
Abstract

Intracranial hypotension is a syndrome of low cerebrospinal fluid (CSF) pressure characterized by postural headache (1). It may occur following lumbar puncture, craniotomy, spinal surgery, or spontaneously – so-called spontaneous intracranial hypotension (SIH). The diagnosis of SIH can be challenging. Recent reports have emphasized intracranial magnetic resonance (MR) findings in SIH (1–4). However, SIH complicated by cerebral sinus venous thrombosis has been mentioned rarely in the literature (5, 6). We present a rare case of SIH complicated by isolated cortical vein thrombosis (ICVT) and cerebral venous infarction. Therapy with epidural blood patch and intravenous heparin was successful.
Case report
A 45-year-old woman with a history of increasingly severe headache, nausea and vomiting for 2 weeks suddenly developed a feeling of numbness in her right leg and had an epileptic seizure involving the right leg. During this episode, she was unable to answer any questions. Upon arrival at the emergency department, the patient was postictal; although somnolent, she was easily arousable and able to answer all questions appropriately. She had no recollection of the event and denied having an aura. The headache had postural variation, worsening on standing up and improving when lying down. The patient had been doing vigorous exercise during the previous month. There was no history of dural puncture, epidural anaesthesia or infiltration. Physical and neurological examinations, including eye funduscopsy, were normal. At lumbar puncture, the CSF opening pressure was 10 mmH2O; CSF composition was normal.
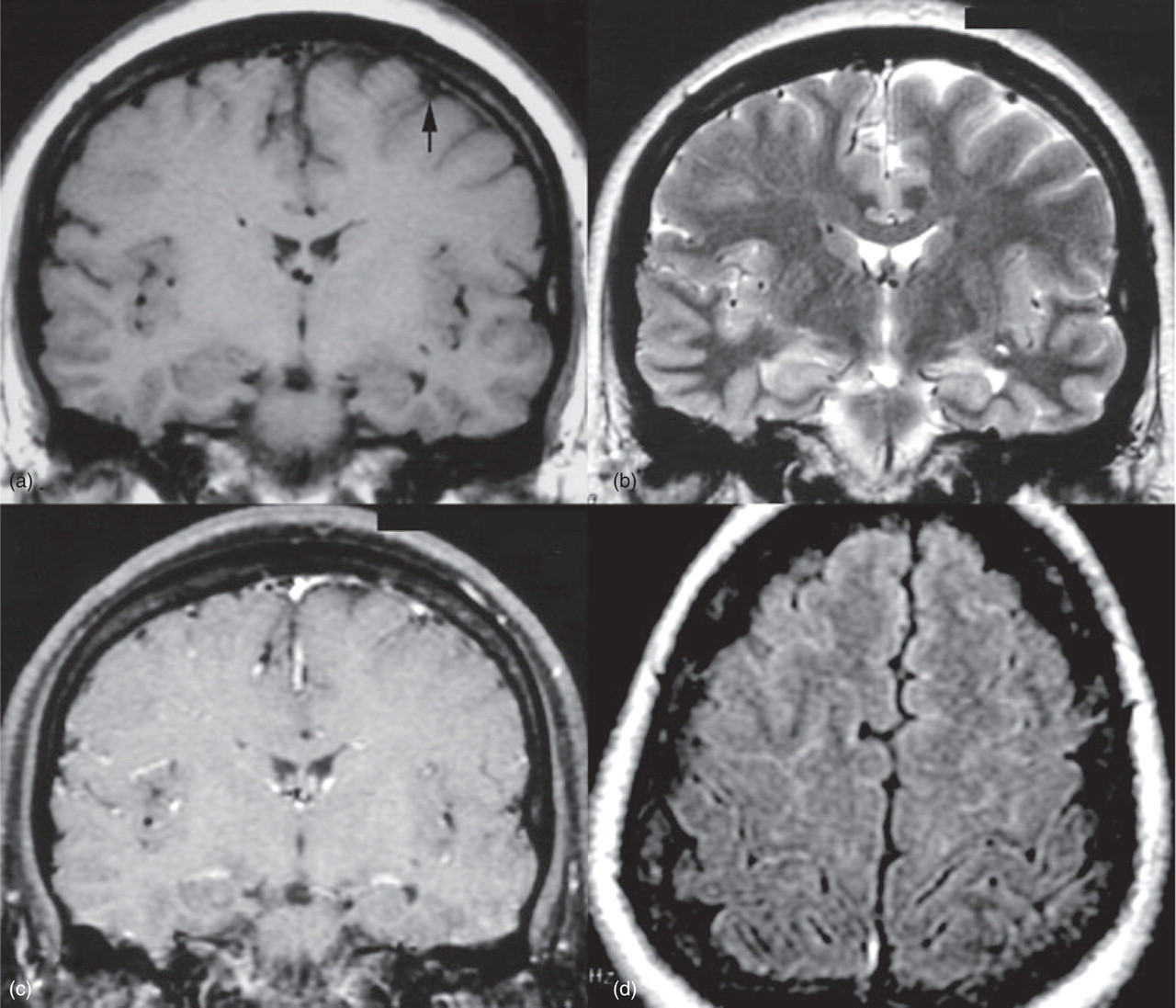
MR imaging (MRI) showed a hyperintense signal of the left cortical vein suggesting subacute thrombosis or slow flow on T1- and T2-weighted images. On T2-weighted and fluid attenuated inversion recovery (FLAIR) images, a hyperintense lesion was noted in the left frontal lobe and subdural fluid collections in both hemispheres. A gadolinium-enhanced T1-weighted image revealed diffuse pachymeningeal enhancement (Fig. 1). No sinus thrombosis or dural arteriovenous fistula was seen on MR venography (MRV) and conventional angiography. Proton MR spectra, obtained from the point-resolved spectroscopy (PRESS) sequence, revealed a decreased N-acetylaspartate/creatine (Cr) ratio, a mildly increased choline/Cr ratio and the presence of lactate in the left frontal lesion compared with contralateral right frontal lobe, indicating acute ischaemic venous infarction (Fig. 2). No underlying neoplastic and thrombotic disorders were revealed during further investigation. With this diagnosis of SIH associated with ICVT and venous infarct, therapy with epidural blood patch and