
Abstract

In cerebral autosomal dominant arteriopathy with subcortical infarcts and leucoencephalopathy (CADASIL), one-fifth to one-third of patients have migraine with aura (MA), and this is often the first symptom of CADASIL (1–3). In one German CADASIL family, all had migraine and dementia (4); and in an Italian family dominant MA was associated with the Notch 3 mutation (5). MA can precede the onset of stroke by a mean of 7 (1) to 15 years (6). The aura symptoms are atypical in approximately half of the attacks (6). The frequency of migraine attacks is variable, from two per week to one every 3 or 4 years or less (6).
We describe here a patient with a prolonged aphasic aura who later with genomic testing was diagnosed as suffering from CADASIL. Single-photon emission computed tomography (SPECT) examination of cerebral blood flow on the fifth day of the attack showed the typical delayed hyperperfusion seen in MA (7).
Case history
A 45-year-old man was admitted on 5 May 2006 on the third day of a severe attack of MA. He was severely aphasic. He could not cooperate with neurological examination and said only ‘yes or no’ and ‘I have a headache’. Computed tomography (CT) showed multiple periventricular hypodensities. Spinal fluid was normal apart from a protein of 0.73 g/l, and there were no monoclonal bands.
The next day he was still aphasic and disorientated. On the third day of admission (fifth day of attack) he had improved but could not tell the year or remember his social security number. SPECT examination with 99mTc-exametazime (Ceretec) demonstrated increased blood flow in most of the left hemisphere (Table 1), especially in the temporal and occipital lobes (see Fig. 1a). SPECT examination 6 weeks later showed normal distribution of the cerebral blood flow (Fig. 1b, Table 1).
Differences in relative cerebral blood flow measured with 99mTc-exametazine (Ceretec) between left and right hemispheres, subdivided into the vascular territories of the anterior, middle and posterior arteries

The percentages shown are counts in the left region of interest, divided by counts in the corresponding right region of interest.

