
Abstract
A patient presented with a painful, pulsating nodosity with marked tenderness on the right side of her neck. Cervical magnetic resonance imaging (MRI) exhibited pathological signal changes in the perivascular tissue of the carotid bifurcation area and around the external carotid artery. Similarly, Doppler sonography revealed an echo-poor wall change with outward bulging and slight narrowing of the affected vessel lumen. The clinical symptoms and our findings led to the diagnosis of carotidynia. We proposed that cervical MRI and Doppler sonography could be used for diagnosing carotidynia.
Introduction
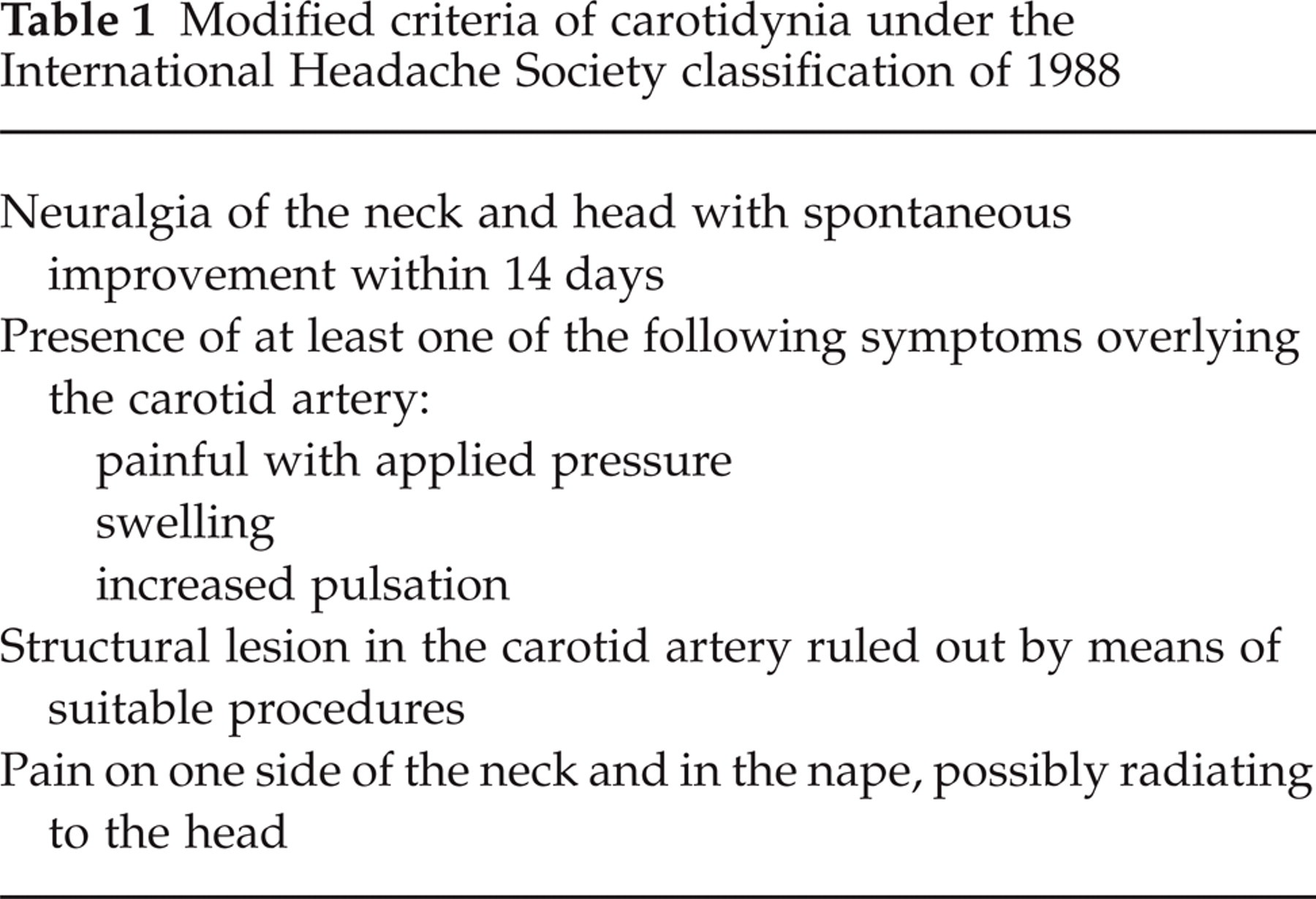
T. Fay proposed the designation of carotidynia in 1927 for atypical neuralgia in the neck and face accompanied by sensitivity of the carotid artery to pressure (1). Consequently, carotidynia was soon accepted as a distinct disease (2). The International Headache Society (IHS) defined the syndrome in 1988 as shown in Table 1 (3).
