
Abstract
Cortical spreading depression (CSD) is supposed to be the underlying biological basis of the migraine aura. Metoprolol was proven to be effective in migraine prophylaxis in clinical trials, but its mechanism of action has not been clarified yet. We studied direct effects of metoprolol on a continuous CSD induction model in rats. Six adult Wistar rats were anaesthetized with intraperitoneal thiopental (50 mg/kg). CSD was induced with application of 1 M KCL through a burr hole into the left frontal dura-mater, and recorded by an Ag/AgCl DC electrode on the left parietal dura-mater. After a basal recording of CSD induction during the first 40-min period, metoprolol (5 mg/kg) was infused within 4 min. Then DC recordings were maintained for a further 120 min. Any significant differences in total number and duration of CSDs before and after metoprolol administration were not detected. This study suggests that the mode of action of metoprolol in prophylaxis is not via direct CSD inhibition.
Introduction
The term ‘migraine aura’ refers to completely reversible neurological symptoms of focal, cortical or brain stem dysfunction that develop over more than 4 min and last for less than 60 min. Aura is supposed to trigger the activation of the trigeminovascular system, and CSD is supposed to be the physiological basis of the aura (1, 2). CSD waves are slow negative extracellular potential shifts (10–20 mV) associated with massive trans-membranous ion exchange resulting in intracellular increase of water. These waves exist in a manner that obeys an all-or-none rule.
A prophylactic antimigraine drug must decrease the number of CSD waves, if its prophylactic effect is related to CSD inhibition. The direct CSD blocker effects of topiramate and magnesium, which are also commonly used in migraine prophylaxis, have been shown in previous studies supporting this hypothesis (3, 4). Metoprolol, a selective blocker of the beta 1-adrenoreceptors, was proven to be effective in migraine prophylaxis in clinical trials, but its mechanism of action in this situation has not been clarified yet (5, 6). We investigated the influence of metoprolol with its acute effects in rat brains on generation or duration of CSD waves. As the acute effects of metoprolol administration on CSD were investigated in this study, the duration of DC recordings was much longer than the time necessary for the distribution of metoprolol into the brain tissue and cerebrospinal fluid from plasma (7).
Methods
Drugs
Metoprolol tartarate, thiopental sodium and saline solutions were purchased from the hospital pharmacy. Metoprolol tartarate was manufactured by Eczacıba ı in Istanbul (licensed by AstraZeneca), thiopentoal sodium by IE Ulagay in Istanbul, and saline by Biosel in Istanbul; 1
Surgical procedures
All experiments were conducted under the approval of Kocaeli University Ethics Committee. Six male Wistar rats (250–300 g) were anaesthetized using sodium thiopental with an initial dosage of 50 mg/kg intraperitoneally. All rats were kept anaesthetized during the whole experimental period by means of additional thiopental dosages (5 mg/kg, i.p.), which were administrated according to tail pinch reaction. The right femoral vein was cannulated for drug infusion. Body temperature was monitored continuously with a rectal probe during the experiment.
The rats were placed in a stereotaxic frame. The scalp was retracted laterally following a median incision, and the skull was exposed. One burr hole with diameter of 2 mm was drilled over the left frontal cortex (2 mm anterior and laterally to the bregma) by use of a mini-drill. The dura mater was kept intact. A second hole was drilled over the left parietal cortex (2 mm posterior and 2 mm laterally to the bregma; 2 mm dia; dura intact). An Ag/AgCl pellet electrode (1 mm dia, World Precision Instruments, Sarasota, FL, USA), which was embedded in polyethylene tubes of 20 mm length and 1 mm diameter filled with 0.9% NaCl in agar, was positioned on the dura over the parietal cortex to measure the direct current (DC) potential. A bare Ag/AgCl electrode placed in the neck served as a reference. After surgical preparation, the cortex was allowed to recover for 30 min. The data were continuously recorded using a data acquisition system (BIOPAC System, Inc., Goleta, CA, USA) for off-line analysis.
One of the animals was chronically implanted with standard tripolar ECoG electrodes (MS333/2 A; Plastic One, USA) over the frontal and parietal cortex 1 week before the experiment for simultaneous ECoG recordings. To test the reliability of the model, this animal was injected with ketamine (which was used as a reference substance that reliably blocks CSD) after the whole experimental procedure and recordings.
Experimental protocols
Continuous CSD induction was elicited by application of a 3-µl drop of KCl (1
Data analysis
All data are reported as mean ±
Results
Application of KCL to the frontal dural surface induced repetitive negative deflection in DC potential (amplitudes >1 mV) in all rats. Every DC potential shift was accompanied by a transient decrease in ECoG amplitude in reference animals. A typical ECoG and DC patterns are shown in Figure 1. Blockage of CSDs after ketamine injection was also observed in this rat at the end of experiment, revealing the reliability of the CSD model. No toxic effect was determined after metoprolol administration during the procedures.
