
Abstract
A recent population-based prospective study reported that in women, migraine with aura (MA), but not migraine without aura (MoA), was associated with increased risk of coronary heart disease events (CHD). We sought to confirm this association in an Australian population-based cohort of older men and women (n = 2331, aged 49-97 years). We defined MA and MoA from face-to-face interview using International Headache Society criteria. Over a mean 6-year follow-up, 30 women (2.8%) and 30 men (4.4%) without any prior CHD history died from CHD-related causes. In women, a history of MA was associated with a non-significant twofold higher risk of CHD death (age-adjusted relative risk 2.2, 95% confidence interval 0.8, 5.8, P = 0.11), which remained similar after adjustment for cardiovascular risk factors. There were no CHD deaths in men with a history of migraine. Our findings support reports that in women, MA, but not MoA, may be associated with increased risk of CHD.
Introduction
There is substantial evidence that migraine may increase the relative risk of stroke (1), but the relationship between migraine and coronary heart disease (CHD) is less clear. A number of previous studies have suggested an association between migraine and chest pain, but not CHD (2–4). The Women's Health Study (WHS), a large prospective study, recently reported that migraine with aura (MA), but not migraine without aura (MoA), was associated with an increased relative risk of CHD events (myocardial infarction, coronary revascularization and angina) in women [hazard ratio (HR) of myocardial infarction after adjusting for cardiovascular risk factors 2.08, 95% confidence interval (CI) 1.30, 3.31; P = 0.002] (5). However, the relationship of migraine to CHD-specific mortality is unclear, with the WHS reporting an association between MA and the combined end-point of ischaemic cardiovascular disease (CHD and ischaemic stroke)-related death (HR 2.33, 95% CI 1.21, 4.51, P = 0.01) (5), but another, earlier study reporting a counterintuitive reduction in mortality among women reporting a history of headache or migraine (HR 0.72, 95% CI 0.52, 1.00) (6). In the study reporting an apparent protective effect, women with one or more features of migraine had a suggestion of reduced relative risk of death, although this was not significant (6). We sought to clarify the association of migraine with CHD mortality in an older Australian cohort.
Methods
The Blue Mountains Eye Study is a prospective, population-based cohort study of eye-related diseases and cardiovascular health outcomes in older persons (≥ 49 years) living in two postcode areas west of Sydney, Australia. In 1997–1999, 2331 persons were interviewed face-to-face by trained medical practitioners and asked a series of questions based on International Headache Society (IHS) guidelines for diagnosing migraine, from which we defined lifetime history of MA and MoA (7, 8). These categories were defined before knowledge of CHD outcome, which was ascertained 6 years later.
We defined CHD deaths from causes of death listed in the Australian National Death Index (NDI), which has been estimated to have high sensitivity (92.5%) and specificity (89.6%) for cardiovascular death (9). Further details on the validity of our migraine and CHD death ascertainment are reported elsewhere (8, 10). The Western Sydney Area Health Service Human Research Ethics Committee approved the study.
To obtain a similar population to that studied in the Women's Health Study, we excluded persons with a previous history of CHD (angina, acute myocardial infarction, coronary revascularization, n = 391) and without complete data on migraine (n = 208), leaving 1732 participants (1053 women, 679 men) for inclusion. We used Cox regression to assess the HR of CHD death, censored on 31 December 2003. We tested the proportional hazards assumption by including a time-dependent variable of migraine and the logarithm of survival time, and found no statistically significant violation.
Results
The mean age of persons without a lifetime history of migraine was 69.1 ± 8.7 years (
A history of any migraine was given by 233 women and 69 men. In women, 119 (11.3%) gave a history of MA, while 114 (10.8%) gave a history of MoA. Of men, 44 (6.5%) and 25 (3.7%) gave histories of MA and MoA, respectively. Over a mean follow-up of 6 years, 30 women (2.8%) and 30 men (4.4%) died from CHD-related causes. In women, a history of MA was associated with a non-significant twofold higher risk of CHD death (aged-adjusted HR 2.2, 95% CI 0.8, 5.8, P = 0.11) compared with women without a history of any migraine (Table 1). Further adjustment for coronary risk factors did not change this result (Table 1), although the association attenuated with additional adjustment for current and past use of hormone replacement therapy (multivariable adjusted HR 1.7, 95% CI 0.5, 5.9, P = 0.39). The rate of CHD death in women with a history of MoA was similar to that of women with no history of any migraine. Any migraine history in women was not associated with risk of CHD death (age-adjusted HR 1.3, 95% CI 0.5, 2.9, P = 0.89). In the whole population of women, including those with and without self-reported CHD (n = 1228), neither MA nor MoA was associated with CHD death (HR 1.1, 95% CI 0.4, 2.7 and HR 0.6, 95% CI 0.2, 1.8, respectively). Among women with self-reported CHD (n = 175), MoA was not associated with risk of CHD death, and there were no CHD deaths in women with a history of MA. There were no CHD deaths in men with a history of MA or MoA.
