
Abstract
Neurotrophins, such as brain-derived neurotrophic factor (BDNF) and nerve growth factor (NGF), have been implicated in the generation and modulation of pain. To investigate whether alterations in neurotrophin levels can be detected in subjects suffering from nociceptive disorders, such as primary headaches, we determined the peripheral (platelet and plasma) levels of BDNF and NGF in patients suffering from migraine, with or without aura, or cluster headache (CH), in the interictal phase, and in healthy volunteers. All primary headaches patients studied showed significantly decreased platelet levels of BDNF (migraine vs. controls
Introduction
The pathophysiological mechanisms that underlie primary headache disorders, such as migraine and cluster headache (CH), are complex and not yet fully clarified (1). While there is today little doubt that activation of the trigeminovascular system (TGVS) is responsible for the headache pain (2), the primary mechanisms, probably centrally mediated, leading to its activation and the generation of pain are still largely obscure. In addition, although current evidence supports the view that altered sensory processing associated with peripheral and central sensitization plays a pivotal role in determining the pain response following the activation of the TGVS (3), the cellular and molecular mechanisms of this process in primary headache sufferers remain largely unknown.
Neurotrophic factors, such as the nerve growth factor (NGF) and brain-derived neurotrophic factor (BDNF), are now emerging as important modulators of nociceptive function in adulthood (4). Although known primarily for their role in neuronal development, NGF is found in many tissues and cells—including brain, meninges and cerebrospinal fluid (CSF)—in adult rodents and humans (5–7), while BDNF is expressed throughout the CNS as well as in the periphery, preferentially in small and medium-sized sensory neurons expressing NGF receptors (8). Peripheral noxious stimuli, such as trauma and inflammation, up-regulate NGF in the affected tissue as well as BDNF in the sensory ganglia, in a NGF-dependent fashion (4); these changes intimately contribute to the sensitization of the peripheral and central nociceptive pathways towards subsequent incoming stimuli (9). However, whilst peripheral NGF contributes substantially to inflammatory and, probably, neuropathic pain inducing the sensitization of peripheral nociceptors, BDNF released within the CNS acts as a central pain modulator at both spinal and supra-spinal level contributing to the central sensitization, presumably by modulating, at least in the spinal cord, the activation of glutamatergic, N-methyl-d-aspartate (NMDA), receptors (10).
Despite the known role of neurotrophins in pain and the multiple sites implicated in the mechanisms of neutrotrophin-induced pain modulation, almost no information is available on the involvement of neurotrophic factors in primary headaches. So far, only one study has shown increased NGF concentrations in the CSF of patients with chronic daily headache (11). However, while this study is in line with the observation that intracerebroventricular infusion of NGF induces dull constant pain in humans (12), peripheral or CSF changes in NGF or other neurotrophins, in particular BDNF, have not been assessed in the different types of primary headaches.
A peripheral site where neurotrophic factors can be found and measured is represented by blood platelets. These cells, long reported to be functionally responsive to exogenous NGF (13), are also currently regarded as the main reservoir of circulating BDNF (14). Indeed, human platelets contain relatively large quantities of BDNF, which is specifically released upon agonist stimulation (15). Platelets, on the other hand, capture and store virtually all the circulating serotonin and, as such, have been extensively used for the study of 5-HT-related alterations in headache pathogenesis (16). It follows that platelets represent an ideal tool for studying peripheral neurotrophic factor levels, particularly BDNF, besides serotonin and its main metabolite 5-hydroxyindoleacetic acid (5-HIAA) in primary headaches.
The aim of the present study was therefore to investigate possible alterations in peripheral (platelet and plasma) levels of BDNF and NGF in patients affected by migraine, with (MA) or without aura (MoA), and CH, and to verify platelet levels of 5-HT and its main metabolite 5-HIAA in the same clinical settings.
