
Abstract
Case Report
A 37-year-old gravida 2, para 2 woman developed a severe bi-frontal non-throbbing postural headache a few minutes after receiving epidural anaesthesia for labour. Her pregnancy was uncomplicated. There was no prior history of migraine, clotting disorders, or exposure to vasoactive drugs. The headaches persisted and she was treated with an epidural blood-patch on day 1 post-delivery for a presumptive diagnosis of low-pressure headache. The character of her headache changed from dull aching to constant throbbing. It now involved her entire head, was accompanied by nausea and vomiting, and did not have obvious precipitating or relieving factors. A non-contrast CT scan on day 4, performed at an outside hospital, was reportedly normal. Over the next 2 days she developed horizontal diplopia and right leg weakness. On day 6, a repeat non-contrast head CT scan showed a new small left posterior frontal hyperdensity, and she was transferred to our hospital.
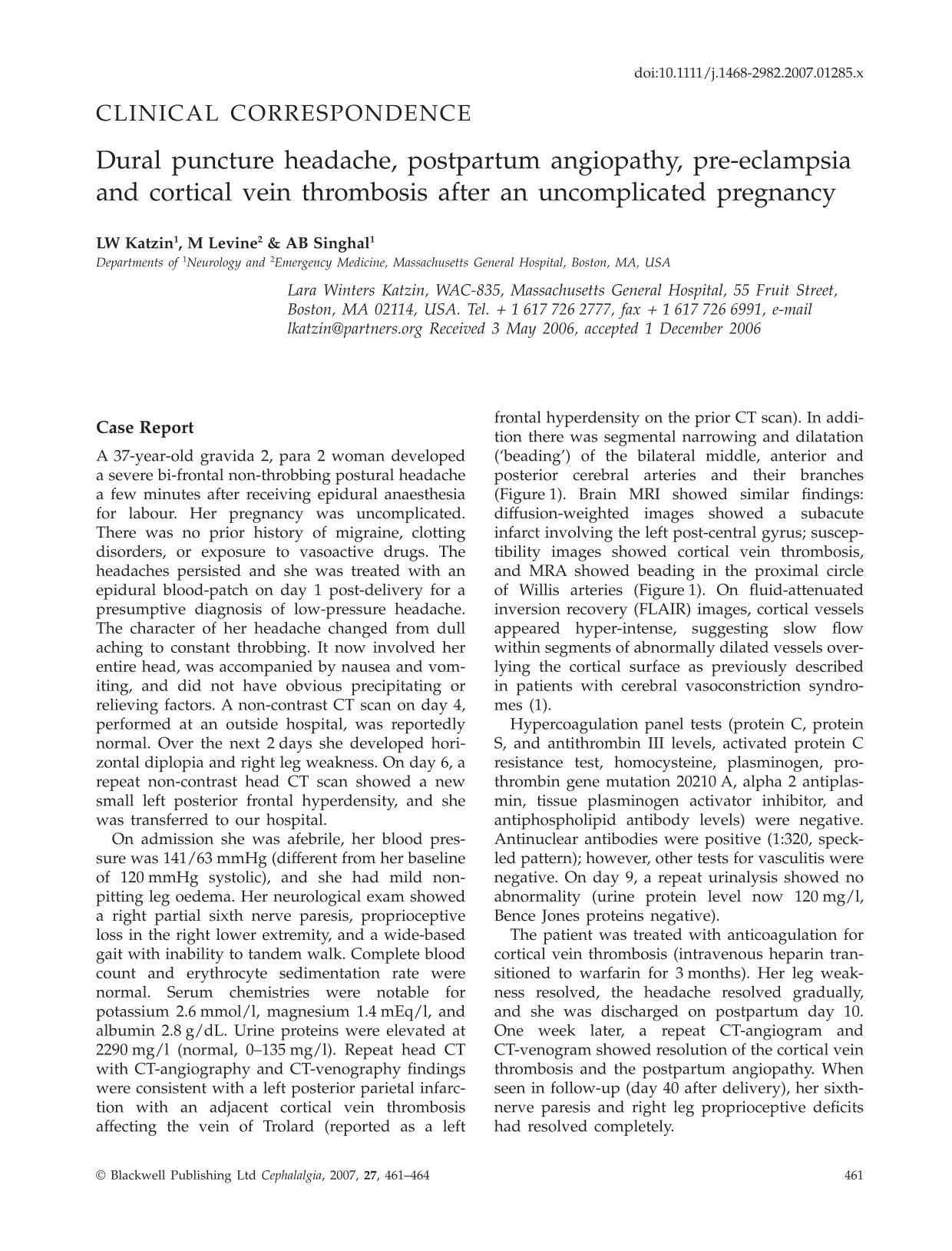
On admission she was afebrile, her blood pressure was 141/63 mmHg (different from her baseline of 120 mmHg systolic), and she had mild non-pitting leg oedema. Her neurological exam showed a right partial sixth nerve paresis, proprioceptive loss in the right lower extremity, and a wide-based gait with inability to tandem walk. Complete blood count and erythrocyte sedimentation rate were normal. Serum chemistries were notable for potassium 2.6 mmol/l, magnesium 1.4 mEq/l, and albumin 2.8 g/dL. Urine proteins were elevated at 2290 mg/l (normal, 0–135 mg/l). Repeat head CT with CT-angiography and CT-venography findings were consistent with a left posterior parietal infarction with an adjacent cortical vein thrombosis affecting the vein of Trolard (reported as a left frontal hyperdensity on the prior CT scan). In addition there was segmental narrowing and dilatation (‘beading’) of the bilateral middle, anterior and posterior cerebral arteries and their branches (Figure 1). Brain MRI showed similar findings: diffusion-weighted images showed a subacute infarct involving the left post-central gyrus; susceptibility images showed cortical vein thrombosis, and MRA showed beading in the proximal circle of Willis arteries (Figure 1). On fluid-attenuated inversion recovery (FLAIR) images, cortical vessels appeared hyper-intense, suggesting slow flow within segments of abnormally dilated vessels overlying the cortical surface as previously described in patients with cerebral vasoconstriction syndromes (1).

