
Abstract
Migraine is a primary headache condition that is not caused by another disorder. Focal brain lesions have been noted to cause headaches that might otherwise be classified as migraines.
The association of midbrain lesions and migraine has been described in the literature, as has migraine associated with midbrain malformations. In this report we describe a patient with new-onset migraine-like headache with aura, and a ruptured midbrain arteriovenous malformation (AVM).
Case report
In 1996, at the age of 30, this patient began having headaches that were accompanied by right upper extremity weakness. Two months later, he was diagnosed with a midbrain cavernous haemangioma that bled and he was hospitalized for 1 week. An intraventricular shunt was placed in 1997. Magnetic resonance imaging (MRI) demonstrated a lesion in the dorsal left midbrain and the upper pons with old cystic components, one of which extended to the fourth ventricle. Partial resection of his brainstem lesion was performed in 1998. The final pathology report was an arteriovenous/cavernous malformation. The patient had no prior history of migraine and no family history of migraine.
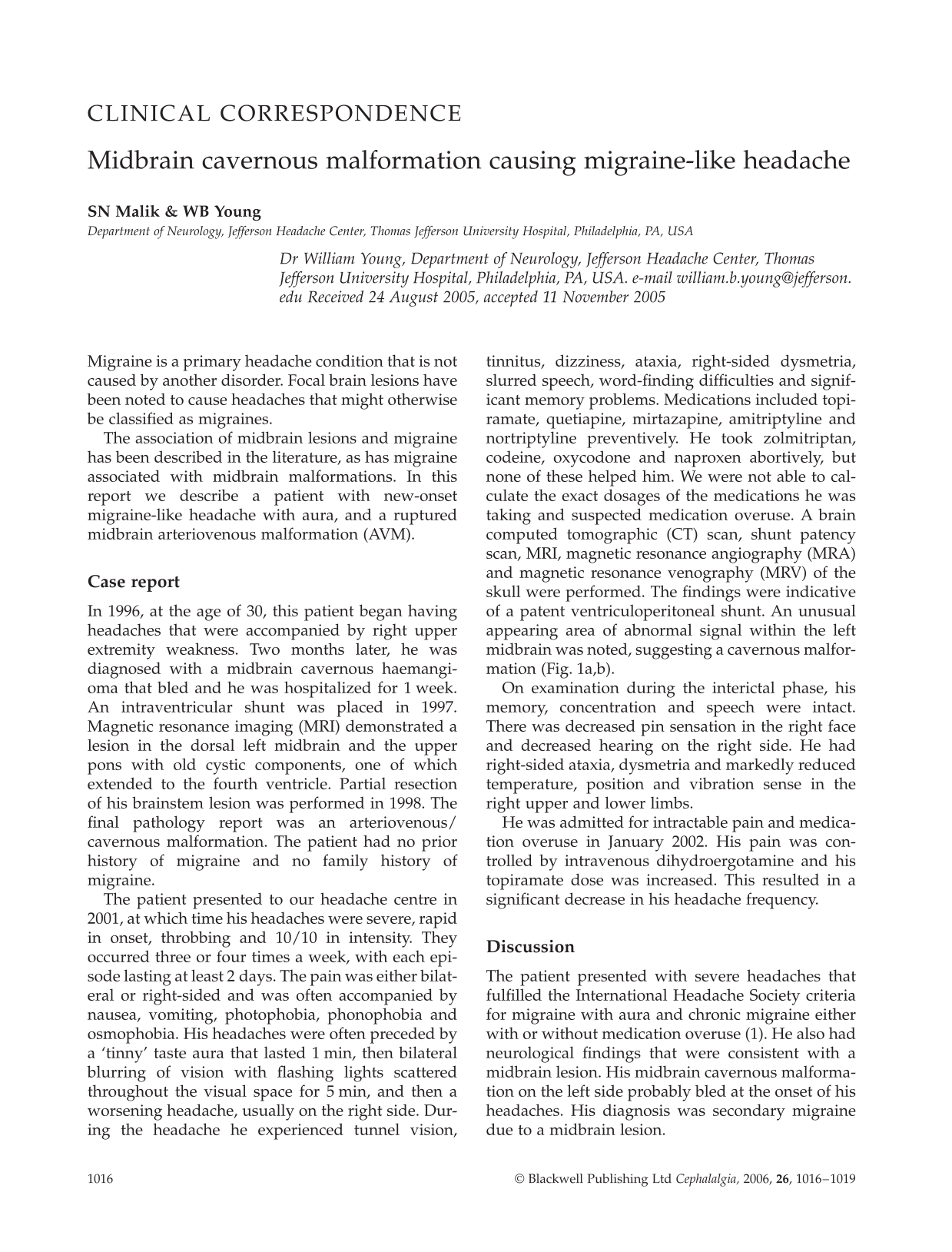
The patient presented to our headache centre in 2001, at which time his headaches were severe, rapid in onset, throbbing and 10/10 in intensity. They occurred three or four times a week, with each episode lasting at least 2 days. The pain was either bilateral or right-sided and was often accompanied by nausea, vomiting, photophobia, phonophobia and osmophobia. His headaches were often preceded by a ‘tinny’ taste aura that lasted 1 min, then bilateral blurring of vision with flashing lights scattered throughout the visual space for 5 min, and then a worsening headache, usually on the right side. During the headache he experienced tunnel vision, tinnitus, dizziness, ataxia, right-sided dysmetria, slurred speech, word-finding difficulties and significant memory problems. Medications included topiramate, quetiapine, mirtazapine, amitriptyline and nortriptyline preventively. He took zolmitriptan, codeine, oxycodone and naproxen abortively, but none of these helped him. We were not able to calculate the exact dosages of the medications he was taking and suspected medication overuse. A brain computed tomographic (CT) scan, shunt patency scan, MRI, magnetic resonance angiography (MRA) and magnetic resonance venography (MRV) of the skull were performed. The findings were indicative of a patent ventriculoperitoneal shunt. An unusual appearing area of abnormal signal within the left midbrain was noted, suggesting a cavernous malformation (Fig. 1a,b).

