
Abstract

Despite the guidelines for the treatment of aneurysms or spinal tumours having been described, the coexistence of both pathologies makes their management difficult. In fact, when subarachnoid haemorrhage (SAH) occurs, a correct surgical assessment of the spinal tumour and planning of suitable anaesthesiology are necessary to reduce the risk of cerebral vasospasm (CVS) and subsequent ischaemic complications (1, 2). This holds true not only in the neurosurgical field but in any other emergency surgical practice, requiring general anaesthesia, after early SAH.
This paper reports the case of a patient diagnosed with cauda equina syndrome caused by lumbar schwannoma who presented with sudden cephalalgia.
Case report
A 73-year-old female patient, suffering from hepatitis C, nodal tachyarrhythmia and arterial hypertension of World Health Organization (WHO) grade II, 3 weeks before hospitalization suddenly presented with spastic paraparesis with distal involvement and predominance of the motor deficit in the right limb. Neurological examination revealed a hyper-reflexia of patellar reflexes with predominance on the right side, bilateral absence of Achilles and middle plantar reflexes, sellar anaesthesia, bilateral hypoaesthesia of the hypogastric region and iliac fossa, and painful thermo-tactile hypoaesthesia of the legs with predominance on the right side. Anal reflex was hypotonic and concomitant bladder dysfunction was present.
Spinal magnetic resonance imaging showed an intradural hyperdense lesion at T12-L1 requiring early removal (Fig. 1). Three hours before the operation the patient experienced sudden thunderclap cephalalgia and vomiting without sentinel signs. The headache was of high intensity with a predominant frontotemporal bilateral distribution. There was no loss of consciousness. A mild headache persisted for about 10 days.

T12-L1 tumour.
The patient was of Hunt–Hess grade II. Emergency computed tomographic scan revealed blood in the basal cisterns. Cerebral angiography revealed a small aneurysm (about 4 mm) of the anterior communicating artery (ACoA) (Fig. 2). Nimodipine was administered to prevent arterial vasospasm. Using a right femoral approach with a 6-Fr microcatheter under general anaesthesia, two Guglielmi Detachable Coils (GDC) 10 were detached into the aneurysm bag until tight coil packing was achieved.

Anterior communicating artery aneurysm: pre-embolization.
Aneurysm obliteration was evaluated by immediate postembolization angiography in multiple projections and no contrast filling of the aneurysm body, neck or dome was observed (Fig. 3). Propafenone was administered during the embolization and amiodarone was added to propafenon in the following days.

