
Abstract
The aim was to analyse the socioeconomic burden of cluster headache in patients from a tertiary headache centre. One hundred consecutive patients from the Danish Headache Centre were invited to an interview about the socioeconomic impact of cluster headache. Work absence and use of medical services were compared with a Danish population-based survey. Eighty-five patients participated; 78% reported restrictions in daily living and 13% also outside of cluster periods; 25% reported a major decrease in their ability to participate in social activities, family life and housework. The disease caused lifestyle changes for 96%, most frequently in sleeping habits and avoidance of alcohol. The absence rate among patients was 30%, which was significantly higher than 12% among the general population (P < 0.001). Use of health services due to headache was also higher among the patients (P < 0.001). Cluster headache, although periodic in most cases, has considerable impact on social functions, quality of life and use of healthcare.
Introduction
Cluster headache is a primary headache characterized by recurrent, severe, short-lasting headaches associated with autonomic features, occurring in episodic and chronic subforms. Cluster headache is relatively rare compared with other primary headaches, with an estimated prevalence of around 1 per 1000. It has a clear male preponderance with a male:female ratio of 4–5 : 1 (1, 2).
Few socioeconomic data are available on cluster headache. The severity of the attacks predicts considerable occupational and social disabilities during attack phases, but little is known about the total impact of the cluster episodes and physical and social functioning outside of clusters.
Ertsey et al. found lower health-related quality of life scores using the Short Form (SF)-36 among patients with episodic cluster headache compared with healthy controls during cluster episodes (3). Similar findings have been published by D'Amico et al., who also included patients with chronic cluster headache (4). Using the SF-20, Solomon et al. found higher pain scores and a higher percentage of patients with poor health due to pain and social functioning among patients with cluster headache than among migraineurs (5).
The objective of this study was to analyse the impact of cluster headache on social functioning, work ability, sickness absence and utilization of medical and non-medical services among patients from a tertiary headache centre. Data on work absence and use of medical services were compared with data obtained in a recent population-based cross-sectional survey of primary headaches (6–8).
Materials and methods
Our clinical study population comprised 100 randomly chosen patients with the initial diagnosis of cluster headache seen at the Department of Neurology, Glostrup Hospital and the Danish Headache Centre between October 1998 and September 2003.
All clinical standardized records underwent audit. The patients who fulfilled the International Headache Society diagnostic criteria for cluster headache were contacted by telephone and offered a semistructured telephone interview, which contained 97 questions about headache characteristics and the socioeconomic impact of headache disorders derived from a recent general population study (6–8), slightly modified to gain additional information about cluster headache. The interview included an extensive description of the headache history, including headache frequency, duration and location, accompanying symptoms, onset of headache, familial occurrence, and influence on working ability, utilization of health services and medicine. All interviews were carried out by the same investigator, a neurologist trained in headache diagnostics (R.M.J.). Patients who refused to participate in the telephone interview, could not be reached by telephone, did not respond to a posted invitation letter or who after the interview failed to fulfil the International Classification of Headache Disorders (ICHD) criteria of 3.1, cluster headache, or 3.4.1, probable cluster headache, were excluded from the study.
If the information given in the interview differed from that in the hospital chart, the answer given in the interview was considered as the most accurate. Data were loaded in a Microsoft Access 2003 database. The patients were primarily diagnosed according to ICHD-I, but data allowed a subsequent reclassification to ICHD-II (9).
The population survey was conducted between May 2001 and April 2002 and comprised subjects from the general population identified through the Danish Civil Registration System. All eligible subjects were invited to a medical interview and a general examination with emphasis on primary headaches. The headache diagnoses were assessed by a medical doctor and based on ICHD-I and ICHD-II. Further details of methods and results from this large epidemiological study are presented elsewhere (6–8).
Data analyses and statistics
Healthcare utilization is presented as consultations with general practitioners, specialist care (out-patient and private specialty clinic care), hospital admissions and off-hour service (general practitioners on off-hour duty or emergency department). Absence rates (at least one absence day from work or school within the last year) and number of days off work were analysed among gainfully employed subjects, i.e. subjects with paid work, apprenticeship or under education in the preceding year. Mean, median and range values are presented. Otherwise, statistical analyses were made using the χ2 test and Wilcoxon paired sample test. The level of significance was chosen as P < 0.05. All data analyses were carried out using the SPSS statistical package, version 12.0 (SPSS Inc., Chicago, IL, USA) and SAS statistical package, version 9.1 (SAS Inc., Cary, NC, USA).
General population
The population survey comprised 848 subjects (422 males and 426 females) aged 25–76 years representative of the Danish background population in age and gender distribution. The subjects had migraine, tension-type headache or coexisting headaches as published elsewhere (6–8). Only one subject in the cohort was diagnosed with cluster headache.
Results
Clinical patient population
Of the 100 patients originally drawn from the patient register with the initial diagnosis of cluster headache, 95 (65 male and 30 female) fulfilled the IHCD-II criteria of 3.1, cluster headache, or 3.4.1, probable cluster headache (9). The remaining five patients had migraine with (n = 1) or without aura (n = 1) or unclassifiable headache associated with sinus or systemic disease (n = 3).
Three patients refused to participate in the structured telephone interview and seven could not be reached by telephone and did not respond to a posted invitation letter.
In total, 85 patients (56 male and 29 female) were included in the study. Patient characteristics are shown in Table 1.
Patient characteristics