(a) Axial diffusion weighted MRI shows an infarct in the left post-central gyrus. (b) Susceptibility MRI shows a thrombus in the vein of Trolard. (c) FLAIR MRI shows hyperintense cortical vessels indicating slow blood flow (arrows) within abnormally dilated cortical surface vessels. (d) Three-dimensional time of flight MRA shows diffuse segmental vasoconstriction affecting the circle of Willis arteries and their branches. (e) CT angiography (CTA) shows vasconstriction but upon repeat imaging 1 month later. (f) the vasconstriction has resolved.
Hypercoagulation panel tests (protein C, protein S, and antithrombin III levels, activated protein C resistance test, homocysteine, plasminogen, prothrombin gene mutation 20210 A, alpha 2 antiplasmin, tissue plasminogen activator inhibitor, and antiphospholipid antibody levels) were negative. Antinuclear antibodies were positive (1:320, speckled pattern); however, other tests for vasculitis were negative. On day 9, a repeat urinalysis showed no abnormality (urine protein level now 120 mg/l, Bence Jones proteins negative).
The patient was treated with anticoagulation for cortical vein thrombosis (intravenous heparin transitioned to warfarin for 3 months). Her leg weakness resolved, the headache resolved gradually, and she was discharged on postpartum day 10. One week later, a repeat CT-angiogram and CT-venogram showed resolution of the cortical vein thrombosis and the postpartum angiopathy. When seen in follow-up (day 40 after delivery), her sixth-nerve paresis and right leg proprioceptive deficits had resolved completely.
Discussion
Headache in the postpartum period has a wide differential diagnosis including postdural puncture headache, postpartum pre-eclampsia, postpartum angiopathy, pituitary apoplexy, Sheehan's syndrome, lymphocytic hypophysitis, subarachnoid haemorrhage, subdural haemorrhage, brain tumour, and arterial and venous infarctions (2). Shortly after delivery, our patient developed postdural puncture headache followed by postpartum angiopathy, postpartum pre-eclampsia, and cortical vein thrombosis, which is unusual. She probably developed a postdural puncture headache related to inadvertent dural puncture from epidural catheter placement, then more severe headaches from postpartum angiopathy, cortical vein thrombosis, or postpartum pre-eclampsia.