Modified criteria of carotidynia under the International Headache Society classification of 1988
Some authors were convinced that carotidynia was frequently overlooked or misdiagnosed (4). Later, the independent existence of this headache syndrome was generally doubted (5). However, highly diverse headache and neck pain syndromes were ascribed to carotidynia even when they did not meet the above criteria. Therefore, the second extended IHS classification of 2004 no longer refers to carotidynia as an independent pathological entity (6). Several current reports, which mainly describe radiological findings of putative carotidynia, suggest that the topic of carotidynia is still open for discussion (7–12).
Case report
A 49-year-old woman presented with a painful, pulsating nodosity on the right side of her neck, which had appeared a few days earlier without any previous trauma. The pain originating from the pulsating nodosity was reported in the ipsilateral soft tissues of the neck and sometimes irradiated to the right chin and ear. The pain was constant, of mild to moderate intensity, and fluctuated from a dull pressure to throbbing exacerbations. Swallowing and coughing were difficult and painful. There was a local palpable, pulsating, roundish structure with a diameter of 2 cm, which was painful when pressure was applied. General medical and neurological findings were otherwise normal.
Doppler sonography revealed an echo-poor thickening of the distal right common carotid artery (CCA) wall that extended to the start of the right external carotid artery (ECA) (Fig. 1), which it almost completely circularly constricted. The change in the wall bulged slightly outwards, but did not cause any significant acceleration of the blood flow. The cranial magnetic resonance imaging (MRI) was normal. However, the transverse T1-weighted slices of a neck MRI showed a short diffuse perivascular contrast medium enhancement in the CCA close to the bifurcation and the proximal ECA (Fig. 2). The fat-suppressed T2-weighted sequences revealed perivascular oedema in this region (results not shown). There were no intramural haematoma, double lumen, or intimal flap present. Contrast enhanced (CE) MRI angiography of the neck vessels revealed normal flow signals and, in particular, no relevant narrowing of the right carotid artery lumen (results not shown).

B-image sonography of the right carotid bifurcation in longitudinal section: echo-poor wall changes and constriction of the lumen of the distal common carotid artery (CCA) and the proximal external carotid artery (ECA) (arrow). ICA, Internal carotid artery.

Axial T1 SPIR sequences after contrast medium. Perivascular contrast medium enhancement around the proximal external carotid atery (arrow).
The combination of symptoms, clinical course and findings indicated a diagnosis of carotidynia. Anti-inflammatories (Paracetamol and Ibuprofen) were administered to treat the pain and provided rapid relief. All the symptoms regressed completely within a few days. The pressure-sensitive nodosity on the right side of the neck was no longer palpable 3 days after admission, although the Doppler sonography findings remained unchanged after 1 and 3 weeks. However, 3 weeks after the condition's onset the MRI findings were substantially less (results not shown).
Discussion
The symptoms initially described by Fay and Roseman as characteristic of carotidynia applied to our patient (1, 2). The criteria of the earlier IHS classification (Table 1) in terms of clinical symptoms and course also indicated a diagnosis of idiopathic carotidynia (3). The pathological findings identified in our patient by MRI and Doppler sonography disagreed with these former criteria to some extent, as the 1988 IHS classification presumed that there were no structural changes present in ‘idiopathic carotidynia’.
There have been recent reports indicating that pathological MRI findings do occur in carotidynia (8, 9, 11). Typically the T1-weighted sequences, after administration of contrast medium, revealed thickening and enhancement of the affected carotid artery periadventitial soft tissue (7, 11). Additional T2 spectral presaturation with inversion recovery sequences were performed in a few cases, which revealed a narrow, perivascularly raised signal corresponding to an inflammatory concomitant oedema as we observed in our patient (8, 11). The MR angiograms of the neck vessels, on the other hand, were normal in every case without any indication of substantial lumen constriction (7, 8). A double lumen, intimal flap, or intramural haematoma referring to a dissection were not present in our patient or any of the reported cases, which is the most important differential diagnosis of carotidynia.
The vascular changes, which extended over a length of 15–35 mm, always affected the distal segment of the CCA and the carotid bifurcation; the start of the internal carotid artery was also occasionally involved (7). The spreading of the vascular changes to the proximal ECA, as was observed in our patient, has not been previously reported. Analogous to the MRI findings, Doppler sonographic changes have also recently been described in carotidynia (9, 10, 12). The vessels involved had echo-poor wall thickening with a slight constriction of the lumen and an outward bulging as we noted in our patient. However, no acceleration of flow was recorded. These observations correlate well with the normal MR angiography findings.
Recently, an underlying non-specific vascular inflammation was demonstrated histologically to be involved in carotidynia (13). This fact may explain why in some cases anti-inflammatory agents, such as non-steroidal anti-inflammatory drugs and corticosteroids, were effective in treatment.
Usually the symptoms of carotidynia fade away completely within a short time, and even the vascular changes observed by MRI and Doppler sonography are capable of involution. This was confirmed by progress checks of the patients in the discussed literature (7–12) and our own case.
The case presented here and previous observations (7–12) underscore the existence of carotidynia as an independent disease. Accordingly, typical clinical symptoms should suggest the rare differential diagnosis of carotidynia. Cervical MRI and Doppler sonography are the modalities of choice for confirmation of the presumed carotidynia diagnosis.