Mean values are indicated with range in parentheses.
One patient had undetermined periodicity.
CH, Cluster headache; ICHD, International Classification of Headache Disorders.
Eighty-eight percent (75 patients) fulfilled the criteria of definite cluster headache (1, 3). Of these, 79% (59/75) had episodic cluster headache (ICHD 3.1.1) and 20% (15/75) had chronic cluster headache (ICHD 3.1.2). One patient had undetermined periodicity as he had experienced only one cluster episode.
Twelve percent (10/85) were classified as probable cluster headache (ICHD 3.1.4), eight of these because of attacks lasting >180 min, one because of lack of autonomic symptoms and one because he had cluster attacks only during airplane takeoff or landing (airplane headache). The distribution of patients between episodic and chronic cluster headache is illustrated in Fig. 1 and further details about the clinical presentation will be presented in a subsequent publication.

Classification according to the International Classification of Headache Disorders, 2nd edition (7).
Daily living in the clinical population
Seventy-eight percent (66/85) of the patients reported restrictions in their daily living because of their cluster headache and 13% (11/85) reported inhibition also outside of cluster periods. The reported impact of cluster headache on working and social abilities is shown in Table 2. During clusters more than 25% reported decreased ability to participate in social activities, family life and house work to less than one-third of normal activity.
Reported impact of cluster headache on working and social ability

Values are presented as percentage values.
In total, the disease had caused lifestyle changes for 96% (82/85) of the patients during the last decade (Fig. 2). The greatest impact was seen on sleeping habits and avoidance of alcohol. Likewise, many patients reported cessation of a range of social or leisure activities and dependence on help from family and friends during cluster periods. Only few patients had changed their diet or smoking habits or lived alone because of their cluster headache.

Reports of lifestyle changes due to cluster headache.
Impact on work in the clinical population
Sixty-four percent (54/85) of the patients were currently gainfully employed and 92% (78/85) had worked during a cluster period, but 82% (63/77) reported decreased work ability during these periods. Half of the patients considered the decreased working ability as minor or moderate, whereas the other half considered it as profound (Table 2). The reported effects on work are shown in Fig. 3a,b. When asked to quantify their work efficiency, 38% (27/72) felt no or very few restrictions in their work efficiency, either because they had very effective and reliable treatment for the headaches or because most attacks occurred during night time and did not affect their daytime condition, whereas 38% (28/72) considered their work efficiency to be <60% of normal during a cluster (Fig. 3a).

(a) Reported work efficiency during a cluster period. (b) Reports of work changes due to cluster headache.
One-third of the patients felt that the cluster headache had limited their career and a similar proportion had changed their work pattern because of the disease, e.g. by changing their working hours or by working from home.
Sixteen percent (14/85) of the patients had lost a job within the last decade and 8% (7/85) had had early retirement because of their cluster headache.
Absence from work in the clinical population
The reported work absences are shown in Table 3. During the last year, 29.6% (16/54) of gainfully employed patients had been absent from work at least once because of cluster headache, which was significantly higher than among the general population, where the headache-related absence rate was 12.3% (P < 0001). The absence rate due to causes other than headache was not statistically different between the groups.
Work absence among gainfully employed subjects reported by cluster patients and by subjects in a general population