Migraine history and risk of coronary heart disease (CHD) death
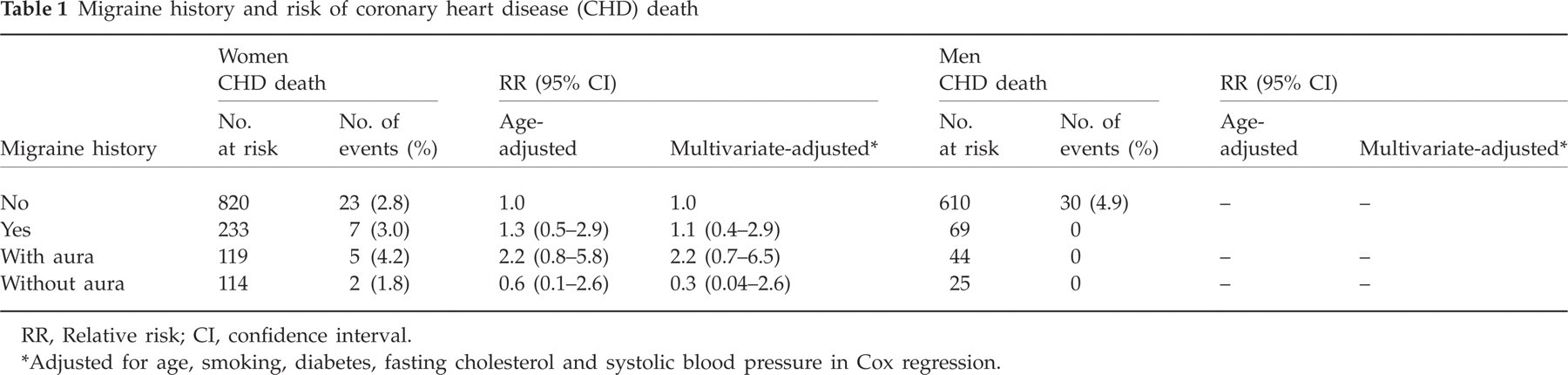
RR, Relative risk; CI, confidence interval.
Adjusted for age, smoking, diabetes, fasting cholesterol and systolic blood pressure in Cox regression.
Discussion
We report that in an older Australian population, a lifetime history in women of MA, but not MoA, was possibly associated with a non-significant, twofold higher risk of CHD death (P = 0.11). In women, a history of any migraine (combining either of these two migraine types) was not associated with risk of CHD death. There are caveats to our findings. First, our results are based on small numbers and do not reach statistical significance. This may be due to our smaller sample size (1053 vs. 27 840 women) and shorter follow-up (6 vs. 10 years
Our findings hence support a recent report that MA may increase the relative risk of cardiovascular events, including ischaemic cardiovascular death, in women, whereas MoA does not appear to (5). Our results differ from an earlier report suggesting that migraine in women may be associated with reduced relative risk of death (6). Possible reasons for the difference may be our use of IHS criteria for migraine definition, which were not available at the time of the earlier study, and the lifetime history of migraine we obtained, compared with a history of migraine symptoms/headache in the last year for the earlier study. If confirmed in other populations, these findings imply that there may be biological links between migraine and systemic cardiovascular disease. The nature of any such links are unknown, but may involve pro-coagulable states (14) or a generalized vascular disorder (15–17). The cardiovascular risk of men with migraine remains unclear and warrants further study.
Conflict of interest
None declared.
Acknowledgement
Supported by the Australian National Health & Medical Research Council, Canberra Australia (Grants no. 153948 and 302068).