(a,b) Magnetic resonance imaging demonstrating caudal midbrain lesion.
On examination during the interictal phase, his memory, concentration and speech were intact. There was decreased pin sensation in the right face and decreased hearing on the right side. He had right-sided ataxia, dysmetria and markedly reduced temperature, position and vibration sense in the right upper and lower limbs.
He was admitted for intractable pain and medication overuse in January 2002. His pain was controlled by intravenous dihydroergotamine and his topiramate dose was increased. This resulted in a significant decrease in his headache frequency.
Discussion
The patient presented with severe headaches that fulfilled the International Headache Society criteria for migraine with aura and chronic migraine either with or without medication overuse (1). He also had neurological findings that were consistent with a midbrain lesion. His midbrain cavernous malformation on the left side probably bled at the onset of his headaches. His diagnosis was secondary migraine due to a midbrain lesion.
This case illustrates that migraine-like headaches with aura can be caused by a malformation in the midbrain. The occurrence of new headaches in a previously normal patient associated with a cavernous malformation haemorrhage suggests that lesions in the midbrain or in the periacqueductal grey (PAG) can cause secondary migraines.
This is one of only a few reported cases of secondary migraine caused by an AVM near the PAG. Midbrain lesions are associated with migraine-like headaches. Two reports from the pre-CT era documented a midbrain AVM and a fourth ventricle AVM associated with migraine-like headaches (2). One of six patients reported by Bruyn with AVM and migraine had AVMs involving the midbrain (2). Bruyn concluded that the symptoms of migraine due to intracranial malformations include late-onset migraines, absence of family history and neurological deficits. In 2001, Goadsby reported a female patient who had new-onset, frequent, migraine-like headaches with left-sided vascular malformation in the PAG that bled at the onset of the headaches (3). In 2003, Afridi et al. reported another female patient who had new-onset migraine with left pontine cavernous malformation (4). Similarly, Katsarava presented a case of a patient with symptomatic, strictly right-sided migraine with a pontine cavernoma affecting the left nucleus raphe magnus (5).