intravenous heparin was given. Within 7 days of heparin treatment, the headache gradually disappeared. After discharge, the patient has remained asymptomatic while under oral anticoagulation treatment for 6 months. Repeated MRI at 3 months showed cortical vein recanalization. The subdural fluid and venous infarct completely resolved and meningeal enhancement disappeared (Fig. 3). Patient remained well 1 year later.

(a) Coronal T1-weighted magnetic resonance image (MRI) of the brain shows a hyperintense cortical vein (arrow), suggesting subacute thrombosis. (b) Coronal T2-weighted MRI shows subdural fluid collections in both hemispheres. (c) Coronal gadolinium-enhanced T1-weighted MRI reveals diffuse pachymeningeal enhancement. (d) Axial fluid attenuated inversion recovery MRI reveals mild hyperintensity of left frontal region. This abnormal signal intensity suggests venous infarction.
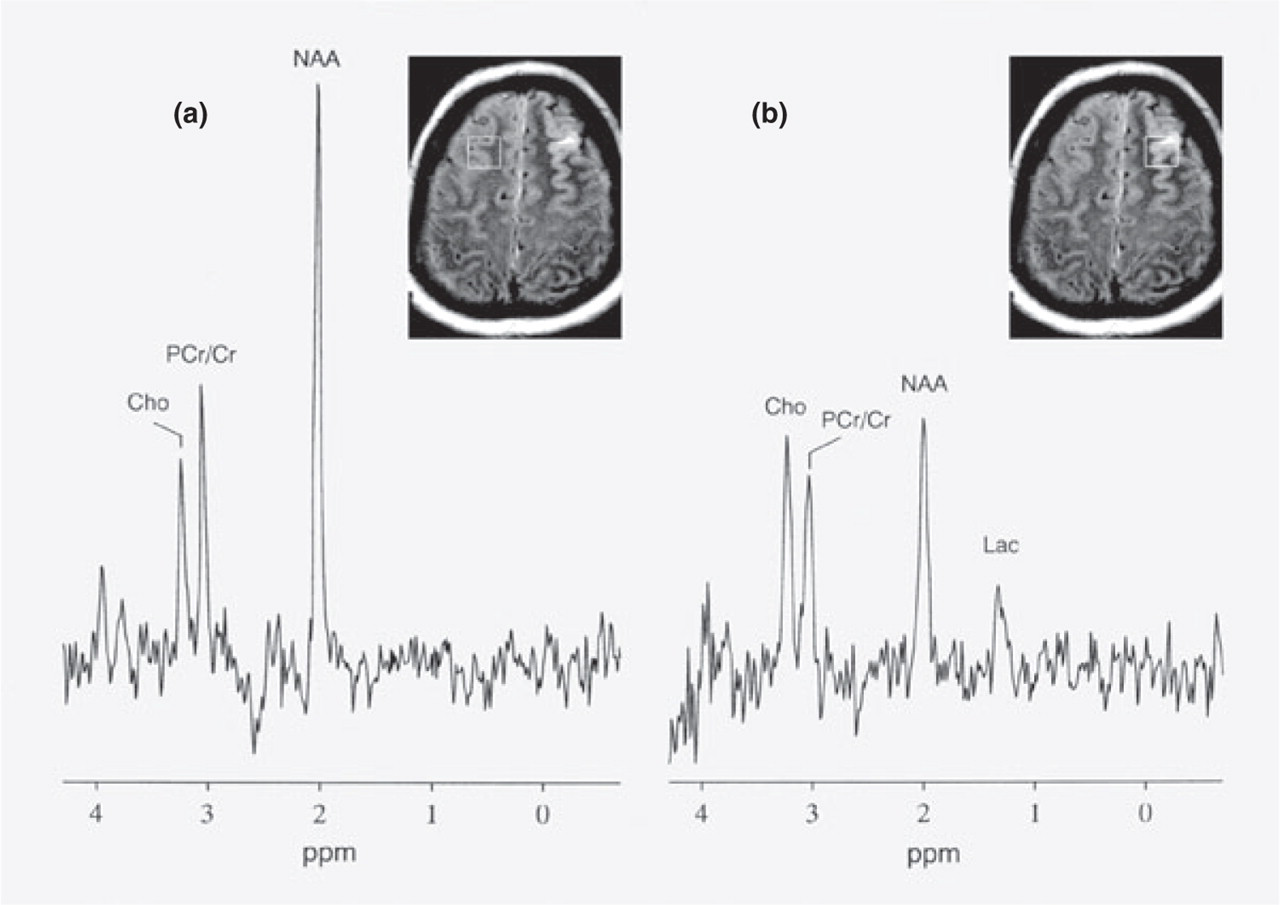
Magnetic resonance (MR) spectra of the left frontal lesion and contralateral side. Chemical shift (horizontal axis) in p.p.m. Each region of interest in the MR image shows the location where the spectrum was obtained. (a) Right frontal lobe normal spectrum (point-resolved spectroscopy; 1500/270, TR/TE). N-acetylaspartate (NAA; 2.02 p.p.m.), phosphocreatine/creatine (PCr/Cr; 3.0 p.p.m.) and choline (Cho; 3.21 p.p.m.) peaks are well identified. The ratios of NAA/Cr (2.32) and Cho/Cr (0.87) are calculated. (b) Proton spectrum of the left frontal lesion shows the presence of lactate (1.3 p.p.m.), decreased NAA/Cr ratio (1.29) and a mildly increased Cho/Cr ratio (1.13), indicating acute ischaemic venous infarction.
Repeated magnetic resonance imaging (MRI) at 3 months. (a) Coronal T1-weighted MRI of brain shows a signal void of the corresponding cortical vein (arrow), indicating cortical vein recanalization. (b) Coronal T2-weighted MRI shows complete resolution of subdural fluid. (c) Gadolinium-enhanced T1-weighted MRI reveals disappearance of meningeal enhancement. (d) Axial fluid attenuated inversion recovery MRI reveals complete resolution of venous infarct at the left frontal region.
Discussion
Intracranial MR findings of SIH include subdural fluid collections or haematomas, downward descent of the midbrain and cerebellar tonsils and a reduction in the size of the prepontine cistern (1–4). However, the most characteristic finding is diffuse pachymeningeal enhancement (1, 2). The MR findings of SIH reflect an increase in venous volume throughout the brain. The explanation for the increased venous volume is thought to be the Monro–Kellie rule (7), which states that intracranial volume is always constant and is represented by the summed volumes of the brain substance, CSF and blood. With an increase in venous blood, there is presumably accumulation of contrast material in the pachymeninges due to the lack of a blood–brain barrier.
