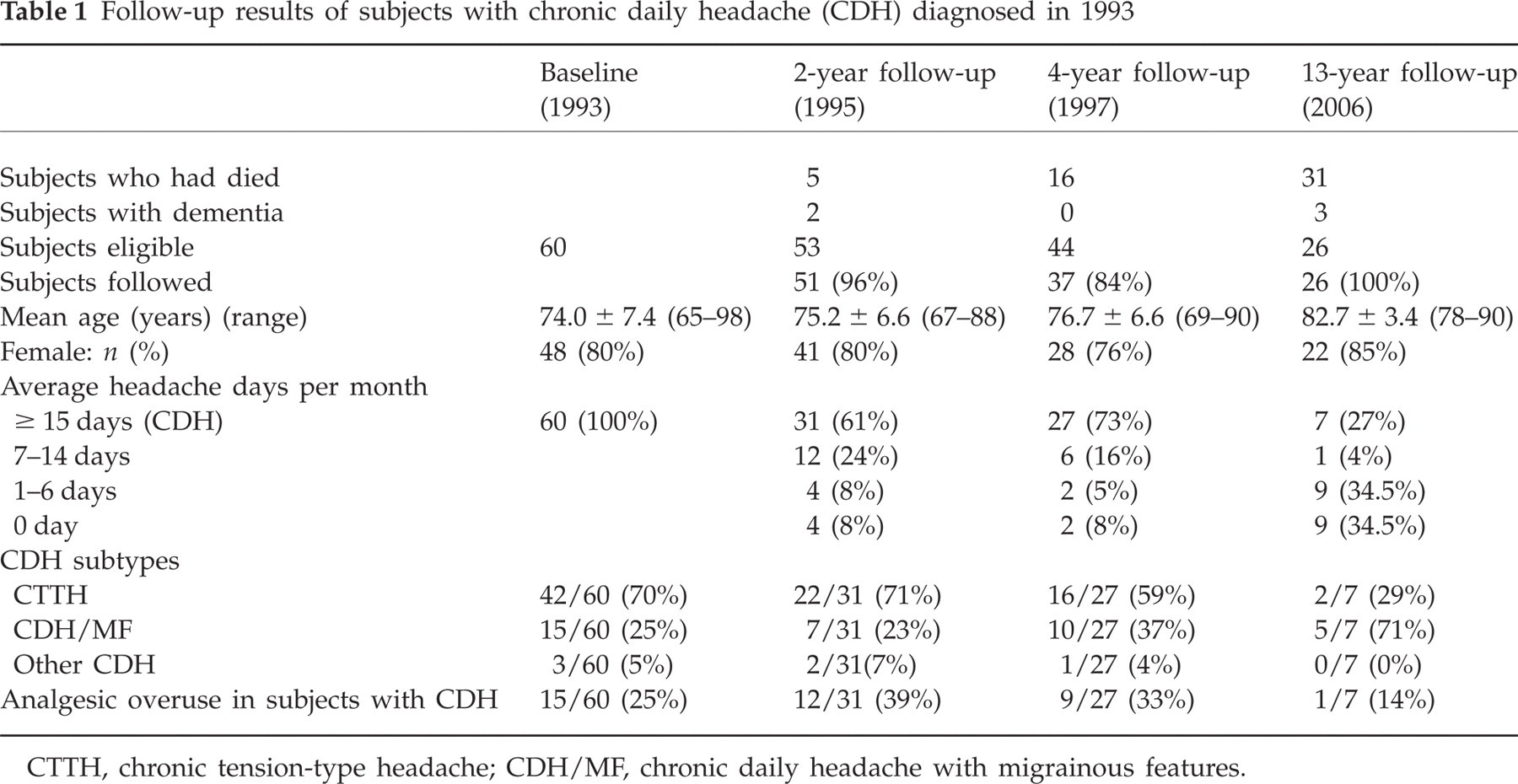
CTTH, chronic tension-type headache; CDH/MF, chronic daily headache with migrainous features.