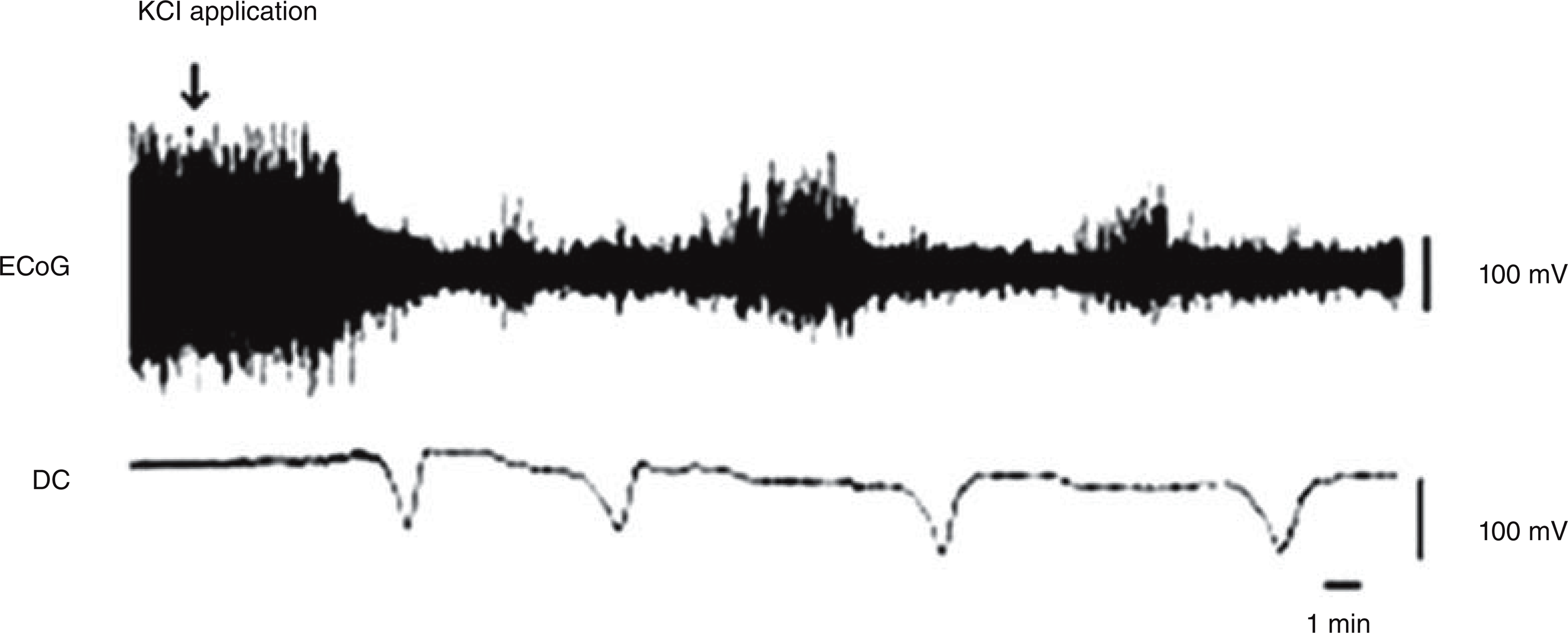
Simultaneous ECoG and DC recordings during continuous CSD induction.
The mean numbers of CSDs was 7.6 ± 0.4 and mean duration of CSDs was 118.7 ± 4.6 s during the baseline 40-min recordings. After metoprolol administration, the mean numbers of CSDs was 8.5 ± 1.3 and mean duration of CSDs was 117.9 ± 5 s during the first 40-min period, 8.5 ± 1.4 and 119.3 ± 4.2 during the second 40-min period, and 8.3 ± 1.2 and 117.2 ± 6.3 during the third 40-min period, respectively. Therefore metoprolol administration did not reduce or block the generation of CSDs. It also did not change duration of CSD waves significantly. Figure 2 shows number and duration of CSDs before and after administration of metoprolol.

The number and duration of CSDs did not change significantly after treatment with metoprolol compared with baseline levels (Kruskal–Wallis test did not reveal any significant differences).
Discussion
We investigated the acute effect of metoprolol on CSD by use of DC recordings on a continuous CSD induction model in rats, and revealed that metoprolol administration has no significant effect on generation or duration of CSD waves. Our findings are consistent with the study by Kaube & Goadsby (8), which investigated the effects of metoprolol on CSD with another method. They also revealed metoprolol and some other prophylactics (dihydroergotamine, acetylsalicylic acid, lignocaine, clonazepam and valproate) to fail in blocking CSD by measuring cortical blood flow with laser Doppler flowmetry and cortical single unit activity in cats.
Considering the results of this study and ours, as metoprolol was found to be ineffective in blocking the generation or duration of CSD on different animal species with different methods, it could be stated that there must be another mechanism of action of it rather than acute inhibition of CSD in brain tissue. In support of this view, Shields and Goadsby (11) reported that the preventive action of propranolol, a non-selective blocker of the beta adrenoreceptors, is partially mediated by B1 adrenoreceptor inhibition of activation of third order trigeminovascular nociceptive neurones.
Recently, Ayata and his colleagues (12) reported that chronic application of prophylactic drugs could have modulating effects on CSD generation in contrast to acute application. They reported another beta adrenoreceptor blocker, propronalol, to reduce CSD numbers with chronic drug application, but not with acute application. Considering acute systemic administration of metoprolol did not modulate CSD induction or duration even after the distribution into the brain tissue and cerebrospinal fluid from plasma in our study, it could be possible that the beta adrenoreceptor blockers have chronic modulating effects on the central nervous system, that is, indirectly effect the generation of CSD.
In conclusion, our study revealed that acute systemic metoprolol application is not effective on CSD. It seems that metoprolol is not a direct CSD blocker in the central nervous system. This is consistent with metoprolol being used in preventive therapy of migraine, but not in aborting migraine attacks. Possibly in the long term, with its indirect effects, the brain becomes more resistant to generation of CSD, but this issue must be clarified with further studies.