Vascular malformations in other brain areas have also been associated with new-onset migraine-like headaches. Most case reports involve the occipital, parietal or temporal lobes (6, 7). In 1975, Waltimo et al. described the association of occipital AVMs with migraines (8). Bruyn et al. has shown that in addition to midbrain AVMs, occipital and temporal AVMs are also associated with migraine-like headaches (2).
Other lesions in the PAG are associated with migraine. Lance and Anthony speculated about the involvement of the brainstem in migraine because of the presence of autonomic symptoms such as nausea and vomiting during acute migraine attacks (9). The role of the brainstem in migraine was initially demonstrated by Goadsby et al. in laboratory studies in 1982 (10). They performed electrical stimulation of locus coeruleus in monkeys which caused intracranial vasoconstriction and extracranial vasodilation that resembled the vascular changes of migraine. Later cases showed that non-migraineurs developed migraine-like headaches after stimulating electrodes were implanted into the PAG (11, 12). Weiller et al. demonstrated positron emission tomography (PET) activation of the upper pons and midbrain in nine migraineurs even after the pain had resolved with the use of sumatriptan (13). Bahra showed dorsal rostral brainstem activation on PET study during migraine without aura (14). The belief that the PAG may be an important area of dysfunction in migraine is further supported by Welch, who observed 17 patients with episodic migraine with or without aura and concluded that they had iron homeostasis impairment in the PAG (15). Activation of the red nucleus and substantia nigra in migraine with aura was observed by Welch (16). Further functional MRI studies of 26 patients with migraine with aura have shown that migraine induced by repeated visual stimulation shows activation in the red nucleus and substantia nigra (17), suggesting that brainstem structures are a part of neuronal network during an attack (13). Multiple sclerosis plaques in the PAG are also associated with new-onset migraine, whereas the overall burden of plaques does not correlate with migraine (18–20). A recent PET study by Afridi et al. showed activation of the dorsal pons during the ictal and interictal stages of migraine (21), as well as areas of deactivation in the contralateral pons in the ictal stage.
Three of the reported cases including this one suggest that a unilateral headache may be contralateral to a dysfunctional midbrain structure. In migraine induced by glyceryl trinitrate and studied with H2 15O-labelled PET, dorsal pontine activation occurs ipsilateral in the right-sided and left-sided groups, and bilateral, with a left preponderance, in the bilateral headache group (22). The PET study also showed development of migraine-like headache contralateral to the area of abnormality (13).
The PAG inhibits traffic from trigeminovascular afferents. A lesion in the area of PAG may cause dysfunction and this could lead to increased trigeminovascular traffic (23). This disinhibition of nociceptive trigeminovascular afferents could give rise to migraine-like headaches (5, 23). This fills a gap between impairment in the PAG antinociceptive activity and sensitization of trigeminal nociception. One explanation of the findings is that structures in the midbrain PAG promote contralateral migraine and suppress ipsilateral migraine. Destructive midbrain lesions disinhibit the ipsilateral structures activated during migraine and suppress contralateral function.
Our case is the first to demonstrate a midbrain lesion causing migraine aura. Aura arises from cortical spreading depression (CSD) and migraine arises from trigeminal sensitization (24). These have been linked in an animal model in which CSD triggers hyperaemia on the surface of the brain with neural connections running through the brainstem (25). How a midbrain lesion may lead to aura remains unclear. Cao demonstrated on fMRI that occipitally generated aura symptoms may be preceded by brainstem changes of visually triggered migraine (17).
These cases teach us about the potential causes of migraine and reinforce the concept that midbrain structures are important in migraine.