
Abstract

Spontaneous intracranial hypotension (SIH) is caused by spontaneous cerebral spinal fluid (CSF) leakage at the level of the spine and is of unknown aetiology. It is typically characterized by orthostatic headache, low CSF pressure (<60 mmH2O), and a magnetic resonance image (MRI) finding of diffuse pachymeningeal enhancement (1). In most cases, SIH patients have typical orthostatic headaches and associated symptoms such as neck stiffness, photophobia or nausea. They recover well after hydration or epidural blood patches (EBP). Some SIH patients develop neurological deficits such as cranial nerves palsy (2, 3), frontotemporal dementia (4), Parkinsonism (5), consciousness disturbance (6–11), or cerebral sinus venous thrombosis (12). These complicated cases usually recover well after aggressive treatment, such as intrathecal saline injection, EBP or surgical intervention. Very rarely do patients with SIH have unrecoverable sequelae such as Duret haemorrhage (11) or even mortality (13). Here we report an SIH patient with bilateral subdural haematomas (SDH) who developed transtentorial herniation and infarction of bilateral posterior cerebral artery territories, midbrain and pons, during hospitalization.
Case report
A 43-year-old rubber worker was well until he developed posterior neck pain after waking up on the morning of 12 July 2005. The posterior neck pain occurred when he sat or stood up for 1–2 min and was relieved after lying down. If he maintained an upright position, the pain became severe and radiated to bilateral temporal areas and was accompanied by dizziness, blurred vision and tinnitus.
He was admitted to a hospital 3 days after the onset of symptoms. Physical and neurological examinations showed no remarkable findings. Biochemical studies were normal. Lumbar puncture showed the opening pressure was 98 mmH2O. The CSF was acellular, with a normal glucose level (60 mg/dL) but a high protein level (105 mg/dL). Brain MRI with gadolinium contrast revealed diffuse pachymeningeal enhancement. SIH was diagnosed. The myelography and post-myelographic computed tomography (CT) failed to demonstrate a CSF leakage site. After hydration and bed rest, his symptoms improved markedly. He was discharged after 11 days of treatment. At discharge, he still had mild neck soreness and stiffness.
Two months later, he developed an acute, severe but non-postural headache over the whole head while he was working in the early morning. The pain gradually worsened and was accompanied by nausea and dizziness. He visited the Emergency Department of our hospital 1 week after the onset of symptoms. Physical and neurological examinations were normal. Brain MRI with gadolinium contrast showed diffuse pachymeningeal enhancement, SDH (high intensity signal in both T1 and T2 weight images) about 10 mm thick in bilateral frontotemporoparietal areas, and brain descent with obliteration of basal cistern but absence of midline shift. Eye fundi examination did not reveal any evidence of papilledema.
Intravenous hydration and aminophylline were given. MR myelography demonstrated extradural CSF collection at C1-3 and T10. Sixteen hours after admission, his consciousness deteriorated (Glasgow Coma Scale: E1V2M5). The follow-up brain CT showed no change of SDH size as compared with the previous image. Despite an EBP with 20 cc autologous blood performed 5 hours after mentality change, the patient rapidly became comatose (E1V1M1) with bilateral, dilated, non-responsive pupils and absent oculocephalic reflex. Emergent occipital decompressive craniectomy and duraplasty were performed right away to release the infratentorial pressure. Nevertheless, the intracranial pressure was not high because the CSF did not overflow from cutting the dura during the operation. After the above procedures, bilateral burr holes were made for drainage of subdural fluid.
After the operation, he remained comatose, but he had spontaneous limb movement beginning from the first day after the operation. Another two EBPs were performed on the third and fourth days after operation. His neurological condition did not improve immediately after the EBPs.