Single photon emission computed tomographic examinations with Ceretec of a CADASIL patient after an attack of an aphasic aura of 4 days duration and a control examination 6 weeks later. Note hyperaemia in the whole left hemisphere. The hyperaemia was most pronounced in the temporal and occipital lobes.
He had suffered from MA since the age of 20 years. Attacks reportedly started with half-sided, pulsating headache and then a sensory, paraesthetic aura involving the arm and the leg on alternating sides, lasting half an hour. The patient suffered from photophobia, but denied flickering light or scotomas. He twice had aphasia during attacks. The patient treated his attacks with paracetamol and bed rest. Attacks occurred every 3 months and the headache could last from some hours to 2 days.
There was no history of early strokes or MA in the family. He was number 5 of five siblings.
In 2002 he had developed a bulbar palsy and a paresis of the right upper extremity and was treated with intravenous corticosteroids at another clinic. He made a full recovery.
In 2004 he was submitted to a psychiatric ward for a psychotic disorder and was subsequently treated with olanzapine for 1 year.
In December 2006 he was admitted again to our department, this time for cognitive deterioration during 1 week. The patient was quite indifferent concerning his symptoms, despite evident difficulties in orientation in place and time. Magnetic resonance imaging (MRI) showed multiple hyperintensive subcortical lesions on T2-weighted images, but no cortical infarcts (Fig. 2). There were more lesions than 4 years previously. Neuropsychological examination 10 days later showed decreased concentration, severe memory problems and severe difficulties in the use of words. Spinal fluid examination was normal without oligoclonal bands. A genetic test showed a Notch 3 mutation (R110C (c328C→T)) diagnostic for CADASIL.
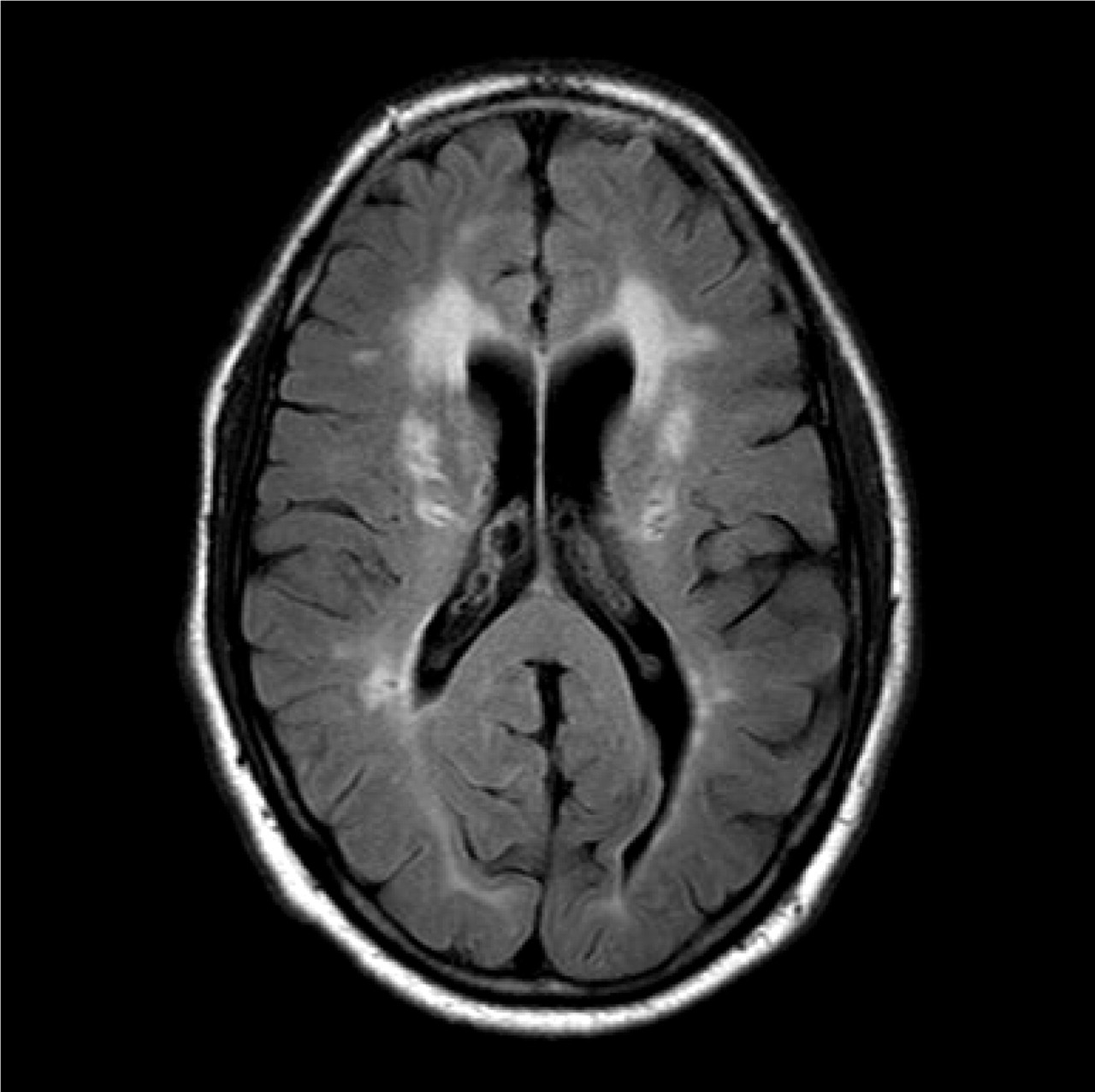
Magnetic resonance imaging with fluid attenuated inversion recovery sequence of the CADASIL patient. Note subcortical lesions in the corona radiata. No cortical infarcts were observed.
Two months later he was marginally better on neuropsychological examination and started working again part-time as a printer. Five months later he still had memory problems, but was working full time.
Discussion
Clinically, the patient had the whole spectrum of CADASIL (1, 2, 3, 6): MA, a stroke event at age 40 years, a psychotic episode, an atypical prolonged migraine aura and an episode with acute cognitive decline, which led to the diagnosis.
SPECT has been used in CADASIL patients outside of attacks of migraine or stroke. In some cases frontal and temporal hypoperfusion were found (4). In one study with positron emission tomography, frontal and occipital white matter blood flow were decreased (8). The present case is, to our knowledge, the first SPECT study in connection with MA in a CADASIL patient.
Hyperperfusion can be present days after cortical infarction (9). In the present case the patient could clinically have suffered a minor stroke, but the CT scan and later MRI showed no cortical infarct. Furthermore, the hyperperfusion was seen in most of the hemisphere and thus in a much larger area than that responsible for the aphasia. The hyperperfusion was not compatible with a subcortical infarct, where a focal decrease in cerebral blood flow would be expected (10, 11).
Delayed hyperperfusion, up to 24 h after the start of aura, has been described in MA after an initial hypoperfusion (7, 12). It has been suggested that the severity of symptoms of the aura determines the duration, extent and severity of the delayed hyperperfusion (12, 13). In our case, the patient was aphasic for at least 4 days, an unusually long aura, and SPECT examination was done on the fifth day. This may explain why the hyperperfusion was still present at the SPECT examination done on the fifth day. The delayed hyperperfusion found in our case indicates that the mechanism of MA is basically the same in CADASIL patients as in primary MA. Thus, in both cases the underlying mechanism is probably cortical spreading depression (CSD) (14). Why CADASIL patients with a subcortical disorder develop CSD remains uncertain. However, since CADASIL is a disease affecting arterioles and small arteries, it seems likely that borderline ischaemia in a cortical area may be the event triggering CSD. Thus, in cases of miserly perfusion caused by carotid artery dissection, a flurry of migraine auras has been observed (15). Against this hypothesis it may, however, be argued that migraine often precedes cerebral infarction and the migraine often disappears as stroke lesions become pronounced in later stages of the disease.
CSD alters blood–brain barrier permeability in rats by activation of metalloproteinase-9 (16). This effect is observed after 3–6 h, reaches a maximum after 24 h and is persistent for ≥ 48 h (16). Such mechanisms added to perfusion problems or, alternatively, repeated waves of CSD may perhaps explain the long-lasting aura in our patient.
Repeated regional blood flow measurements covering also the early phases of attacks are needed to explore further the regional cerebral blood flow changes in migraine aura in CADASIL patients.