P < 0.001. NS, Not significant.
The median number of days off work within the last year because of headache was 0 days (range 0–150) among the cluster patients, with no significant difference between episodic and chronic patients, and 0 days (range 0–41) in the general population. The mean number of days off work due to cluster headache was 9 days. Statistically the number of absence days due to headache was significantly larger among the cluster patients (P < 0.001). The number of absence days due to other causes was similar between the two groups.
Use of medical services
The reported use of medical services is illustrated in Table 4. Almost all the cluster patients had at some time contacted their general practitioner (GP) because of their cluster headache, a third of the patients within the last year. This covers both face-to-face consultations and telephone calls concerning renewal of medicine prescriptions, etc. The use of specialists and off-hour services was significantly higher among cluster patients compared with the general population (P < 0.001). Among patients who had been in contact with another specialist due to cluster headache within the last year, 91.8% had had visits in the Danish Headache Centre; 44.7% (38/85) of the cluster patients had previously been admitted to hospital due to cluster headache, but after being treated in the Headache Centre only one patient had been admitted during the last year, similar to the admission rate in the general population.
Use of medical services for headache by cluster headache patients and by subjects in a general population

Values are presented as percentage values.
P < 0.01;
P < 0.001. NS, Not significant.
In the general population, use of medical services is for any type of headache, as only one subject had cluster headache.
Physicians, physiotherapists and others consulted
The use of non-medical treatments for headache is shown in Table 5. In total, non-medical treatment was received by 58% (49/85) of the cluster patients, which was significantly more frequent than among the general population.
Life-time use of non-medical treatment for headache, in a clinical and a general population
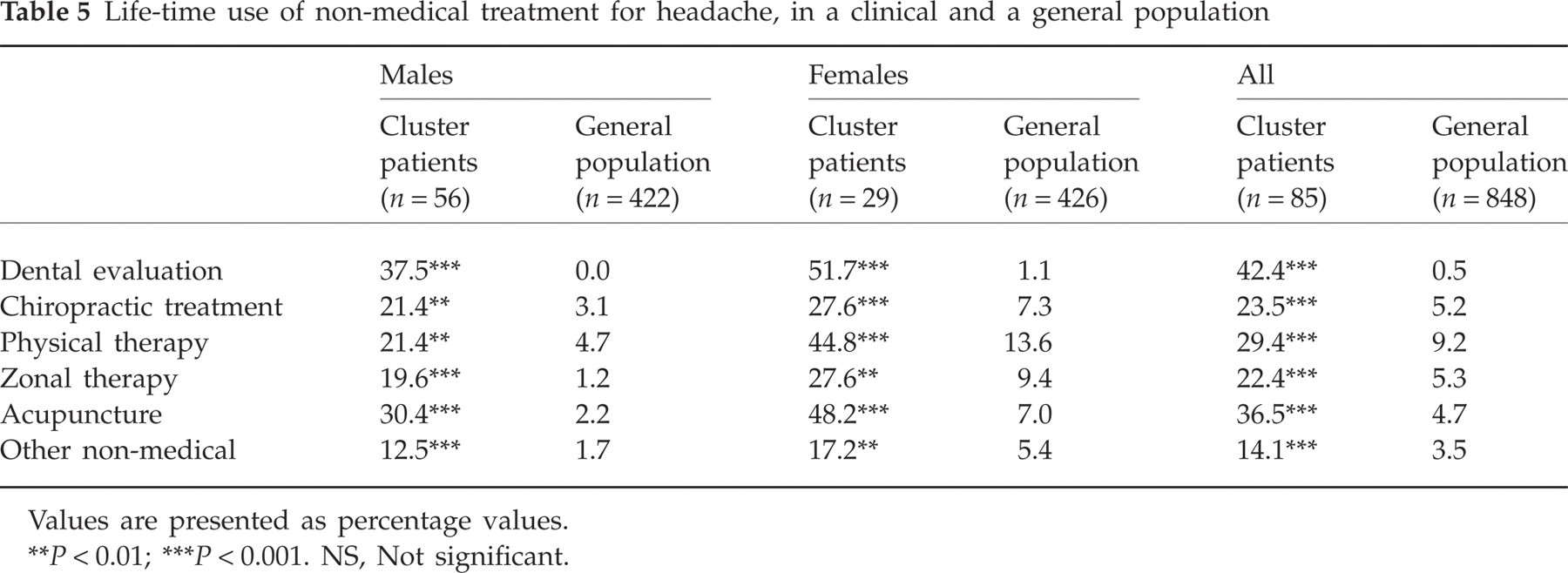
Values are presented as percentage values.
P < 0.01;
P < 0.001. NS, Not significant.
Discussion
In this study it has been shown that cluster headache, although periodic in most cases, has considerable impact on social functioning and quality of life. As expected, the vast majority of patients reported substantial restrictions to their daily living during cluster periods and some felt this inhibition even outside of clusters. Many patients changed their lifestyle because of the disease, mostly by altering sleeping habits and avoidance of alcohol during clusters. Our findings are consistent with those of Ertsey et al. (3), Solomon et al. (4) and D'Amico et al. (5), who demonstrated significant reduction in the overall quality of life measures among patients with cluster headache compared with migraine patients and healthy controls.
Many patients reported considerable impact on their working ability and efficiency during clusters, leading to changes in working place and pattern and cessation of specific job tasks. In addition, many patients felt that the cluster headache had limited their career. Others managed their jobs without many restrictions and the clinical population seems to cover a broad spectrum, from patients with very little work absence to patients with a very high frequency of sickness absence, loss of jobs and early retirement because of their cluster headache.
Although significantly higher than total absenteeism in the general population, the absence rate among cluster headache patients was actually lower than would be expected in patients from a selected clinical population in a tertiary centre. This may be a reflection of the periodicity, diurnal variation and short duration of the cluster headaches, which for some patients make it possible to go to work even on a day of attacks.
A considerably larger socioeconomic impact was expected among patients with chronic cluster headache, but we were unable to demonstrate this in the present study due to the limited number of chronically affected patients.
Almost all patients had been in contact with their GP because of the disease before referral to the Danish Headache Centre and as many as one-third had been admitted to hospital. A high number of patients had received specific dental evaluation and more than half had tried non-medical treatment such as physical therapy, chiropractic treatment, acupuncture or others, compared with a minority of the general population.
