
Abstract

Cluster Headache (CH) is a primary disorder defined by the International Headache Society (IHS) classification (1) as severe, unilateral orbital, supra-orbital, or temporal pain lasting 15–180 min if untreated and associated to signs of dysfunction of the autonomic nervous system such as conjunctival injection, nasal congestion, lacrimation, Horner's sign, and rhinorrhea. The attack frequency is ranged from one every other day to eight per day. In recent years several cases have been described concerning patients having cluster-like syndromes associated with intracranial pathologies, usually showing atypical manifestations with respect to the above mentioned diagnostic criteria (2). We report the case of a female patient affected by cluster-like headache completely fulfilling IHS diagnostic criteria, at least at presentation, who during the course of the illness presented clinical and neuro-imaging aspects of an organic brain lesion, e.g. a cavernous sinus metastasis.
Case history
A 60-year-old woman presented with a 3-week history of daily headache. The attacks occurred once daily during the night at the same hour (about 0400h) awakening the patient, and lasted 30–90 min. The pain was severe or excruciatingly severe and strictly localized on the left side and in the temporal region. The attacks were accompanied by ipsilateral lacrimation, conjunctival injection, rhinorrea and, occasionally, ptosis. Prior to the onset of the symptoms the patient was otherwise well, had never suffered from headache and did not take any medication. No familial history of headache disorder was reported.
On the initial neurological examination, the only finding was a mild left eyelid ptosis, interpreted as a partial Bernard-Horner sign, frequently recurring in CH patients during the active period (3). The physical examination was unremarkable. In particular, a tender superficial temporal artery was not found and neck movement were within the normal range. Blood-count, ESR, glycaemia, TSH and antinuclear antibodies were normal or negative. A brain and orbit CT with administration of contrast material was required because of the relatively advanced age of the patient, and the result was normal. A diagnosis of cluster headache was made and the patient was administered prednisone, 50 mg/daily.
Two weeks later the patient reported the almost complete remission of the pain. Nevertheless intermittent diplopia developed and eyelid ptosis was more pronounced. Furthermore, a few days earlier the patient had started to suffer from low-back pain. Neurological examination discovered a slight left midriasis and a paresis of left medial right muscle, in addition to the previous left eyelid ptosis. A brain MRI disclosed a iso/hyperintense area in the anterior aspect of left cavernous sinus, significantly enhanced by contrast material, consistent with a possible metastatic lesion (Fig. 1). In a few days ptosis became complete and the low back pain worsened. The patient was admitted to hospital. Spine X-ray and total-body CT scan disclosed the presence of diffuse bone and liver metastasis. A CT-guided liver biopsy was performed and the histological examination revealed metastasis from non-differentiated carcinoma of unknown origin. The patient died 35 days after the onset of symptoms. Autopsy was not performed.
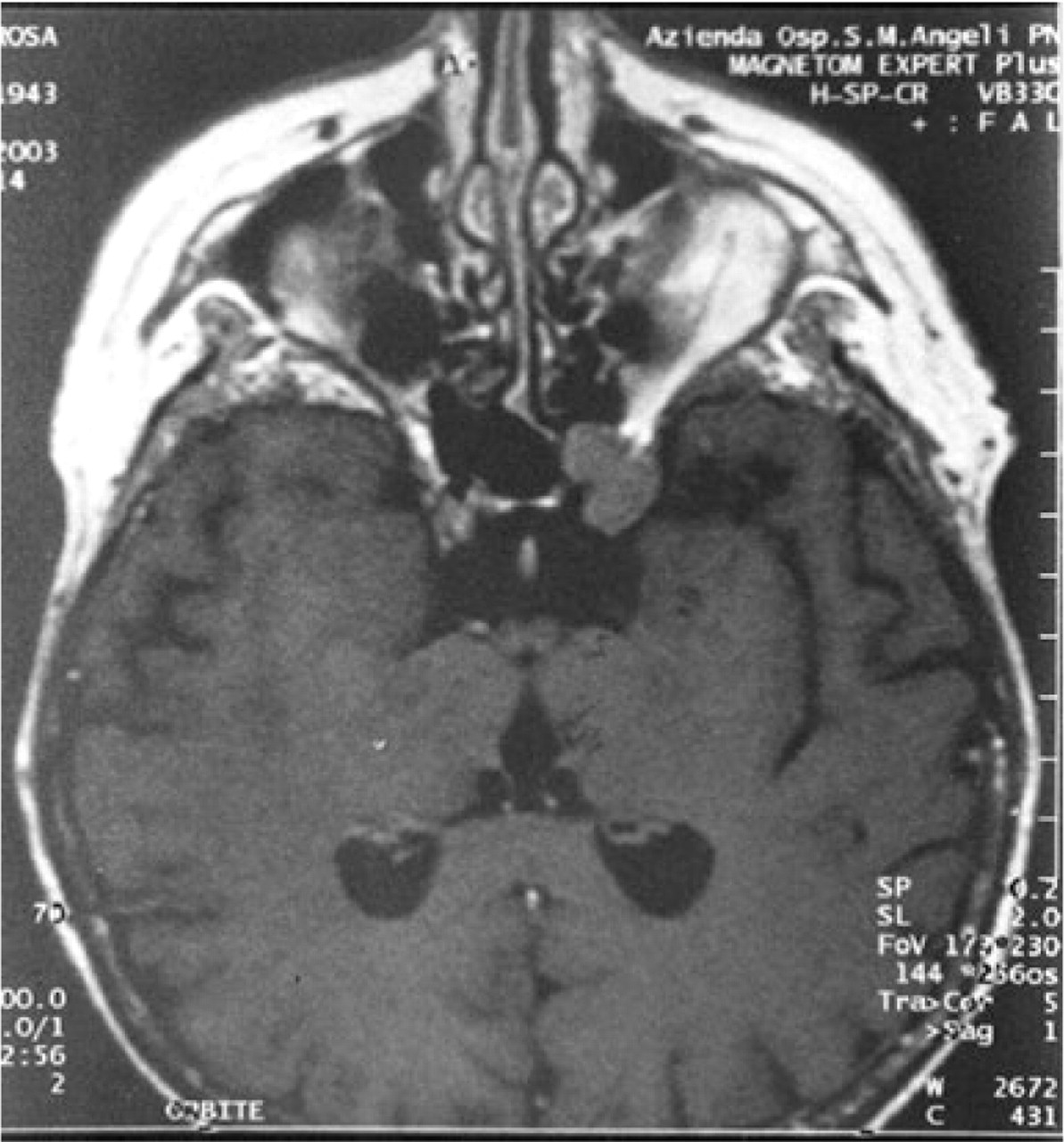
Post-gadolinium, T1 weighted MRI axial image shows an iso/hyperintense area in the left cavernous sinus significantly enhanced by contrast material.
Discussion