Evolution of headache diagnoses from baseline (1993) to 2006
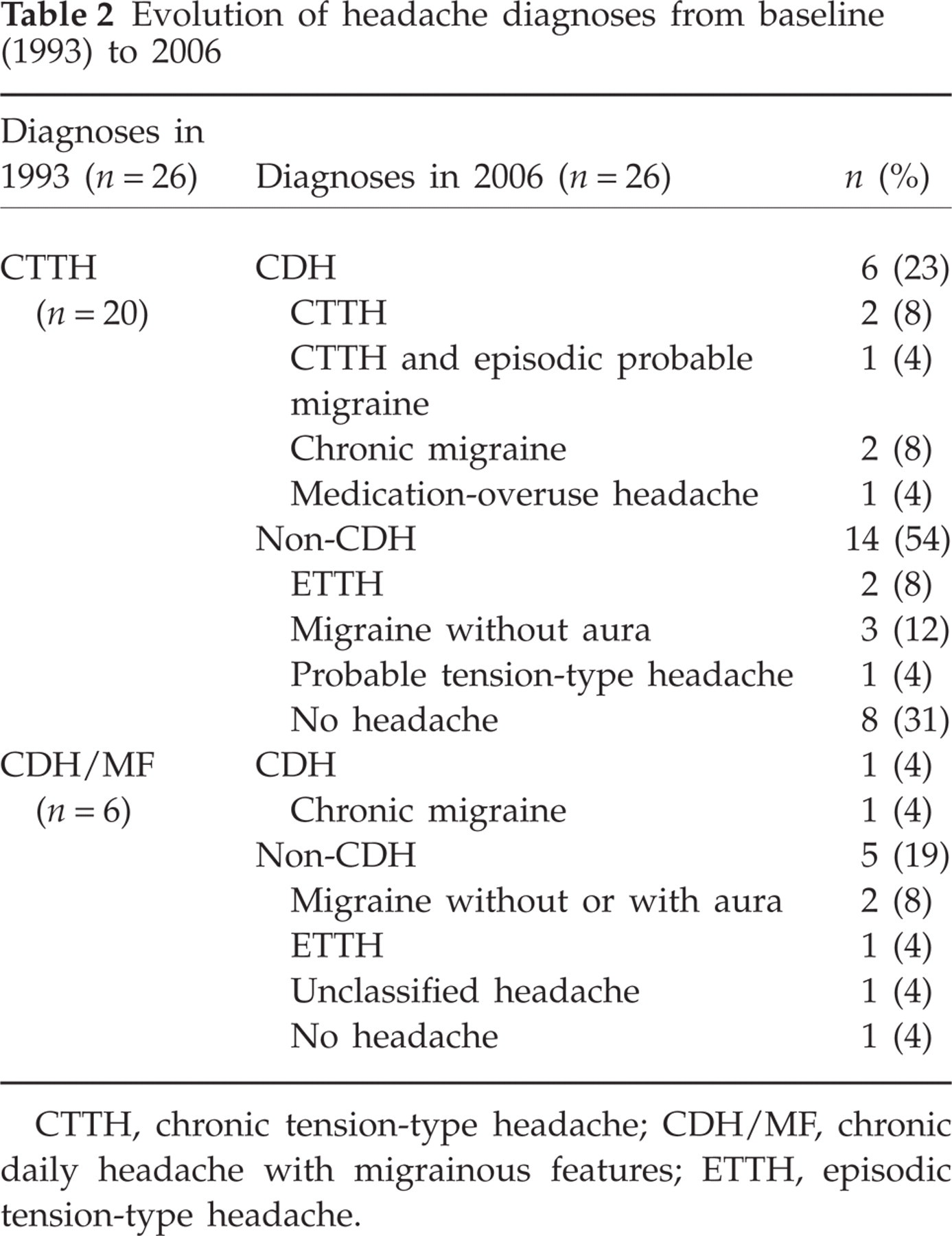
CTTH, chronic tension-type headache; CDH/MF, chronic daily headache with migrainous features; ETTH, episodic tension-type headache.
Figure 1 shows the evolution of the frequencies of migrainous features in the 26 CDH survivors in 1993 and 2006. Of note, only 17 of them had headaches in the 2006 follow-up. The frequencies of throbbing, photophobia and phonophobia were markedly increased at this follow-up survey.

The frequencies of migrainous features at baseline (1993) and 13-year (2006) follow-up.
Painkiller usage
In 2006, 11 (65%) subjects had taken medications for their headache in the past year. Nine of them (82%) took over-the-counter painkillers, one prescribed medication, and only one was on preventive medications. One patient fulfilled the criteria of MOH.
Mood and functional impairment
The seven subjects with persistent CDH reported their moods as: very bad (14%), bad (29%) and average (57%). All three subjects reporting very bad or bad moods were diagnosed as CM. In contrast, subjects without CDH reported their moods as: very good (37%), good (37%) and average (26%). Four of the seven (57%) subjects with persistent CDH reported severe functional impairment caused by their headaches.