Although a specific socioeconomic analysis of total healthcare use before and after diagnosis of cluster headache is lacking, it is noteworthy that the need for acute medical services and the number of hospital admissions are relatively low among patients after diagnosis and treatment in the Headache Centre. This may reflect a lack of knowledge of cluster headache in the general Danish healthcare system, leading to a considerable overuse of medical and non-medical services, a very long diagnostic delay and lack of effective medical treatment. Thus, the present study illustrates the urgent and continuous need for education and information for the entire medical community.
Methodological considerations
There are several possible limitations to this study. The patient sample is drawn from a setting in a tertiary headache clinic, and our results may therefore not be representative of cluster headache patients in the general population, since speciality clinics usually see the most disabled and atypical patients. Nevertheless, most previous studies of cluster headache have been of patients from headache clinics. Furthermore, the present patient material shows a similar distribution between the episodic and chronic subforms and duration of disease as in prior epidemiological series (10–13) and our patients may therefore be comparable to most other clinic populations.
Another limitation to the study is the lack of a proper control group interviewed by the same investigator. We used the same questionnaire as was applied in the population study by Lyngberg et al. (6–8). Due to specific diagnostic information of cluster headache, we found it necessary to expand the questionnaire with additional questions about autonomic features, annual and diurnal periodicity and specific impact to ensure the diagnosis. Most of the questions about absence from work and use of healthcare services are nevertheless identical and therefore the data are comparable to those from the general population. The applied modified questionnaire is not specifically validated in a cluster headache population, whereas the general questionnaire has been found to be valid and reliable in the population study (6–8).
A specific questionnaire about quality of life was not included in the present study, first, because high-quality studies have previously documented the overall impact on quality of life in detail (3–5) and second, because we aimed to analyse the various underlying elements behind this general impact in order to target specific information and treatment campaigns in the future.
Recall bias is always a major problem in such clinical studies, but due to the high intensity of cluster headache it is expected that most patients may recall their attacks precisely and describe them in detail. Specific data about days off work and use of medical services are usually more unreliable but probably not different from other patient surveys or from the general population. The advantage of this study is the high diagnostic validity based on systematic registration, mandatory use of IHCD criteria and prospectively recorded headache diaries in the Danish Headache Centre, and that all interviews were preformed by the same medical doctor.
Furthermore, due to the Danish healthcare system, where medical services are totally free of cost for patients, we expect no effect of economic restrictions in the recorded data and therefore the results may be representative of the general use of healthcare services by cluster patients. On the other hand, most dental, chiropractic and other non-medical services are not covered by the public healthcare service and these data may therefore be skewed with respect to income level.
In conclusion, in addition to the severe pain attacks, cluster headache represents a major personal and socioeconomic impact on the individual and on society due to direct costs of healthcare services and indirect costs of lost work days and decreased work efficacy. Therefore, increased medical focus on early diagnosis, information to general society and effective treatment is of utmost importance.
Acknowledgements
We thank our laboratory technician Mrs Hanne Andresen for helpful technical assistance during the data collection. The study was supported by a grant from The Danish Cluster Headache Foundation.