
Abstract

Idiopathic intracranial hypotension is a frequently overlooked headache entity, as it shares many clinical features with migraine without aura. Its diagnosis requires the documentation of headache that worsens after sitting or standing and low CSF pressure or the direct visualization of CSF leakage (1). Until recently, most available diagnostic imaging techniques entailed penetration of the lumbar subarachnoid space to measure the opening pressure or administer intrathecal agents. Despite the progressive refinement of contrast agents, side-effects of these techniques are still relatively common. The resultant iatrogenic dural defects further complicate diagnosis and effective management. Development of non-invasive imaging techniques is needed, but this is hampered by the complicated anatomy of the region and the dynamic process of CSF flow and absorption, which may not allow the demonstration of slow leaks that do not result in large fluid accumulations.
We here report a patient with idiopathic intracranial hypotension, in whom the dural leaks were identified with SSFSE MR myelography.
Case report
A 38-year-old right-handed woman started experiencing headaches 5 months prior to the initial evaluation. They were throbbing, of bilateral fronto-occipital location, occurred daily, and would improve with lying down and worsen with sitting or standing up. They would also worsen with straining, coughing or bending over. They were associated with mild photophobia and nausea, but no phonophobia. There was no neck stiffness or focal neurological symptoms.
She had three bouts of similar headaches. The first one occurred 15 years ago, lasted for 6 months and resolved spontaneously, without any specific treatment. The second one occurred 12 years ago. The headaches were of similar character; she was again hospitalized, an MRI showed meningeal enhancement and she was treated with IV antibiotics for 10 days. The third bout was less severe than the others and lasted for 3–4 months. There was no previous history of dural puncture.
On neurological examination, there was no fever, papilledema, meningeal signs or focal neurological deficits.
MRI of the brain with gadolinium (Fig. 1) revealed mild tonsillar ectopia (4.7 mm), flattening of the anterior belly of the pons and the pontomedullary sulcus, crowding of the area of the foramen magnum at the level of the cervicomedullary junction by the descending tonsils, prominent linear dural enhancement throughout the entire intracranial cavity, no hydrocephalus, and no leptomeningeal enhancement or parenchymal lesions. MR venography revealed no occlusive process of the dural sinuses or the deep venous system. Lumbar puncture revealed opening pressure of 30 mm H2O (lateral recumbent position) and no CSF evidence of inflammation, infection or neoplasia.
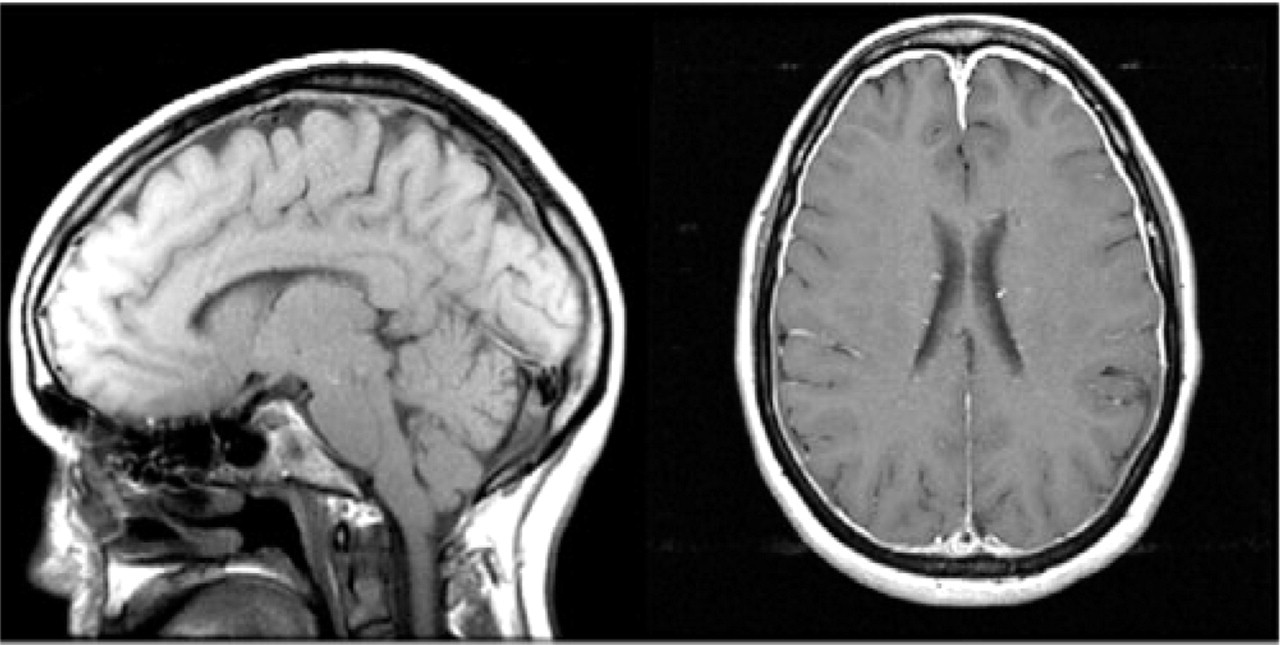
MRI of the brain with contrast demonstrating mild tonsilar ectopia, flattening of the pons, and linear dural enhancement of the entire cranial cavity.