Postpartum cerebral angiopathy is a prototype cerebral vasoconstriction syndrome characterized by the abrupt onset of thunderclap headaches, generalized seizures and focal neurological deficits, typically in the first 2 weeks after delivery, associated with segmental arterial narrowing and dilatation (‘beading’) of medium and large sized cerebral arteries that is reversible on serial angiography (3). The syndrome can be complicated by ischaemic strokes, usually located in ‘watershed’ arterial territories. Most patients recover spontaneously within days to weeks. Postpartum pre-eclampsia is the triad of peripheral oedema, hypertension and proteinuria, usually developing within a few days after delivery (4). Postpartum cerebral angiopathy has been associated with pre-eclampsia, and brain MRI in such patients can show cerebral arterial vasoconstriction as well as features of the reversible posterior leukoencephalopathy syndrome (5). Our patient had transient hypertension relative to baseline, peripheral oedema and proteinuria, as well as reversible angiographic ‘beading’ of intracerebral arteries, which is consistent with a diagnosis of postpartum angiopathy with pre-eclampsia. Except for the positive ANA, she did not have any features of vasculitis or rheumatologic disorders such as systemic lupus erythematosis (SLE). Further tests for cerebral vasculitis such as cerebrospinal fluid examination were not performed, because the onset and resolution of clinical-angiographic abnormalities without immunosuppressive therapy is most consistent with postpartum angiopathy, and virtually excludes the possibility of cerebral vasculitis (3).
Risk factors for cerebral venous sinus thrombosis include dehydration, genetic and acquired prothrombotic states, infections such as mastoiditis or sinusitis, inflammatory diseases including SLE, haematologic conditions such as leukaemia and thrombocytopenia, oral contraceptive use, head trauma, and neurosurgical procedures (6). In addition, cortical vein thrombosis and cerebral venous sinus thrombosis have been reported in the postpartum state, often associated with epidural anaesthesia during labour (7, 8). The pathophysiology of venous sinus thrombosis after delivery is unclear. Some authors have proposed that thrombosis results from a relative hypercoagulable state, or damage to the venous sinuses from fluctuations in intracranial pressure during delivery (8). Most patients with venous thrombosis after labour and delivery are initially diagnosed with a postdural puncture headache and undergo a dural blood-patch procedure; venous sinus thrombosis is eventually diagnosed when the headache persists or changes in character over time, recurs despite treatment, or if the patient develops neurological symptoms from the venous thrombosis. It is unclear whether there is a causative relationship between dural puncture and venous sinus thrombosis. It is believed that cerebrospinal fluid drainage induces a downward shift of the brain with traction on the cortical veins and sinuses, which results in thrombosis from deformation of the walls of the cerebral veins (6). In our patient, mild dehydration, the hypercoaguable postpartum state, and inadvertent dural puncture, are three potential contributing factors for the vein of Trolard thrombosis. Interestingly, however, dural puncture has been independently associated with cerebral venous sinus thrombosis and with reversible diffuse cerebral arterial vasospasm (i.e. cerebral vasoconstriction syndrome) (9). Furthermore, the cerebral veins may also be affected by disturbances in autoregulation. The coexistence of cortical vein thrombosis and postpartum angiopathy in our patient raises the question of an interrelationship between these conditions.
Our patient had several different aetiologies for her postpartum headaches, which were diagnosed upon investigating the changing character of her pain. While postdural puncture headaches are the most common cause of head pain post-delivery, it is important to consider other causes of headaches in the postpartum period, especially if the headaches are not position-dependent, persist after blood patch, or are associated with neurological deficits. In such cases, appropriate neuroimaging tests should be obtained to exclude conditions such as cerebral venous sinus thrombosis and postpartum angiopathy.