Brain MRI with gadolinium contrast on the fifth day after the operation revealed alleviation of SDH but presence of acute infarctions of bilateral occipital and mesial temporal lobes, right thalamus, midbrain, and upper pons (Fig. 1). Additionally, haemorrhage was noted at the midbrain and upper pons (Fig. 2). Brain MR angiography revealed no occlusion or stenosis of all intracranial arteries. The acute infarctions and secondary haemorrhage in the brainstem (Duret haemorrhage) were most likely caused by transtentorial herniation.

The T2-weighted MR images revealed infarction of bilateral occipital regions of the brain and right thalamus (a), bilateral mesial temporal regions of the brain and the midbrain (b) and bilateral aspects of the pons (c) on the fifth day after the operation.
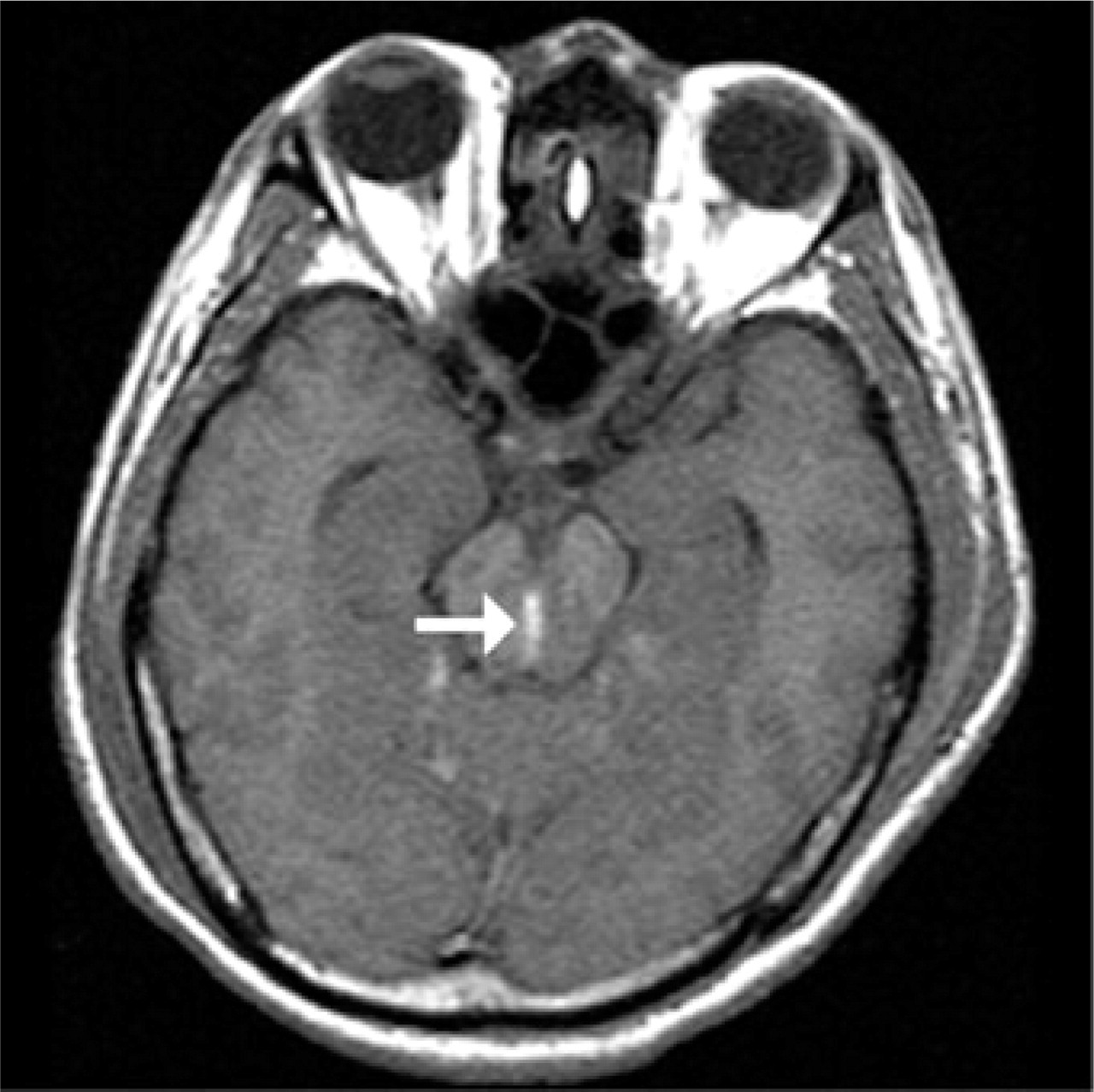
The non-contrast T1-weighted MR image showed haemorrhage (high signal component) in the midline of the midbrain (arrow) on the fifth day after the operation.