Medical treatment with hydration, caffeine and dihydroergotamine resulted in no relief. Autologous lumbar epidural blood patch (EBP) also resulted in no resolution of the symptoms.
In an attempt to localize the suspected CSF leak, radionuclide cisternography with intrathecal administration of 0.5 mCi In-111 DTPA (diethylenetriamine penta-acetic acid) (Fig. 2) was performed. Post-procedural posterior planar images of the injection site and thoracolumbar region, followed by lateral, anterior and posterior planar images of the head and face and the thoracolumbar spine region at 4 and 24 h were obtained. They demonstrated an outpouching of the radionuclide in the region of the upper thoracic spine bilaterally at 4 h, which disappeared by 24 h, and slow ascent of the radiotracer without other focal abnormality.

Radionuclide cisternography demonstrates outpouching of the radionuclide in the region of the upper thoracic spine bilaterally, at 4 h. There was slow ascent of the radiotracer but no other focal abnormality.
In order to confirm the isotope cisternogram findings, MR imaging (sagittal T1-weighted imaging, sagittal fast spin-echo T2-weighted imaging and axial gradient echo images) of the entire spine was obtained, revealing no prominence of the epidural venous plexus. A heavily T2-weighted sequence (single shot fast spin echo (SSFE): TR 4000, TE 498, TI 0, 2.5 thk/3 sp., matrix 256/256) was able to identify prominent CSF leak at the level of the T1-T2 neural foramina, left more than right, which correlated with the radionuclide cisternogram findings, suggestive of possible tear at that level. In addition, there were prominent perineural CSF sleeves, not suggestive of CSF leak, at the levels of C7-T1, T10-T11 and L4-L5 bilaterally, which were not evident on routine MR images (Fig. 3). Differentiating between a dilated perineural sleeve (arachnoid diverticulum) and actual dural tear resulting in CSF leakage was done on the basis of the image appearance of the CSF collections. Dilated perineural sleeves had rounded distinct margins, while dural leaks had an irregular, linear appearance, without distinct margins. In addition, nerve roots were seen to traverse through the dilated perineural sleeve but not through a dural leak.

Comparison of MR myelography with conventional MRI at the same levels. First row: C7-T1 level. Second row: upper-mid thoracic level. Third row: lower lumbar level. CSF leak is noted at the C7-T1 level. Multiple prominent perineural CSF collections are noted at other levels.
After these studies, the patient refused further invasive procedures of any kind, including CT myelography, focal epidural blood patch or other form of targeted therapy.