Our patient showed, at least for the first three weeks, a clinical picture indistinguishable from primary CH. The attacks occurred with a high regularity, in an ‘alarm-clock’ fashion, and were completely abolished by corticosteroid therapy. During the fourth weeks, when diplopia increased, the symptomatology assumed the aspect of a possible secondary cluster-like syndrome.
Increasing evidence indicates that pain and autonomic symptoms typical of CH result from the activation of trigeminal vascular and cranial parasympathetic pathways. Values of calcitonin gene-related peptide (CGRP) and vasoactive intestinal peptide (VIP), markers for, respectively, trigeminal vascular and cranial parasympathetic systems are increased in the external jugular vein blood during attacks (4). According to present theory, involvement of the ophthalmic division of the trigeminal nerve would provoke pain in the periorbital region and reflex activation of parasympathetic fibres arising in the superior salivatory nucleus leading to excessive gland secretion (lacrimation, nasal congestion, and eye injection), and dilation of internal carotid artery. Sympathetic dysfunction (the Horner's syndrome of miosis and ptosis) could be secondary to the compression of fibres arising in the superior cervical ganglion over dilated carotid wall.
Circadian and circannual rythmicities of CH are thought to be the product of a hypothalamic dysfunction (5), with a secondary involvement of the trigemino-autonomic pathways, as demonstrated by PET studies describing a unilateral activation in the hypothalamic grey matter ipsilateral to the headache side (6).
Our case of secondary CH indicates that an organic lesion in the anterior aspect of the cavernous sinus presumably involving the first division of the trigeminal nerve could have triggered the trigeminal autonomic hypothalamic circuitry. We are not sure that the pain was interrupted by the prednisone therapy or by the advancing of the metastatic lesion with a consequent injury of trigeminal sensory fibres. If the second option was true it would indicate the relative importance of integrity of the fifth nerve fibres in determining the pain.
Although primary CH may persist after trigeminal nerve root section (7), and recent papers indicate that CH is generated primarily from within the brain (5) rather than peripherically (8, 9), it is probable that in secondary CH, in predisposed individuals, a lesion located nearby the pain-sensitive pathways in the cavernous sinus or elsewhere (10–12) might trigger a brain-stem activation.
Other patients affected by CH secondary to a diverse variety of intracranial structural abnormalities involving the cavernous sinus had been described (13–16). Most patients, such as ours, developed during the course of the illness clinical signs atypical for primary CH, mostly a background pain and/or external ophthalmoplegia (2).
Most patients responded dramatically to corticosteroid. In those patient in whom the cerebral lesion could been removed the pain syndrome improved or ceased.
CH is a well defined primary headache syndrome with a peculiar clinical picture that allow an easy diagnosis in a relatively high percentage of cases. Nevertheless, it must be remembered that a cluster-like syndrome could be the consequence of a structural brain injury involving primarily the cavernous sinus and the trigeminal autonomic complex. Secondary CH often displays a clinical picture closely resembling that of idiopathic form, and share with primary CH a good response to corticosteroid. The presence of even minimal unusual aspects must prompt the clinician to seek a secondary cause of CH. In such cases, especially when CH starts in the elderly, proper neuroradiological investigation is mandatory.