
Abstract

A 32-year-old lady was admitted with sudden-onset left-sided headache followed rapidly by left-sided in-coordination and weakness. Initial examination revealed right hemi-sensory loss to pain and temperature sparing the face, left hemi-facial numbness and left-sided Horner's syndrome with left facial and palatal weakness. There was marked in-coordination of the lower limbs, the patient having a wide-based stance and gait. She had brisk deep tendon reflexes and extensor plantar reflexes bilaterally.
Magnetic resonance imaging of the brain (Fig. 1) revealed left medullary infarct and a magnetic resonance angiogram demonstrated left vertebral artery dissection with involvement of the posterior cerebellar artery. Because she had had a mildly raised temperature on admission, a cerebrospinal fluid examination was performed, which showed no cells, normal protein and glucose. The patient was anticoagulated with warfarin.
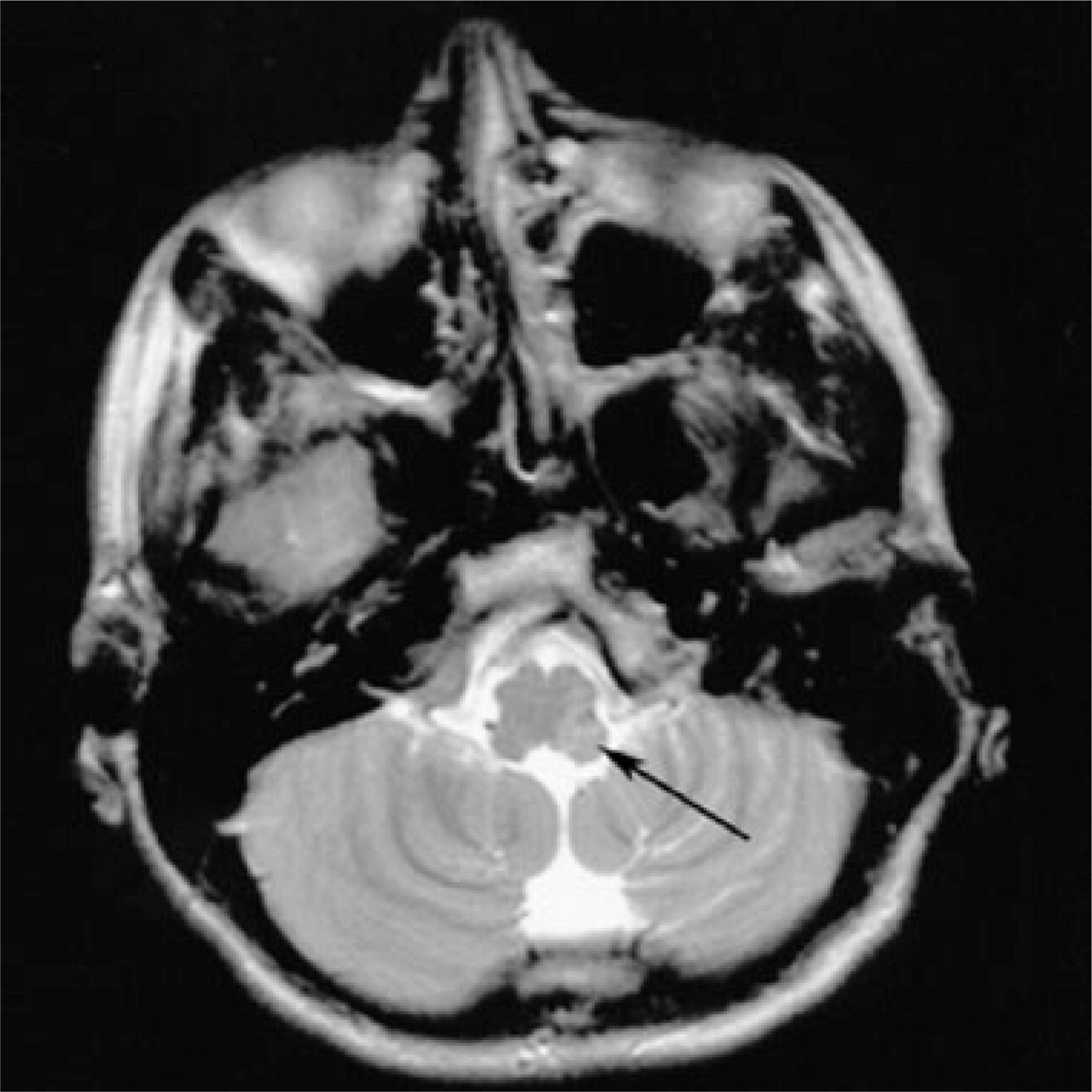
T2-weighted magnetic resonance imaging scan showing the medullary infarct (arrow) secondary to left vertebral artery dissection.