Materials and methods
Subjects
Patients were recruited among those attending the Headache Centre of the Neurological Institute ‘C. Mondino’, Pavia, Italy. The diagnosis of headache type was made according to the criteria of the International Headache Society (17) and all patients included had been suffering from headache for at least 1 year. Patients with a history of cardiovascular disease, major depression, hypertension, drug or alcohol abuse, or other apparent diseases were excluded from the study. The study comprised 60 patients suffering from migraine (27 MA and 33 MoA) and 14 patients affected by CH, evaluated during the active period (Table 1). All patients were examined during a headache-free period: migraineurs had been pain-free for at least 1 week and remained pain-free for at least 3 days after the test; CH patients were pain-free for at least 8 h and remained pain-free for at least 3 h after the test. Patients were instructed to complete a daily diary for the detection of headache attacks. Pain intensity was graded hourly on a 3-point scale (1 = mild, does not impair daily activities; 2 = moderate, may inhibit, but does not prohibit daily activities; 3 = severe, prohibits daily activities). All women participating in the study were in the follicular phase of their menstrual cycle. The control group included 57 age- and sex-matched healthy subjects (Table 1), none of whom suffered from migraine or CH or had more than two episodes/year of tension-type headache. Patients and controls had not taken any medication (analgesics, non-steroidal anti-inflammatory drugs and 5-HT-related drugs) for at least 7 days prior to the study. For CH patients, only symptomatic treatment with oxygen for inhalation was permitted in the 7 days preceding the examination. The local ethics committee approved the study protocol and all participants gave written informed consent before entering the study.
Demographic and clinical characteristics of subjects participating in the study.

MA, Migraine with aura; MoA, migraine without aura; CH, cluster headache.
Sample preparation
Venous blood (30 ml) was drawn, without tourniquet, from the antecubital vein of fasting patients and controls, between 08.00 h and 09.00 h and collected directly into vacuum tubes, where it was mixed 9 : 1 with 0.129
BDNF and NGF assay
Platelet pellets were re-suspended in 1 ml PBS and sonicated on ice (three cycles of 20 s, each separated by 10 s) (Labsonic 2000; B. Braun, Melsungen, Germany), at middle power output. Platelet lysate was centrifuged at 12 000
5-HT and 5-HIAA assay
Platelet concentrations of 5-HT and 5-HIAA were measured by high-performance liquid chromatography (HPLC). Before HPLC assay, platelet pellets were re-suspended in 900 μl of ice-cold HClO4 (0.1