Discussion
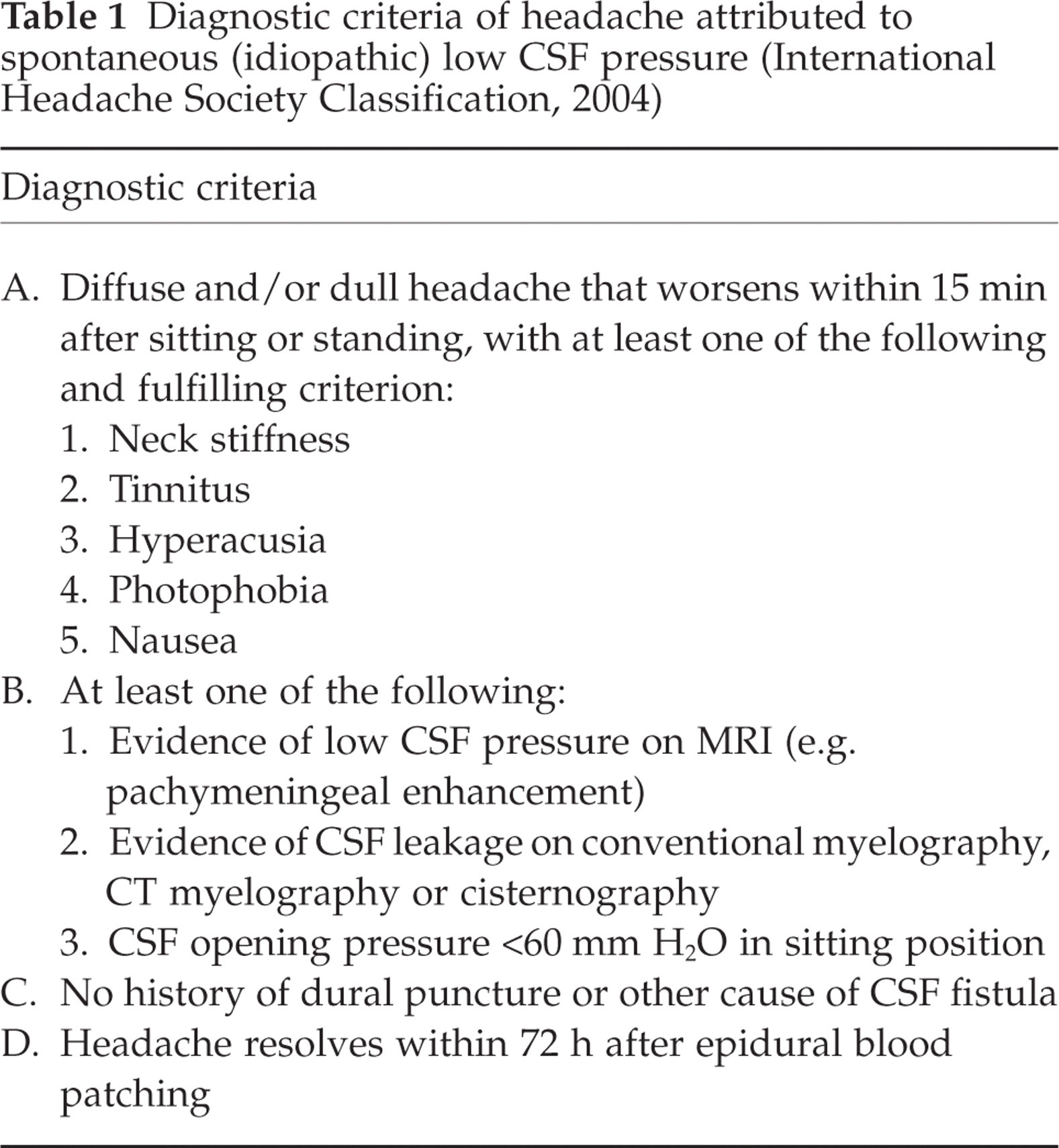
The described patient had the clinical and radiological features (criteria A-C) of spontaneous intracranial hypotension (Table 1). Similar to radionuclide cisternography, high-resolution MR myelography was able to define the site of CSF leak. She did not accept the performance of a targeted EBP, because of the potential complications, and as a result there is no confirmation of response to targeted therapy.
Diagnostic criteria of headache attributed to spontaneous (idiopathic) low CSF pressure (International Headache Society Classification, 2004)
The presence of intracranial hypotension was strongly suggested by radiological findings on MRI of the brain. The radiological appearance, typically consisting of dural thickening and enhancement, prominence of the dural sinuses, downward displacement of the brain, and subdural hygromas, is non-specific and does not provide any indication as to the aetiology of the hypotension and the level of the suspected CSF leak (2). Localization of the dural tear and CSF leak can be attempted by radionuclide cisternography, CT-myelography and MRI techniques. Our patient had evidence of CSF leak on both cisternography and MR imaging.