The patient continued to experience burning dysaesthesias involving the right side of the body, which was partially relieved by gabapentin (900 mg/day). Three to four weeks following the acute event she developed intermittent short-lasting left-sided headache lasting 5–300 s accompanied by left-sided ptosis, pupillary constriction as well as conjunctival injection. She was left with mild residual ptosis and miosis which got significantly worse during the attacks. However, there was no clear history of any excessive lacrimation. The headaches were mainly during the day, mainly involving the left orbito-frontal and parietal regions, happening at a frequency of three to five times daily. She denied having any triggers for these attacks. The truncal dysaesthesias improved significantly and were unrelated to the headaches. There was no past history or family history of headaches. The headaches partially responded to gabapentin (prescribed initially for right-sided dysaesthesia), later becoming resistant to it, at doses of up to 2700 mg/day. Other medications tried include pregabalin (up to 600 mg/day) and indomathacin (up to 150 mg/day), both of which had had a short-term effect. The headaches are currently well controlled (but with very infrequent relapses) using lamotrigine 100 mg/day in two divided doses. Attempts to reduce or withdraw the medication were resisted by the patient, fearing relapse of further attacks.
Discussion
Short-lasting unilateral neuralgiform headache with conjunctival injection and tearing (SUNCT) is a rare form of trigeminal autonomic cephalalgia (TAC) mostly described as a primary headache syndrome. The acute headaches are usually accompanied by ipsilateral conjunctival injection, lacrimation, rhinorrhoea, nasal congestion, ptosis, miosis and facial redness or sweating (1). Short-lasting unilateral neuralgiform headache with cranial autonomic symptoms (SUNA) has been defined by the International Headache Society (ICHD-2) as similar to SUNCT with less prominent or absent conjunctival injection and lacrimation (2). Ipsilateral cranial parasympathetic activation and sympathetic hypofunction have been implicated in the pathophysiology of autonomic symptoms in these patients (3). Our patient satisfied all the criteria for SUNCT except for lacrimation, making it possible to label her condition SUNA rather than SUNCT. It is possible that case reports of SUNA (without conjunctival congestion and/or tearing) are not published as widely as SUNCT. SUNA could represent a forme fruste of SUNCT and may have more widespread autonomic symptoms as the syndrome evolves. Further long-term observational studies might provide insight into the natural history of this rare headache syndrome.
SUNCT syndrome has been described secondary to other causes. Posterior fossa lesions, including ipsilateral cerebellopontine angle arteriovenous malformations (4, 5), brainstem cavernous haemangioma (6) and base of skull bony abnormalities (7, 8) have been described anecdotally to be associated with SUNCT. Posterior fossa lesion in a patient with human immunodeficiency virus (3) and pituitary adenomas (9) have been described as other associations.
Lateral medullary infarction is associated with headaches in up to 76% of patients (10). As far as we are aware, this is the third patient described to have this form of trigeminal autonomic cephalalgia following a medullary infarction. One of the previously described patients revealed no radiological evidence of brainstem infarction (11) but the other patient demonstrated left medullary infarction and vertebral artery dissection (12), similar to our case. SUNCT has been described following previous cerebellar lacunar infarct (13). Hemicranial headaches have been described in four out of 10 consecutive patients with vertebral artery dissection, with no autonomic features described in any of these patients (14). Cluster-like headaches lasting approximately 2 h have been described in two patients with vertebral artery dissection and lateral medullary infarction (15).
The trigeminovascular reflex plays an important role in the pathophysiology of trigeminal autonomic cephalalgias. Afferent impulses through the trigeminal nerve relay in the trigeminocervical complex, consisting of the trigeminal nucleus caudalis in the caudal medulla and dorsal horns of C1/C2. Efferents from this complex pass through the superior salivatory nucleus and greater petrosal nerve to the sphenopalatine ganglion mediating the parasympathetic features of TACs. The resulting vasodilation of the intra- and extracerebral arteries provides a positive feedback to the trigeminal afferents (16). A lesion in the medulla affecting fibres of the trigeminovascular complex or the sympathetic pathway may be responsible for the production of these headache syndromes.
Recently, criteria have been proposed to establish a causal relationship between the associated lesion and the headache syndrome (Table 1) (17). Our patient satisfied three of the four criteria, the fourth (surgical or aetiological treatment) not being applicable to this case.
Criteria for determining causal relationship between associated pathology and headache (Trucco et al.) (17).

We have described a patient with clear left-sided medullary infarct following vertebral artery dissection whose headache description would be consistent with the classification of SUNCT/SUNA. Recognition of such rare headaches secondary to relatively common vascular events is important in instituting the appropriate treatment. This case would further support the hypothesis that brainstem trigeminal autonomic pathways are important in the pathogenesis of this rare headache syndrome.