Anterior communicating artery aneurysm: post-embolization.
Calciparin 0.5 g twice daily for 3 days, then reduced to 0.2 g twice daily for another 5 days, was administered. The microcatheter was left until normalization of partial thromboplastin time levels and arterial pressure was maintained over 140 mmHg (1, 2).
After coiling, immediate and long-term outcomes were good apart from a cauda equina syndrome.
Cerebral blood flow (CBF) velocity was monitored by transcranial Doppler (TCD). However, given the higher vasospasm risk, a TCD measurement of ACoA velocities was performed more frequently than usually required. No increasing of peak mean velocity was observed.
Even though an emergency tumour removal would have been necessary to obtain a good outcome, the authors decided to postpone surgery since the haemodynamic variations might have induced cerebral vasospasm. The patient was at an American Society of Anesthesiology (ASA) grade III risk rate.
Eleven days after coiling, a T12-L1 laminectomy was performed and a hard and yellowish grey intradural mass was revealed (Fig. 4). The tumour was detached from the dura and then shifted towards the right before being completely removed. Dura was stitched and reinforced with fibrin glue. An epidural drainage was left in aspiration mode.
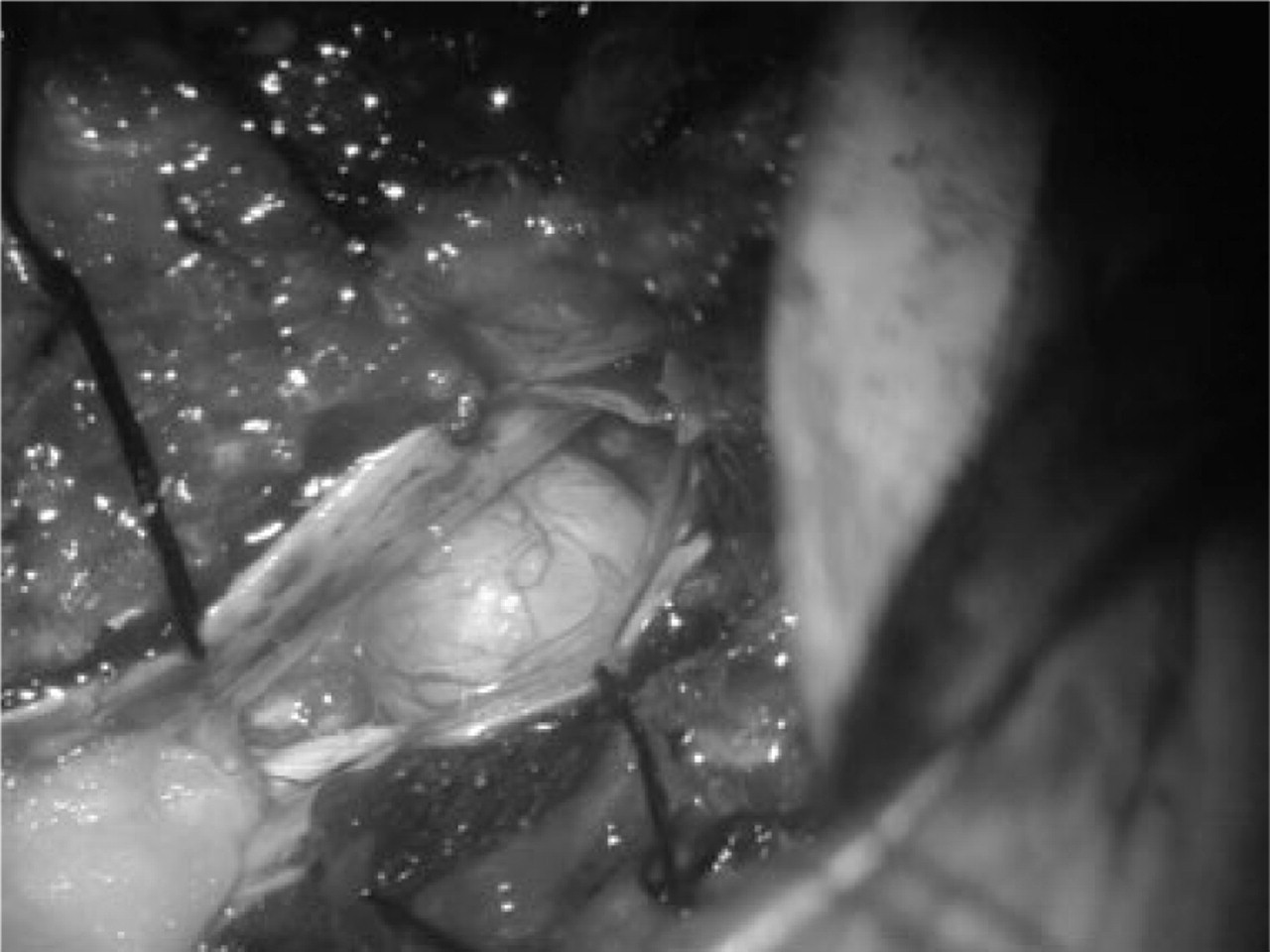
T12-L1 tumour (intraoperative).
Midazolam 1.5 mg and fentanyl 100 µg were administered before induction of general anaesthesia (GA) that was made i.v. with sodium thiopental and, after succinylcholine, the patient was intubated and mechanically ventilated in O2/air (fraction of inspired oxygen = 0.4). GA was maintained using sevoflurane as hypnotic, remifentanyl as opiod and cis-antracurium as curare. Heart rate, invasive blood pressure (IBP), central venous pressure (CVP), O2 saturation, tidal CO2 and oesophageal temperature (°T) were monitored throughout the operation. IBP was maintained in the range 85–95 mmHg. CVP, measured with a central venous catheter inserted in the right jugular vein, was maintained at 10 mmHg (1, 2) and °T at the end of the operation was close to the basal temperature by active warming with a forced air blanket. About 10 min from stopping the administration of anaesthetic drugs and antagonization of residual curarization with intrastigmine, the patient awoke without complications.
Therapy for postoperative pain was achieved using tramadol and ketorolac i.v. in continuous mode for the first 48 h.
Histological tests on a spinal surgical fragment reported a type B Antoni schwannoma (Fig. 5). After surgery, electromyography of the legs showed bilateral loss of motor units in musculus iliotibialis, anterior tibial muscle, gastrocnemius and short extensor muscle of toes.