The patient could obey simple commands to raise his limbs occasionally on the 46th day after the operation. Six months after the operation, his visual acuity was impaired, and he could only count fingers. His cranial nerve function was preserved, except for oculomotor palsy. He could obey commands to move his four limbs although his muscle power was still weak (MRC scale 4/5) with spasticity.
Discussion
Most SIH patients have a benign disease course and good prognosis. Duret haemorrhage caused by transtentorial herniation, as in our patient's condition, has only been reported in one SIH patient (11), who recovered later with ataxia and dysarthria after bilateral burr holes and subdural fluid drainage. In addition to transtentorial herniation and Duret haemorrhage, our patient had infarctions of bilateral occipital and mesial temporal lobes, right thalamus, midbrain, and pons, which so far have not been reported. Only one fatality, for a Korean patient with SIH (13), was reported in the literature. The patient had orthostatic headache and diplopia, with complete recovery after conservative treatment. However, he developed recurrent headaches with vomiting 4 weeks later, followed by consciousness disturbance and cardiac arrest, which were considered to be caused by brain descent.
In SIH patients with consciousness disturbance (6–11), most received treatment after a relatively long period of time (days to weeks) since consciousness deteriorated but almost all of them recovered well. Our patient developed unrecoverable sequelae after only less than 12 h of consciousness disturbance. It implies that brain descent could develop suddenly and acutely and should not be overlooked.
There is no consensus regarding the management of SIH complicated with SDH. In one case series of 40 SIH patients (14), half of them had subdural collections. All of them recovered well after their CSF leaks were treated either by supportive care, EBP, or surgical repair. Three of them underwent surgical drainage of SDH at first. None of their SDH resolved until the underlying CSF leak was treated. In another study (15), an SIH patient showed deteriorating consciousness after craniotomy but recovered after EBP. It was hypothesized that the deterioration was the result of acute brainstem displacement provoked by opening the hypovolemic intrathecal space to atmospheric pressure. Therefore, craniotomy might do more harm than good for SIH patients. Only one case series (11) supported the role of surgical drainage of SDH. The four reported patients improved after neurosurgical drainage and all of them showed large SDH with obvious midline shift or mass effect. The surgical intervention of SDH in SIH patients might only be indicated in a few select cases.
Surgical treatment of SDH was not considered initially for our patient because he had no consciousness disturbance or focal neurological deficit, and the brain haematoma thickness was less than 15 mm without midline shift (16). When his consciousness deteriorated, we believed it was caused by diencephalic compression secondary to severe brain descent and herniation resulting from intracranial hypotension. Therefore, EBP was performed first but failed to reverse his neurological deterioration. We then considered that SDH might contribute to his condition in part and surgical decompression was performed. Unfortunately, the surgery neither improved his consciousness nor prevented permanent neurological damage.
According to our patient and some prior case reports, surgical drainage of SDH alone cannot resolve intracranial hypotension and may worsen it (16) if the underlying CSF leakage is not resolved (14, 17, 18). It is important to treat CSF leakage and restore CSF volume earlier in patients with SIH and SDH to prevent irreversible sequela.
Acknowledgements
This study was supported in part by a grant from Taipei Veterans General Hospital (V95C1-035).