Statistical analysis
Statistical analysis was performed using InStat software (Instant Biostatistics, Version 3.0 for Windows; GraphPadTM Software, Inc., 1990–98). All variables were tested for normal distribution (Kolmogorov and Smirnov normality test) and most of them failed the test with
Results
Detectable levels of BDNF were found in all platelet and plasma samples tested. Absolute levels of BDNF were more elevated in platelets than in plasma, which is in agreement with the current notion that platelets are the main reservoir of circulating BDNF (15). As shown in Fig. 1, platelet levels of BDNF were significantly lower in all three groups of headache sufferers compared with controls (MA and MoA vs. controls
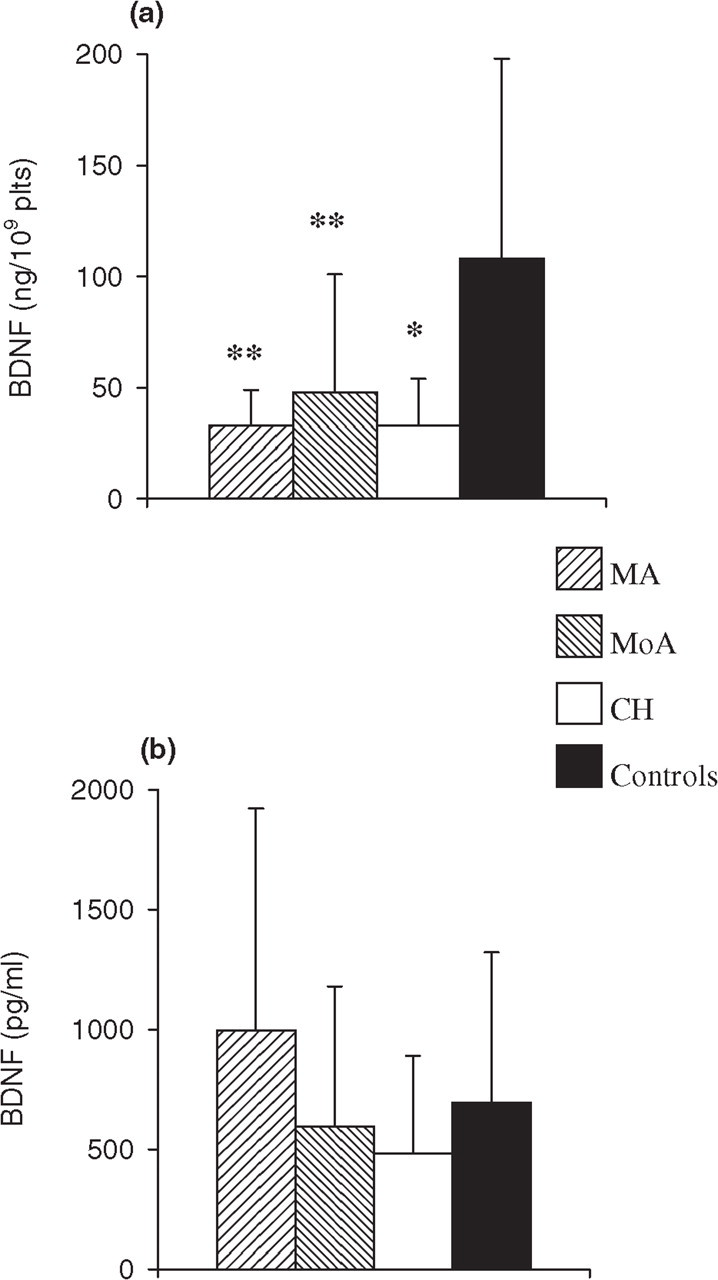
Platelet (a) and plasma (b) levels of brain-derived neurotrophic factor (BDNF) in patients suffering from migraine with aura (MA,
Figure 2 shows mean NGF levels found in the platelets and plasma of all subjects considered. While NGF was present, as expected, in plasma at concentrations much lower than BDNF, small but significant amounts of NGF were also found in platelets. This latter finding, to our knowledge not previously reported, is not a consequence of aspecificity of the assay system employed, since NGF levels found in plasma and other tissues or cells (data not shown) were, at all times, in a range comparable to that previously reported (18, 19). A significant reduction was observed in platelet NGF of MA and MoA patients compared with healthy controls (MA and MoA vs. controls

Platelet (a) and plasma (b) levels of nerrve growth factor (NGF) in patients suffering from migraine with aura (MA,
In line with previous studies (16, 20, 21) and as reported in Fig. 3, platelet levels of both 5-HT and 5-HIAA were significantly higher in all the three groups of headache sufferers, with respect to the control group.

Platelet levels of 5-HT (a) and 5-hydroxyindoleacetic acid (5-HIAA) (b) in patients suffering from migraine with aura (MA,
Discussion
In an attempt to verify whether neurotrophin-related mechanisms are involved in primary headaches, we investigated whether changes in peripheral circulating BDNF or NGF occur in subjects affected by MA, MoA and CH. Interestingly, we found significantly decreased levels of platelet BDNF in all the three headache groups considered, while platelet levels of NGF were significantly reduced in migraneurs but not in CH patients. No differences were found in the plasma levels of either neurotrophin, raising the possibility that mechanisms related to the production and/or compartimentalization, rather than the release of the neurotrophins, may be involved.