Prognostic factors for persistent CDH at the 13-year follow-up
Univariate Cox proportional hazard models showed that none of the following variables predicted persistent CDH in 2006: female gender (HR 42.6, 95% CI 0.3, 59 443.2; P = 0.310), medication overuse at baseline (HR 1.8, 95% CI 0.4, 8.0; P = 0.453), life-time migraine history (HR 0.5, 95% CI 0.1, 4.6; P = 0.579), CDH/MF (HR 1.4, 95% CI 0.1, 22.0; P = 0.824) and baseline geriatric depression score ≥ 8 (HR 0.6, 95% CI 0.1, 5.2; P = 0.651).
Discussion
To our knowledge, this is the first study to examine the long-term (13 years) outcome of elderly subjects with CDH in a community setting. Many of them continued suffering from frequent headaches with a mean frequency of 8.4 days per month. About one-quarter had persistent CDH. Of note, in the 1995 and 1997 (2- and 4-year) follow-ups, a high proportion (two-thirds) of this cohort had persistent CDH. Therefore, CDH in the elderly might have a relatively grave prognosis compared with the studies done in other age groups. Their persistence rates ranged from 25 to 42% in 1- or 2-year follow-ups (7, 16–18).
The proportion of CDH/MF among participants increased from 25% at baseline to 71% at the 2006 follow-up. In contrast, the proportion of CTTH decreased from 70 to 29%. It has been known that migraine is the major headache type before transformation to CDH (1, 19, 20). Intriguingly, our study has shown similar findings, but in a reverse direction, i.e. migraine became the most common headache type and migraine features became more prominent when CDH had resolved. In fact, this finding was also noted in the follow-up survey of our adolescent cohort with CDH (18). In addition, we also found 30% of patients with CTTH in 1993 evolved to CM or episodic migraine. Therefore, in some patients with CDH, CTTH and CDH/MF might represent different phenotypic diagnoses at different times of survey. Migraine history could be traced or diagnosed in about two-thirds of our elderly subjects with CDH and is the most important headache type in relation to elderly CDH.
Medication overuse at baseline was a risk factor for persistent CDH for short-term (1995, 1997) but not long-term (2006) prognosis. In fact, medication overuse declined from 25% in 1993 to 14% in 2006 among those with CDH. None of the seven subjects with long-term persistent CDH had medication overuse at baseline. In contrast, all had CDH at the 2- and 4-year follow-up surveys. It indicates that around one-quarter of elderly CDH sufferers who ran a rather protracted course were not associated with medication overuse. It is unknown if early intervention in this group of patients might halt the grave prognosis.
As the 2- and 4-year follow-up results showed (11), subjects with persistent CDH had lower mood level scores in comparison with those without at this long-term follow-up survey. This is a universal finding in patients with CDH in clinic- or community-based studies (7, 11, 16, 21). However, high depression scores in our CDH elderly at baseline failed to predict persistent CDH at either short- or long-term follow-ups. Therefore, in the elderly, depression was more likely to be a reactive condition in response to the occurrence of CDH than a phenomenon of ‘shared mechanisms’. Life interference caused by chronic pain has been considered as an important factor in depression in the elderly (15, 22). In contrast, our previous study done in adolescents showed that the presence of major depression could predict persistent CDH (18). These findings suggest that co-morbidity of depression occurs in every age group with CDH, but their underlying mechanisms might differ.
The strengths of this study are the rarity of long-term outcome studies in the elderly with CDH in the community, a high follow-up rate and ascertainment of headache diagnoses by neurologists. The potential reporting error is thus minimized. Its limitations are (i) the change of the definitions of CDH. In the baseline survey, we defined CDH as ≥ 15 headache-days/month for > 6 months rather than > 3 months in the 2006 survey, and (ii) the low number of survivors/cases at follow-up. Type II errors were inevitable when calculating the significant risk factors for mortality or prognosis. In addition, selective mortality is an important issue, because only half of this elderly cohort survived. However, we did not find any headache features (migraine or aura) in relation to mortality. As in previous studies done in community-dwelling older populations (23, 24), we found high levels of depressive symptoms also increased the risk of mortality in our CDH cohort. The differential survival rates between CDH elderly with and without depression might downplay the impact of depression on the long-term outcome of CDH persistence.
Competing interests
None to declare.