SIH complicated by cerebral sinus venous thrombosis has rarely been mentioned in the literature (5, 6). Cerebral sinus venous thrombosis with SIH has been suggested by the change in the pattern of headache, from a postural to a permanent one (5). Our patient presented as an increasingly severe headache but without change of headache pattern. Based on the pathophysiology of SIH, it is theoretically possible that SIH causes a downward shift of brain with traction on the cortical veins and sinuses. Deformation of the venous walls, dilation and stasis in the venous system may predispose to venous thrombosis (5, 6). This association raises important practical issues regarding definite diagnosis and appropriate treatment.
ICVT is less commonly encountered than dural sinus thrombosis. Its detection depends primarily on visualizing the thrombosed vein and, secondarily, on visualizing any associated venous infarction or haemorrhage. The most sensitive examination technique is MRI in combination with MRV (8). The acute thrombosis may mimic a flow void when the clot tends to be isointesne on T1-weighted images and hypointense on T2-weighted images. Idbaih et al. have shown that T2∗ susceptibility-weighted imaging may be useful for acute clot detection of cerebral venous thrombosis in conjunction with conventional MRI and MRV (9). The subacute thrombosis becomes hyperintense on T1- and T2-weighted images. The venous infarct is suggested if swollen gyri are apparent, and the venous infarct was further confirmed by MR spectroscopy in our case. The venous infarction may be reversible if the underlying condition is treated early and successfully (8).
The occurrence of ICVT in patients with SIH also raises difficult practical questions as regards the treatment of these two conditions. The first-line treatment of SIH is epidural blood patch (1, 2). For treatment of ICVT, despite a long debate about the use of heparin, most neurologists now start with heparin as soon as the diagnosis is confirmed, even in the presence of haemorrhagic infarcts (8). In our patient, treatment with epidural blood patch and intravenous heparin was successful.
In summary, this first case report demonstrated ICVT associated with cerebral venous infarction in a patient with SIH. Therapy with epidural blood patch and intravenous heparin was successful. Knowledge of this association can be helpful in facilitating definite diagnosis and appropriate treatment.
Acknowledgements
This study was supported by grant NSC 94-2314-B-075B-008 (P-H.L.) from the National Science Council, Taiwan, ROC.