Several lines of evidence suggest that platelet function is altered in migraine as well as CH patients. Human blood platelets are the cellular elements with the highest content of 5-HT, which is taken up from plasma, stored in dense bodies and, upon release, exerts a pronounced vasomotor activity. Consequently, platelets have long been implicated as important contributors to the peripheral (i.e. vascular) 5-HT pathogenic component of migraine headache (2). Indeed, a number of studies have reported ongoing disturbances in systemic 5-HT homeostasis of migraneurs examined during headache-free periods (16), findings in line with our present observations showing increased intraplatelet levels of both 5-HT and 5-HIAA in the interictal phases of migraine and CH. On the other hand, there is also evidence that platelets are the main reservoir of circulating BDNF, the content of which we found to be markedly diminished in both migraineurs and CH sufferers, in contrast to 5-HT and 5-HIAA. Since BDNF, unlike 5-HT, is internalized in α granules (15), this, together with evidence of an abnormal platelet α granule secretion of β-thromboglobulin and platelet factor 4 in the headache-free phase of migraine and CH (21–24), raises the possibility that the observed reduction of BDNF content may reflect a preactivation state of these cells in primary headache patients. However, the fact that the decrease in platelet neurotrophins is not accompanied by an increase of their plasma levels does not fully support such a possibility. Also of note, we found, to our knowledge for the first time, that human platelets contain measurable levels of NGF. Although further studies are needed to determine whether circulating NGF storage processes within platelets follows steps analogous to 5-HT and BDNF, our results show a reduced intraplatelet NGF only in migraneurs and not in CH patients compared with controls. Again, we could not find any significant difference in plasma levels of NGF.
An alternative possibility is that the diminished levels of neurotrophins within platelets may reflect a decrease of their production in the periphery, e.g. BDNF production by vascular endothelial cells (25), as well as by other alternative sources, including pituitary gland and hypothalamus (26–28). Interestingly, BDNF and 5-HT production are intimately connected, at least in the CNS. This, together with our results showing concomitant occurrence of elevated levels of 5-HT and diminished levels of BDNF within the platelets of all three groups of primary headache patients, raises the question of whether a similar interplay also occurs in the periphery. On the other hand, primary headache patients may carry polymorphisms of the genes encoding for neurotrophins which may affect either their expression or release from the peripheral cellular sources. Although, to our knowledge, no polymorphism for NGF has been detected so far, a BDNF polymorphic variant (BDNFMet) determining quantitative decreased secretion of BDNF from neurons has recently been described (29). Moreover, humans heterozygous for BDNFMet were shown to have memory impairments (30), thus raising the possibility that this or other polymorphic variants may be of clinical interest in headache and other pain disorders (8). Further studies of these issues are nevertheless warranted.
Given the role of neurotrophins in activity-dependent plasticity of pain processing pathways in adulthood, it is tempting to speculate that our findings may reflect adaptive changes involved in peripheral and/or central sensitization mechanisms accompanying headache pathophysiology. However, although peripheral NGF is thought to contribute to the sensitization of nociceptors (4), other evidence points to a role of BDNF in plasticity and function of pain processing pathways solely in the CNS (8). In addition, little is known about the function of BDNF in the periphery. Notwithstanding this, our findings raise the possibility that primary headache patients are characterized by disturbances in neurotrophin-related processes, the further study of which may be of relevance for the better understanding of the complex pathophysiological mechanisms involved in primary headache disorders. In this regard, it is intriguing that we did not observe a reduction of platelet NGF in CH patients, in whom the hypothalamus, an important source of circulating NGF, plays a prominent role (31). Also of note is that, at least in rodents, circulating BDNF levels are positively correlated with cortical BDNF levels (32). Moreover, there is evidence that psychosocial stress markedly affects NGF and BDNF levels both in plasma and selected brain areas (33), and human platelets have been suggested to behave as peripheral markers of BDNF alterations in the CNS (34). The latter hypothesis is sustained by recent studies reporting a reduction of circulating BDNF in patients with depression (35), a psychiatric disorder which, interestingly, shows a high comorbidity with primary headaches, especially migraine (36).
In summary, our results favour the hypothesis of the occurrence of neurotrophin homeostasis alterations in the periphery of subjects affected by primary headache. Although further studies are necessary to define the specificity of our findings with regard to primary headache vs. other pain disorders, our results nevertheless show that platelet neurotrophins have the potential to be relevant biological markers for the study and clinical management of primary headache disorders.
Footnotes
Acknowledgements
This work has been supported by grant no. ICS030.9 of the Italian Ministry of Health (Ricerca Corrente), and by grant no. 3933 of the Italian Ministry of Education, University and Research (MIUR). A special note of appreciation to the ‘Antonio R. Cananzi Association for Headache and Cerebrovascular Diseases’.