Type B Antoni schwannoma (H&E, × 200).
Discussion
Cauda equina syndrome by lumbar schwannoma is an indication for emergency surgery, considering that this tumour may be removed completely, usually without recurrences (3).
In 1996, Asahara reported a review of 42 cases of spinal schwannomas analysing the therapeutic results to investigate the factors affecting clinical outcome. The delay in diagnosis and duration of the symptoms were significantly greater in cases of lumbar lesions compared with cervical and thoracic ones (4).
Even though an emergency tumour removal would have been necessary to obtain a good outcome in the reported case, it was decided to postpone surgery because deliberate hypotension might have induced cerebral vasospasm. Vasospasm prevention after aneurysmal SAH is the most important problem of the neurointensive care in ruptured aneurysms. According to the data of the American Heart Association (AHA), the resolution of vasospasm after SAH develops over 4 weeks (1). However, in the presence of cauda equine syndrome, schwannoma removal was postponed and performed only 11 days after coiling.
During the operation, IBP was maintained in the range 85–95 mmHg because the patient was hypertensive and a relative hypertensive state is recommended to contrast with the onset of vasospasm (1, 2). Following our therapeutic algorithm based on the study reported by the AHA and Treggiani et al. (1, 2), Figure 6 shows the incidence of CVS after the SAH (blue trace) compared with the percentage of patients who may present a good postoperative course and outcome if they receive no anaesthesiological hypotension intraoperatively (red trace). Patients with hypotension, on the other hand, may present a worse surgical outcome (yellow trace).

Trend of cerebral vasospasm compared with positive surgical outcome with and without relative hypotension.
During postoperative follow-up, in the intensive care unit, TCD monitoring of ACoA blood velocities was performed. The choice of TCD ultrasonography in the measurement of cerebral blood flow velocity is based on Joanna's observational study which assessed the impact of routine TCD ultrasound monitoring on the diagnosis, management and outcome of delayed ischaemic neurological deficit after SAH.
Given that TCD ultrasound findings correspond closely to the results obtained using intra-arterial angiography (5), routine TCD ultrasound monitoring is established as the first useful tool in the early diagnosis of cerebral vasospasm with specificity between 88.6% and 97.6% (6). Diagnostic sensitivity decreases from 83.6% for the middle cerebral artery to 40.6% for ACoA.
It must be acknowledged that TCD demonstrates high specificity but its sensitivity is too low for aneurysms located far from the middle cerebral artery bifurcation (1, 2).
In 1997, Winking reported a good correlation, after SAH, between blood flow velocity in TCD and levels of immunoreactive cysteinyl-leukotrienes (cys-LT) in cerebrospinal fluid (CSF). Normalization of TCD values is accompanied by decreased levels of CSF cys-LT. Several studies have indicated that cys-LT, produced by lipid peroxidation and enhanced arachidonic acid metabolism after blood–brain cell contact, has the capacity to constrict arterial vessels in vivo and in vitro, suggesting their involvement in the pathogenesis of cerebral vasospasm (7).
Considering that the increase of cys-LT is earlier and more sensitive compared with TCD ultrasonography, in future its evaluation may become standard in the early diagnosis of arterial spasm.
Nowadays, urokinase injection via cisternal drainage seems the most promising treatment to achieve a reduction of symptomatic vasospasm, even if a significant increase in the incidence of hydrocephalus has been observed (8).
In 1994, Saveland's study on 275 patients concluded that arterial hypertension does not influence the outcome of aneurysmal SHA (9). The site of delayed cerebral ischaemia after vasospasm seems not to be related to the location of the SAH (10).
SAH and risk of cerebral vasospasm should not be considered absolute contraindications to spinal surgery. Clinical management and surgical planning which take into account the factors analysed in this paper may improve the outcome of these unusual cases.
In the presence of spinal tumour complicated by bladder dysfunction, emergency tumour removal would have been necessary to obtain a good outcome but, in the described case, spinal surgery was postponed to avoid cerebral ischaemia. The patient's outcome demonstrated that subarachnoid haemorrhage may not be considered a total contraindication to spinal surgery if successful embolization of the aneurysm responsible for intracranial bleeding can be achieved and the haemodynamic status of the patient can be carefully and closely controlled at the time of surgery.