On cisternography, the oldest of all imaging techniques of CSF anatomy and physiology (3), a CSF leakage can be directly visualized if there is accumulation of radioactivity outside the subarachnoid space. The radiotracer may ascend slowly over the convexities or disappear early from the subarachnoid space and accumulate in the bladder. If there is no active leakage or if the size of the defect is smaller than the resolution of the technique, no direct evidence of the leak is seen (4). In cases of more than one dural defect, some of them may not be visualized, a fact that has obvious implications for treatment. On the other hand, CT myelography is considered to be the gold standard in the identification of the aetiology of spontaneous intracranial hypotension (SIH). In a single study, it can provide evidence of meningeal anatomical defects, precise location of extra-dural collections and relationship to bony structures. It is the most sensitive technique and can prove the existence of multiple concurrent CSF leaks that would potentially represent a contraindication for focused surgical treatment (5). Both CT myelography and radionuclide cisternography have potential drawbacks. The risk of ionizing radiation with CT is not negligible. The intrathecally administered agent can cause seizures or pial irritation (CT contrast) or is radioactive (radiotracer). Moreover, these techniques introduce an iatrogenic CSF leak that can further disturb CSF flow dynamics and result in worsening of the pre-existing orthostatic symptoms. The potential benefit of CSF sampling and analysis is unnecessary, as the constellation of symptoms is so specific that CSF analysis is not required.
Non-invasive modalities in SIH usually involve MR imaging. Conventional T2-weighted techniques usually reveal extra-arachnoid fluid collections, spinal meningeal enhancement, and dilation of the epidural venous plexus. Routine MRI techniques are less sensitive and precise than CT myelography as the interpenetration of solid and fluid structures throughout the spine makes identification of leaks more challenging. The administration of intrathecal gadolinium (gadolinium enhanced MR myelography) can facilitate the identification of enhancing CSF collections that are in continuity with the subarachnoid space (6).
In our patient, the addition of a heavily T2-weighted single shot fast-spin echo MR sequence assisted in the non-invasive localization of CSF leaks. This technique virtually erases all solid components and can visualize the CSF, wherever it is, regardless of the rate that it exits the subarachnoid space. It appears that SSFSE MR myelography can differentiate a dilated neural sleeve (arachnoid diverticulum) from an actual dural tear resulting in CSF leakage. High-resolution axial images are essential in achieving this. The appearance of the fluid collection seems to be important, as dilated neural sleeves typically have distinct round margins, while dural leaks have an irregular linear appearance, without distinct margins. In addition, on axial images nerve roots are seen to traverse through the dilated neural sleeve but not through a dural leak (7). Both these imaging characteristics are better seen on CT myelography, which remains the gold standard imaging modality in this condition, as it additionally demonstrates the actual extravasation of contrast outside the thecal space. Similar MR CSF-depicting sequences have been used in the evaluation of cerebellopontine angle lesions and trigeminal neurovascular compression (8). The additional SSFSE technique, which has been used mostly in paediatric neuroimaging (9, 10), ensures a short duration of scanning, minimizes movement artifact and enables adequate resolution. To our knowledge, this is the first application of this technique in the evaluation of SIH. Further studies are required in order to compare the sensitivity and specificity of our technique with that of CT myelography, as well as to prove a treatment benefit.
A limitation of the SSFSE MR myelography is that it allows, by default, only a static image of a dynamic process and it cannot reveal the actual dural defect or the diffusion of CSF into the extra-arachnoid space. Similar limitations apply to all non-invasive and invasive imaging modalities. The ultimate confirmation of a leakage site can only be provided by resolution of the headache syndrome after a successful targeted intervention.
Our patient did not respond to conservative treatment. The initial radionuclide cisternography demonstrated a single responsible level of CSF leakage. This was the primary level demonstrated by SSFSE-MR myelography as well. It is likely that the patient would have benefited from targeted therapy (either focal EBP or fibrin glue application or operative approach). On the basis of the agreement between radionuclide cisternography and our technique, we propose that targeted therapy (i.e. EBP or fibrin glue application) may be attempted, based solely on MR myelography. This is a relatively simple procedure with minimal morbidity when performed by experienced physicians, and in cases of failure MR myelography can guide subsequent CT myelography to a specific level of the neuraxis. Our patient did not accept any form of targeted therapy, a fact that did not allow the definite confirmation of the level of the CSF leak.
In conclusion, the syndrome of SIH is usually associated with the presence of a persistent CSF leak. Routine lumbar EPB are usually ineffective as the responsible site is usually located in the cervical or upper thoracic region. Invasive diagnostic modalities, such as CT-myelography and cisternography, can increase the rate of CSF loss and prolong recovery. SSFSE MR myelography is safe, non-invasive, and can provide CSF images that are equal or even superior to traditional cisternography. A larger comparative study is required to establish that MR myelography is comparable with current techniques and capable of independently guiding treatment.